










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.61 no.2 Cape Town 2023
http://dx.doi.org/10.36303/SAJS.3962
BREAST SURGERY
Sentinel lymph node biopsy in a resource-limited setting: a retrospective comparison of sentinel lymph node biopsy before and after the introduction of Sentimag at an academic breast unit
M YousefI; L RoodtII; A MasuIII; D NelIV; F MalherbeII
IDepartment of Surgery, University of Cape Town, South Africa
IIBreast and Endocrine Unit, Division of General Surgery, Groote Schuur Hospital, University of Cape Town, South Africa
IIIDepartment of Statistics, University of Cape Town, South Africa
IVDivision of General Surgery, Groote Schuur Hospital, University of Cape Town, South Africa
ABSTRACT
BACKGROUND: Sentinel lymph node biopsy (SLNB) is performed for staging and prognostication of breast cancer (BC) in cases with a clinically and radiologically negative axilla. Using blue dye and a radioactive colloid injection is considered the gold standard for SLNB. This study aims to evaluate the SLNB outcomes before and after the introduction of Sentimag at an academic breast unit. Sentimag uses an injection of superparamagnetic iron oxide which is then detected in the sentinal lymph node using a magnetometer
METHOD: A retrospective cohort study was performed comparing SLNBs done from 1 January 2017 to 31 December 2018. During 2017, a nuclear medicine technique was used for all SLNBs, while the Sentimag system was used in 2018
RESULTS: There was no difference between the two groups comparing age, T-stage, size of tumour, and molecular status. The only statistically significant difference found was more higher-grade tumours in the group where a nuclear medicine technique was used in 2017 (p = 0.04). There was no difference in the type of surgery performed comparing mastectomy and breast-conserving surgery rates between the two groups. There was an 11% increase in the number of patients who had an SLNB done with the Sentimag technique (2018). In 2017, 42% (58/139) had an SLNB and in 2018, 53% (59/112) had an SLNB
CONCLUSION: This result demonstrates the feasibility of the magnetic technique for SLNB in a resource-limited setting. This new method shows promise as a safe and effective technique for SLNB - it is a valuable alternative in the absence of nuclear medicine (N.Med) facilities
Keywords: breast cancer, sentinel lymph node biopsy, Sentimag, nuclear medicine
Introduction
Cancer is increasing worldwide and in low- to middle-income countries (LMICs), the mortality rate is higher than that of high-income countries (HICs).1 Studies estimate that by 2035, developing countries will harbour two-thirds of the new cancer cases.2 This projected increased burden of disease in LMIC demands that breast units are able to provide up-to-date surgical treatment of the axilla in women with early breast cancer (BC).
Sentinel lymph node biopsy (SLNB) is a tool that is widely used to stage patients who have a clinically and radiologically negative axilla. Using blue dye and a radioactive colloid injection is considered the gold standard for SLNB.3,4 Using either blue dye or radioactive colloid injection individually leads to a detection rate of 85.6%, while using them together achieves a 96% detection rate.5 Nuclear medicine techniques have several drawbacks, including radiation exposure, nuclear medicine unit dependency and legislative control accompanying the use of radiopharmaceuticals. Hence, it is only available in centres with an active N.Med department. An injectable magnetic tracer has become available, and it can be used as an alternative to SLNB. The magnetic tracer is a sterile aqueous suspension of superparamagnetic iron oxide (SPIO) particles with brownish colour that accumulate in the sentinel lymph nodes. This build-up is then identified using a handheld magnetometer (Sentimag®).6 The main advantage of Sentimag is that this technique is independent of N.Med centres which are only available in large academic hospitals beyond the reach of many women with BC.
The study was conducted at Groote Schuur Hospital (GSH), an academic hospital in South Africa. GSH provides a centralised diagnostic BC clinic and multidisciplinary team (MDT) management for all patients diagnosed with BC in the western part of Cape Town. An average of 550 new patients with BC have been diagnosed between 2014 to 2017, with approximately 60% of the patients experiencing early BC.7 The unit has used a nuclear medicine technique to identify sentinel lymph nodes since 2001. In January 2018, the nuclear medicine technique was replaced by Sentimag for all SLNBs.
The study aimed to evaluate the SLNB outcomes of the newly introduced Sentimag technique in comparison to the standard nuclear medicine technique.
Methods
A retrospective cohort study, which included all patients meeting the inclusion criteria managed by the GSH/ University of Cape Town Breast Surgery Unit MDT, from 1 January 2017 to 31 December 2018, was undertaken. The sample population was divided into two groups for comparison. The first group, named 'N.Med', consisted of all patients who had surgery in 2017 and had an SLNB using a radioisotope, while the second group, named "Sentimag", consisted of patients who had surgery in 2018 and had an SLNB using SPIO.
The data were retrospectively collected from patient notes, digital and paper records. The inclusion criteria were female patients, age 18 or older, who had breast surgery and axillary surgery for BC at GSH and surrounding referral hospitals (New Somerset Hospital, Mitchells Plain Hospital and Victoria Hospital). Patients with ductal carcinoma in situ were included if they had axillary surgery. Patients were excluded from the study if they received neoadjuvant chemotherapy, had no axillary surgery, had non-epithelial BC, or had incomplete records.
For sentinel node localisation, patients receiving a nuclear medicine SLNB were injected with a radioactive tracer (99mTc) the day before surgery. The injection was made subareolar in patients with non-palpable tumours and subcutaneously above the tumour in patients with palpable tumours. Lymphoscintigraphy was routinely performed, and the hottest node was marked on the skin of the axilla in the nuclear medicine department the day before surgery, as per local protocol. The timing and mode of administration of radioisotope were documented in the clinical records. Sentinel nodes were detected intraoperatively using a gamma probe. The magnetic technique was standardised for patients receiving a Sentimag SLNB. However, at set-point or zero-point, the Sentimag device tends to drift thereby requiring regular recalibration in the process. The operating surgeon injected a 5 ml solution, consisting of 2 ml of the magnetic tracer Sienna+ (Sysmex Europe GmBH, Hamburg, Germany ) diluted with 3 ml of normal saline, into the retroareolar subcutaneous space. The solution was injected preoperatively the day before surgery. During surgery, the surgeon used a handheld magnetometer Sentimag® (Sysmex Europe GmBH, Hamburg, Germany) for skin localisation of the sentinel lymph node.
After incision, the surgeon removed all metal instruments from the operative field and replaced them with plastic retractors and forceps before the handheld magnetometer was used for sentinel node localisation. Excision of nodes with the handheld magnetometer was undertaken by using the same cut-off as used for the gamma probe, that is, any node with 10% or highest count was excised. Beyond four sentinel nodes, surgeons noted the background count and excised additional nodes at their discretion. Any palpable nodes were also removed. All nodes were examined with haematoxylin-eosin staining on paraffin-embedded specimens.
The data were analysed using STATA v14. Numerical data were summarised as means and medians and categorical data were summarised as proportions. A t-test was used to compare means and a Wilcoxon Rank sum test was performed to compare medians. For categorical data, a Fisher's exact test or a chi-squared test was used as appropriate. A level of significance was set at a two-sided _p-value of 0.05.
Results
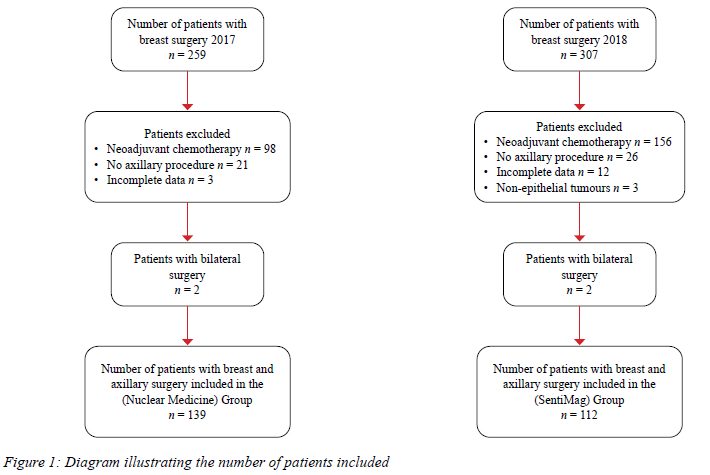
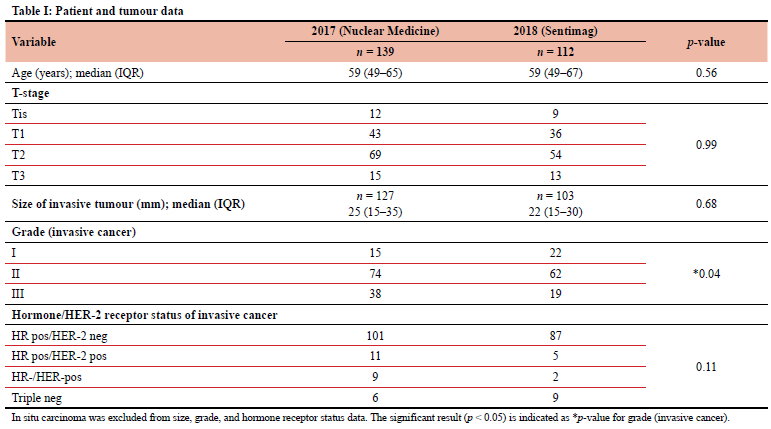
After excluding patients not meeting the inclusion criteria and including patients who had bilateral surgery, 140 axillary procedures were performed in 2017 and 112 in 2018 as shown in Figure 1. Patients with bilateral breast cancer had their axillae counted separately. The description of the two groups of patients is represented in Table I. The analysis found no statistical difference between the two groups comparing age, T-stage of tumours, size of an invasive tumour or molecular status of the cancers. However, there was a statistical difference in the grade of the tumours, with more high-grade tumours in the N.Med group (p = 0.04).
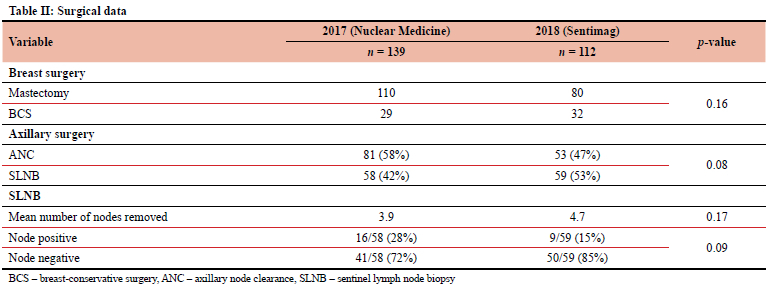
The two groups were also compared in terms of surgical data (Table II). There was no difference in the type of breast or axillary surgery between the two groups. There was an 11% difference in the number of patients receiving an SLNB, with more patients receiving SLNBs after 2018 - the results did not reach statistical significance. The results did not show a statistically significant difference between the two groups comparing the number of nodes removed when doing an SLNB (p = 0.17).
Discussion
Sentinel node biopsy was first reported in the 1990s as an attempt to decrease the number of patients with no axillary metastasis undergoing an axillary lymph node dissection (ALND).8 This is overtreatment of the axilla and must be avoided to limit the complications such as lymphoedema and sensory nerve deficits that can occur after ALND.9 Unfortunately, the current gold standard technique in SLNB, using an N.Med tracer and a gamma probe, is not widely available due to resource constraints in LMICs.10 Only 13 (24%) countries, mainly in the north and south of Africa have more than one facility.11 Therefore, new technologies with equivalent efficacy are constantly being researched to offer SLNB without depending on a nuclear medicine department. Sentimag is the most promising of the new technologies available and is already widely used around the world.
Several non-inferiority trials have been published in Europe comparing SPIO to a radioisotope. In 2013, a study by Douek et al.3 on 160 women with BC scheduled for SLNB who were clinically and radiologically node negative found that the identification rate was 95% (152/160) with the standard technique and 94.4% (151/160) with the magnetic technique. Two hundred and ninety-seven (297, 74 %) were true sentinel nodes.3 In many European studies,12-17 the findings of Douek have been verified. The results showed a detection rate per patient of 97.3% (146/150) for (99m) Tc vs 98% (147/150) for SPIO. These results indicate that SLNB using the magnetic technique can be performed easily, safely and equivalently in comparison to the radiotracer method.11 Pinero-Madrona et al.13 also compared the magnetic to a nuclear medicine technique for the detection of SLNs. They found that transcutaneous and intraoperative detection rates were 95.5% vs 97.2%, and 97.2% vs 97.8% for Sentimag and gamma probe respectively (concordance rates > 97%). At the node level, intraoperative and ex vivo detection rates were 92.5% vs 89.3% and 91.0% vs 86.3% for SM and GP, respectively.
Non-inferiority was proven comparing Sentimag to the gamma probe.13 The French Sentimag feasibility trial evaluated the localisation of BC SLN using SPIO particles in comparison to the standard technique (isotopes ± blue dye). They reported an SLN identification rate of 98.1% for both methods, 97.2% for Sienna+®, and 95.4% for the standard technique. The concordance rate was 99% per patient and 97.4% per node. The provision of Sienna+® tracer has been found to cause skin discolouration (grey-brown bruise) in many patients.13 This effect causes discomfort in patients, and it perseveres for up to 24 months before complete disappearance.14 Forty-six patients (43.4%) had nodal involvement. Among involved SLNs, the concordance rate was 97.7% per patient and 98.1% per node.15 Rubio et al.15 assessed the concordance between SPIO and the Tc 99 radiotracer. The detection rate by Tc 99 was successful in 113 (95.7%) of patients and by SPIO in 116 (98.3%). Concordance rates per patient between the techniques was 98.2%. The SLN was positive in 36 (30%) of patients. Of this, SLN positivity was detected by both techniques in 32 patients which indicates that detection of SLNs with SPIO allows for easy identification of axillary nodes, at a frequency not inferior to the radiotracer.17 Karakatsanis et al.,16 in the Nordic Sentimag trial, compared the efficacy of SPIO as a tracer with Tc 99 and patent blue, and reported that SN detection rates were similar between standard technique and SPIO both per patient (97.1 vs 97.6%, p = 0.76) as well as per node (91.3 vs 93.3 %, p = 0.34). These findings were not affected by the presence of malignancy. Concordance rates were also consistently high (98% per patient and 95.9% per node).18 Although, not statistically significantly different, the current study demonstrates an increase in the number of patients who had an SLNB after the introduction of Sentimag. There was an 11% increase in the number of patients who had an SLNB done after the introduction of Sentimag. The N.Med Department at GSH restriction on the availability of lymphoscintigraphy limited the amount of SLNBs performed on a surgery list to two. This limitation in access to N.Med compelled surgeons at GSH to perform an ALND on patients with a clinically node negative axilla. The Sentimag technique allowed the surgeons to increase the number of sentinel node biopsies without the need for N.Med facilities (availability of radiopharmaceuticals). Lack of access to N.Med facilities makes new SLNB techniques without using radiopharmaceuticals an attractive alternative. This study, therefore, confirms findings from the literature that SPIO is easier to use without the restrictions in availability, use, manipulation and disposal of radiopharmaceuticals.13,14,19,20
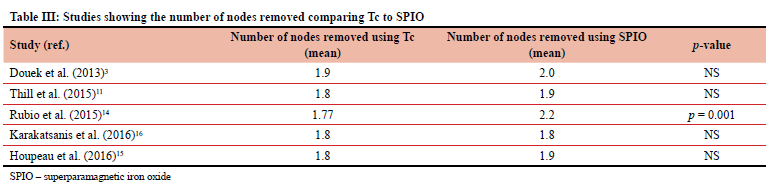
Other than access to a nuclear department, the cost of the equipment needed to implement an SLNB service is one of the main factors hampering the establishment of an SLNB service in developing countries. It appears that no cost analysis has been done to compare Sentimag to an N.Med technique. There is initial capital that needs to be spent to acquire the detection equipment for both procedures. The cost of SPIO when compared to radiopharmaceuticals is similar. Man et al.21 reported that all the following needs to be accounted for in calculating the cost of an N.Med SLNB service; day admission for injection of the radiopharmaceutical, specially arranged specimen transportation as per local risk management protocol, annual on-site contamination tests and monthly calibration of pocket dosimeters all at extra cost. They estimated that by using SPIO alone, $22 300 per year can be saved compared to radiopharmaceuticals.21 Our study did not show a higher nodal retrieval rate between the nuclear medicine and Sentimag groups. The mean number of nodes removed using the nuclear medicine technique was 3.9 compared to 4.7 (p = 0.17) in the patients who had the magnetic procedure. These results are in concordance with current literature: many authors found that SLNB using SPIO resulted in a similar number of nodes retrieved compared to radioisotope. However, Rubio et al.16 retrieved more nodes in the SPIO group as shown in Table III.
The current study did not demonstrate why more nodes were harvested using the Sentimag procedure. Rubio et al.16 speculated that it could be explained by a learning curve using the new tracer agent. The Sentimag technique is different from the nuclear medicine technique in that plastic instruments must be used during the time the magnetometer is used to prevent interference. Another reason for the increase in the number of lymph nodes removed could be nonuniformity in the size of the tracer particles with varying uptake of tracer by other axillary nodes.
The major limitation of this study is the retrospective nature of data collection which can lead to selection bias. Of importance is the comparison of the Sentimag, the new technique, with the established radionuclear methodology. Further studies are needed to add to the considerable amount of data supporting Sentimag as a viable alternative to conventional methods.
Conclusion
This study demonstrated the feasibility of the magnetic technique for SLNB in a resource-limited setting. The results from this study, along with the accumulating evidence from the literature, are practice changing. This new method shows promise as a safe and effective technique for SLNB. It is a valuable alternative in the absence of N.Med facilities.
Acknowledgements
I remain thankful to Dr Francois Malherbe, Dr Liana Roodt, Dr Daniel Nel and Dr Mohamed Almoslemany for their significant inputs in ensuring coherent results. Also, I am very grateful to all my colleagues at the Department of Surgery, University of Cape Town, for their contributions during the study. Special appreciation goes to Groote Schuur Hospital for making this study a reality.
Conflict of interest
The author declares no conflict of interest.
Funding source
No funding was required.
Ethical approval
The author hereby declares that this study is his original work and has not been submitted for publication elsewhere in part or as a whole. Ethical approval for the study was received from the Human Research and Ethics Committee of the University of Cape Town (HREC number 199\2019).
ORCID
M Yousef https://orcid.org/0000-0003-3604-6847
F Malherbe https://orcid.org/0000-0001-8910-6925
D Nel https://orcid.org/0000-0002-3265-1049
L Roodt https://orcid.org/0000-0002-0545-5413
REFERENCES
1. DeSantis CE, Bray F, Ferlay J, et al. International variation in female breast cancer incidence and mortality rates. Cancer Epidemiol Biomarkers Prev. 2015;24(10):1495-506. https://doi.org/10.1158/1055-9965.EPI-15-0535. [ Links ]
2. Tefferi A, Kantarjian H, Rajkumar SV, et al. In support of a patient-driven initiative and petition to lower the high price of cancer drugs. Mayo Clin Proc. 2015;90(8):996-1000. https://doi.org/10.1016/j.mayocp.2015.06.001. [ Links ]
3. Douek M, Klaase J, Monypenny I, et al. The Sentimag multicentre trial: Sentinel node biopsy using a magnetic technique versus the standard technique. Eur J Surg Oncol. 2013;39(11):S85-S86. https://doi.org/10.1016/j.ejso.2013.07.124. [ Links ]
4. Lyman GH, Giuliano AE, Somerfield MR, et al. American Society of Clinical Oncology guideline recommendations for sentinel lymph node biopsy in early-stage breast cancer. J Clin Oncol. 2005;23(30):7703-20. https://doi.org/10.1200/JCO.2005.08.001. [ Links ]
5. Teshome M, Wei C, Hunt KK, et al. Use of a magnetic tracer for sentinel lymph node detection in early-stage breast cancer patients: a meta-analysis. Ann Surg Oncol. 2016;23(5):1508-14. https://doi.org/10.1245/s10434-016-5135-1. [ Links ]
6. Douek M, Klaase J, Monypenny I, et al. Sentinel node biopsy using a magnetic tracer versus standard technique: the Sentimag Multicentre Trial. Ann Surg Oncol. 2014;21(4):1237-45. https://doi.org/10.1245/s10434-013-3379-6. [ Links ]
7. Cairncross L, Panieri E, Anderson D, et al. Expanding breast cancer care through partnerships and innovation: experience from a South African public hospital. S Afr Health Rev. 2019;2019(1):105-13. [ Links ]
8. Krag DN, Weaver DL, Alex JC, Fairbank JT. Surgical resection and radiolocalisation of the sentinel lymph node in breast cancer using a gamma probe. Surg Oncol. 1993;2(6):335-40. https://doi.org/10.1016/0960-7404(93)90064-6. [ Links ]
9. Brar P, Jain S, Singh I. Complications of axillary lymph node dissection in treatment of early breast cancer: a comparison of MRM and BCS. Indian J Surg Oncol. 2011;2(2):126-32. https://doi.org/10.1007/s13193-011-0078-2. [ Links ]
10. Brand NR, Wasike R, Makhdomi K, et al. Sentinel lymph node biopsy pathology and 2-year postsurgical recurrence of breast cancer in Kenyan women. J Glob Oncol. 2018;4:1-7. https://doi.org/10.1200/JGO.17.00111. [ Links ]
11. Grigoryan A, Bouyoucef S, Sathekge M, et al. Development of nuclear medicine in Africa. Clin Transl Imaging. 2021:111. [ Links ]
12. Thill M, Kurylcio A, Welter R, et al. The Central-European Sentimag study: Sentinel lymph node biopsy with superparamagnetic iron oxide (SPIO) vs. radioisotope. Breast. 2014;23(2):175-9. https://doi.org/10.1016/j.breast.2014.01.004. [ Links ]
13. Pinero-Madrona A, Torró-Richart J, De León-Carrillo J, et al. Superparamagnetic iron oxide as a tracer for sentinel node biopsy in breast cancer: a comparative non-inferiority study. Eur J Surg Oncol (EJSO). 2015;41(8):991-7. https://doi.org/10.1016/j.ejso.2015.04.017. [ Links ]
14. Lorek A, Stojcev Z, Zarebski W, Kowalczyk M, Szyluk K. Analysis of postoperative complications after 303 sentinel lymph node identification procedures using the Sentimag® method in breast cancer patients. Med Sci Monit. 2019;25:3154-60. https://doi.org/10.12659/MSM.912758. [ Links ]
15. Houpeau JL, Chauvet MP, Guillemin F, et al. Sentinel lymph node identification using superparamagnetic iron oxide particles versus radioisotope: the French Sentimag feasibility trial. J Surg Oncol. 2016;113(5):501-7. https://doi.org/10.1002/jso.24164. [ Links ]
16. Rubio I, Diaz-Botero S, Esgueva A, et al. The superparamagnetic iron oxide is equivalent to the Tc99 radiotracer method for identifying the sentinel lymph node in breast cancer. Eur J Surg Oncol (EJSO). 2015;41(1):46-51. https://doi.org/10.1016/j.ejso.2014.11.006. [ Links ]
17. Lopez-Gobernado M, Perez-Rubio A, Lopez-Garcia E, Eiros JM. Data collection and microbiological monitoring in global tuberculosis intervention. Arch Bronconeumol. 2019;55(7):395-6. https://doi.org/10.1016/j.arbr.2019.01.003. [ Links ]
18. Karakatsanis A, Christiansen PM, Fischer L, et al. The Nordic Sentimag trial: a comparison of super paramagnetic iron oxide (SPIO) nanoparticles versus Tc (99) and patent blue in the detection of sentinel node (SN) in patients with breast cancer and a meta-analysis of earlier studies. Breast Cancer Res Treat. 2016;157(2):281-94. https://doi.org/10.1007/s10549-016-3809-9. [ Links ]
19. Pouw JJ, Ahmed M, Anninga B, et al. Comparison of three magnetic nanoparticle tracers for sentinel lymph node biopsy in an in vivo porcine model. Int J Nanomedicine. 2015;10:1235-43. https://doi.org/10.2147/IJN.S76962. [ Links ]
20. Rescigno J, Zampell JC, Axelrod D. Patterns of axillary surgical care for breast cancer in the era of sentinel lymph node biopsy. Ann Surg Oncol. 2009;16(3)687-96. https://doi.org/10.1245/s10434-008-0195-5. [ Links ]
21. Man V, Wong TT, Co M, Suen D, Kwong A. Sentinel lymph node biopsy in early breast cancer: magnetic tracer as the only localising agent. World J Surg. 2019;43(8):1991-6. https://doi.org/10.1007/s00268-019-04977-1. [ Links ]
 Correspondence:
Correspondence:
M Yousef
Email: mazz377@gmail.com


{kind=link}
{kind=link}
{kind=link}
{kind=link}