










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Surgery
versión On-line ISSN 2078-5151
versión impresa ISSN 0038-2361
S. Afr. j. surg. vol.61 no.1 Cape Town 2023
http://dx.doi.org/10.36303/SAJS.3811
SURVEY
South African surgical trainees Master of Medicine dissertation survey
M BarnardI; BS JacksonII
IDepartment of General Surgery, University of Pretoria, South Africa
IIEndocrine and Trauma Unit, Kalafong Provincial Tertiary Hospital, Department of General Surgery, University of Pretoria, South Africa
ABSTRACT
BACKGROUND: Since 2011, South African specialist registration requires a research component in the form of a Master of Medicine (MMed) degree. The aim of the study was to assess opinion regarding research and the progression and obstacles toward the completion of the research component of the MMed amongst South African surgical registrars
METHODS: One hundred and sixty-eight (24%) from 708 nationally registered surgical registrars participated. The participants completed an electronic survey that focused on research progression timeline, registrar research perspectives, factors affecting research success and obstacles, and interest in future research
RESULTS: There was an expected progression of research with increasing seniority. Forty-two (25%) started their research 6-12 months into their training time. One hundred and ten (66%) were confident their research would be completed timeously. Obstacles to timeous completion included clinical responsibilities with lack of protected research time in 130 (75%) and lack of funding in 46 (28%). From the registrars' perspective, their confidence to complete their research timeously was increased when they had attended a structured research course and had prior research experience
CONCLUSION: Completion of the MMed research component was considered to be hampered by a lack of dedicated time and funding and aided by prior research experience and a structured research training course
Keywords: research, surgical training, Master of Medicine research, surgical trainees, surgical education, postgraduate research, postgraduate education
Introduction
The introduction of structured research programmes amongst surgical trainees has changed the research culture towards evidence-based medicine.1,2 It aims to create critical thinking specialists with research appraisal skills.3 The American Surgical Society Blue Ribbon committee acknowledges that surgery's future depends on prioritising research.4 Furthermore, the Accreditation Council of Graduate Medical Education (ACGME) has identified medical knowledge as a core competency, making research an important addition to the general surgery curriculum.5 The Health Professions Council of South Africa (HPCSA) requirements for registrar research were introduced in 2011, in order to demonstrate trainee understanding of the research process.6 The research criteria consist of a submitted Masters of Medicine (MMed) minor dissertation which is completed in tandem with the 5-year surgical training programme.7,8 The surgical qualification/degree requires a successful result from the CMSA final examination (Fellowship of College of Surgeons) and a completed dissertation under the respective training university (MMed), which has been assessed by at least one external examiner.
The timeous completion of the dissertation component of the MMed is challenged by multiple obstacles during the surgical training period. One of the greatest obstacles for successful research remains lack of adequate time to conduct and complete a research project. In a multicentre survey amongst South African general surgery registrars, 87.9% reported lack of sufficient time as a major obstacle.9 This challenge was echoed in similar surveys from the African continent.10,11 In the United States, dedicated research time was established to address this obstacle, with 56.6% of American general surgery programmes offering dedicated research time, which may continue for 1-4 years.12 In this environment it is not uncommon to embark on a laboratory-based training programme for 1-3 years after completing 2 years of surgical training with over a third of American surgical residents choosing to interrupt clinical training to pursue a research fellowship.12 A survey amongst American urology trainees showed that 12 months of dedicated research time produced three times more resident manuscripts.13 Other benefits of dedicated research time have also found to be independently associated with faculty appointments and research grant awards.14 Some South African surgical training programmes offer limited protected research time, with 93.5% of surveyed general surgery registrars proposing dedicated research time as a potential solution.15
Lack of knowledge of research methodology can obstruct progression. Attending a research methodology course has shown to improve the quality of research.16 Competency of supervisors also influences research completion. The Committee for Higher Education (CHE) recommends that a supervisor should have an appropriate research record, ongoing research development and at least have a qualification at the level of the postgraduate programme.17 Delays in statistical support and approval from research committees, such as ethical approval, can also act as obstacles to completion. A South African university audit reported that data collection may have a cumulative delay of up to 4 months.18 Lack of funding poses another major obstacle to research amongst registrars in low-income countries with 20.2- 95% reporting lack of funds,9,15 and 80% funding their own research in some institutions.1
The obstacles at different stages of research, during the progression timeline to the registrar's final examination, have not been documented. Establishing a trend of progression and identifying obstacles and drivers of success may guide surgical training institutions to identify registrars who are failing to progress in their research. Unfortunately, there is a lack of data on the conduct of MMed research from training centres and therefore the ability to monitor the process and assess the effect of interventions is challenging. As a starting point this study aimed to assess the progression and obstacles toward the completion of the MMed research component as experienced by the registrars in training. This study is conducted as part of the South African Surgeons in Training (SASSiT) research initiative.
Methods
A nationwide cross-sectional survey was designed and categorised into surgical registrar: demographics, perspectives towards research, MMed research progression timeline, aspects of research success and obstacles. Topics were generated with guidance from existing literature9,19 highlighting facilitators and barriers to research success. From June to August 2020, questionnaires were distributed electronically via an online survey platform (www.SurveyMonkey.com) and social media registrar platforms to surgical registrars. The survey was voluntary and anonymous with no additional incentive, comprising of 23 questions. Questions were structured using a combination of 10 multiple-choice, one Likert scale, 11 yes- or no-type questions and one free text question. The programme's Internet Protocol (IP) address recognition prohibited registrars from duplication. Registrars from all surgical departments (general, orthopaedic, vascular, ear/nose/ throat, maxillofacial, cardiothoracic, urology and paediatric surgery) from the nine accredited South African surgical training universities were approached to participate. Demographic and descriptive data were categorical and described using frequencies and percentages. Ethical approval was obtained from the Human Research Ethics
Committee of the University of Pretoria, reference number 199/2020.
Results
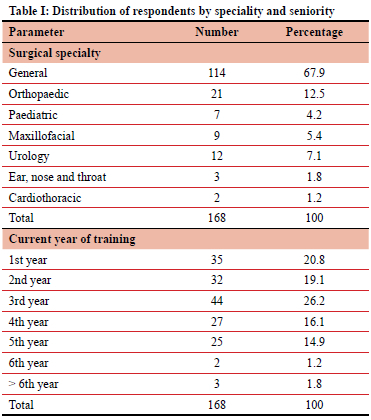
Of the 708 surgical registrars approached, 168 (24%) participated. The number of registrars per surgical subspecialty can be seen in Table I. One hundred and eleven (66%) were either in the first, second or third year of training. Five registrars had not completed their research within the five-year surgical training period, but their training time had been extended.
Research progression timeline
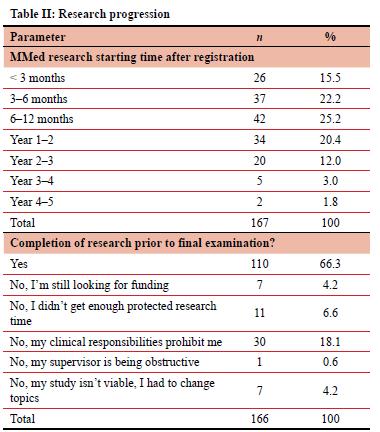
One hundred and five (63%) surgical trainees, started their MMed research within the first year of registrar training, with 42 (25%) starting between 6-12 months (Table II). Sixty-two of the registrars (37%) were at the stage of protocol development or awaiting MMed protocol and/or ethical committee approval. Twenty-three (13.7%) had not chosen a research topic. There were 56 (34%) registrars who did not see themselves completing their research within the specified timeline due to various reasons, including clinical responsibilities and lack of protected research time.
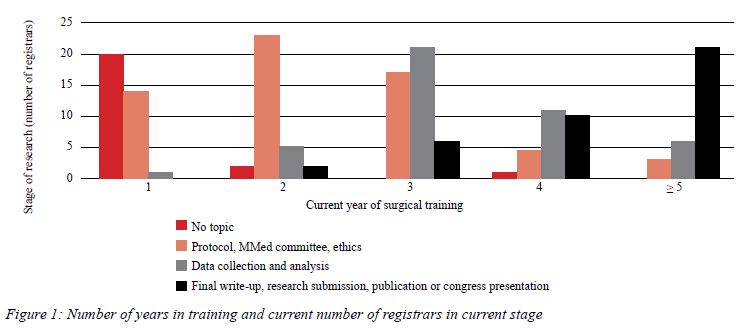
When comparing the number of years in training to current stage of research (Figure 1), the progression timeline can be appreciated as registrars increase in seniority. In the early training years, i.e., first and second year, registrars either had no research topic or were in their protocol development, awaiting MMed protocol and/or ethical committee approval phase. In the final years of training (5 or more years), 21/30 (70%) were in the final write-up, research submission, publication or congress presentation phase. However, not all registrars progressed as rapidly during the training period. The remainder of those in their final years had not yet achieved the final stages of research completion.
Research success and obstacles
Structured research training courses have been implemented in the majority of South African training universities, however 59 (35%) registrars reported that their university did not offer such a course (Table III). Regarding protected (or dedicated) research time during formal training, 130 (78%) registrars had no protected research time. However, 21/37 (56%) who had protected research time reported a positive impact on their research progression. Fifty-eight (35%) stated that they required funding. Forty-six (28%) registrars were not progressing with their research due to lack of funding.
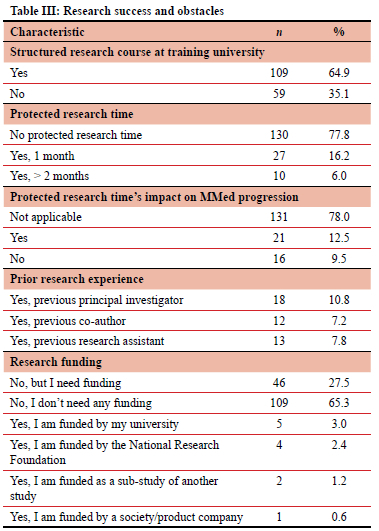
One hundred and twenty-four registrars (74%) had no research experience prior to registrar training, while 43 (26%) had been involved in some aspect of research. Forty-nine (29%) surgical registrars were concurrently involved in research other than their MMed (Table III).
One hundred and twenty-four (74%) registrars chose their supervisors. One hundred and forty-nine (89%) reported that their supervisors were involved with other research projects and 62 (37%) registrars agreed that this influenced their decision to choose such a supervisor.
Registrar perspectives
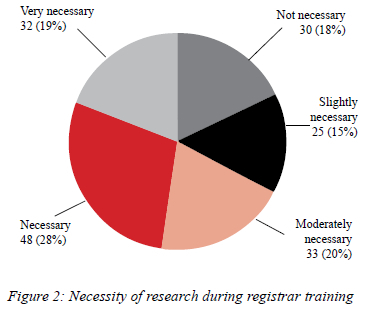
Registrar's perspectives on research necessity were assessed, as seen in Figure 2. Various degrees of necessity were acknowledged in 138 (82%) registrars, while 30 (18%) thought research was not necessary.
Registrars had more confidence in completing their research timeously depending on their current stage of research and if they had access to a structured research course. Eighty-one (74%) who were confident of timeous completion had also attended a research training course. Lack of protected research time, reported by 82 (75%), and lack of prior research experience, reported by 73 (67%), did not alter the registrars confidence in timeous completion.
Regarding research and clinical skills, 117 (70%) did not think research time affected their skills. Fifty-one registrars (30%) were of the opinion that the time spent on research resulted in a decline in their clinical skills.
With regard to future participation in research, 139 (83%) registrars plan to publish their MMed research upon completion. One hundred and eleven (66%) registrars were considering future participation in research after their formal training. Thirty-six (21%) planned to extend their research into a doctorate. Regarding research collaboration options with other institutions, 139 (83%) reported that they would consider collaboration if given the option.
Discussion
Despite the large majority of registrars starting their research within the first year of training, only 110 (66%) were confident that their research would be completed timeously. Clinical responsibilities with lack of protected research time and lack of funding were the most commonly reported obstacles to completing research. These obstacles are consistent with those outlined in previous reports.9,15
Clinical responsibilities remain the main obstacle preventing research completion. This is well mimicked in previous studies where the intrusion of clinical work (54%) was the main obstacle to research amongst senior registrars.20 Lack of time seems to be a common denominator as the majority of training centres did not have protected research time.9,15 Only 37 (22%) reported having formal protected time, of which only 21 (56%) felt it made a difference to research progression. These findings are inconsistent with centres from other countries that have longer periods allocated for dedicated research.12,13 Further investigations are required to determine the reasons and may include the timing of the allocated research period, limited allocated research time and incorrect use of the research time from what it was intended for.
Although the MMed dissertation was not intended to be an expensive undertaking, many research projects do require funding. Lack of funding was reported as an obstacle by 46 registrars (28%) who failed to progress due to lack of funds. There are established research collaborative efforts amongst high and lower-middle income countries.21 Collaboration of research allows for wider financial options, depth of research and division of workload. The majority of registrars (83%) stated that they were open to collaboration. This is well mimicked with high income counterparts where 92% of trainees were interested in international collaboration.22 Research collaborations may pool funding and resources as well as cement a fair partnership between different institutions.
Registrars with previous involvement in research tend to have an advantage compared to those without research experience. Most South African training universities offer a structured research training course lasting one week, providing skills to perform research. Implementation of a formal research curriculum as a part of general surgery residency training in the United States also showed a significant increase in resident presentations and higher trends for publications.23 Amongst registrars not confident that they will submit their research timeously, only 28 (50%) reported access to a structured research training course. A structured research course was considered by the registrars to enhance the likelihood of completing their research project.
Although a good researcher does not ensure a good supervisor, the research experience does allow a supervisor to be more prepared when guiding a registrar. However, supervisor experience did not significantly influence a registrar's choice of supervisor. The reason may be due to the unfamiliarity of registrars, especially if just entering the training programme, with specialists that may be good supervisors.
One of the concerns with increased research responsibilities is the interruption of clinical skill development. Dedicated research fellowships have shown moderate skills decay of difficult surgical procedures, such as bowel anastomosis and laparoscopic hernia repairs.24 In the opinion of 117 registrars (70%), time spent on research did not affect their surgical skills - a perception that is possibly due to the registrars not leaving clinical training for a dedicated research time. A balance has to be achieved in order to develop research skills without compromising clinical training.
This survey had the limitations of a moderate response rate of 24% and a heterogeneous surgical disciplines sample which compromised the representativity and conclusions of the study. Despite these limitations this survey provides an insight into the reality of the national situation regarding the MMed research component from a registrar's perspective. It is hoped that the findings will spur academic departments to collect real time data to monitor MMed progress. In the meantime, they should give consideration to the concerns found in this survey, namely a lack of dedicated research time and funding, and implement the introduction of a structured research programme.
Acknowledgements
We thank the South African Society of Surgeons in Training (SASSiT) for supporting this research. We also thank Professor PJ Becker, Research Office, University of Pretoria, South Africa, for assisting with the statistical analysis.
Conflict of interest
The authors declare no conflict of interest.
Funding source
SASSiT.
Ethical approval
Ethical approval for the study was granted by the Human Research Ethics Committee of the University of Pretoria (reference number: 199/2020).
ORCID
M Barnard https://orcid.org/0000-0003-3553-3846
BS Jackson https://orcid.org/0000-0001-8994-8575
REFERENCES
1. Habineza H, Nsanzabaganwa C, Nyirimanzi N, et al. Perceived attitudes of the importance and barriers to research amongst Rwandan interns and paediatric residents - a cross-sectional study. BMC Med Educ. 2019;19(1):1-8. https://doi.org/10.1186/s12909-018-1425-6. [ Links ]
2. Kanna B, Deng C, Erickson SN, et al. The research rotation:competency-based structured and novel approach to research training of internal medicine residents. BMC Med Educ. 2006;6:1-8. https://doi.org/10.1186/1472-6920-6-52. [ Links ]
3. Hebert RS, Levine RB, Smith CG, Wright SM. A systematic review of resident research curricula. Acad Med. 2003;78(1):61-68. https://doi.org/10.1097/00001888-200301000-00012. [ Links ]
4. Debas HT, Bass BL, Brennan MF, et al. American Surgical Association Blue Ribbon Committee report on surgical education: 2004. Ann Surg. 2005;241(1):1-8. https://doi.org/10.1097/01.sla.0000150066.83563.52. [ Links ]
5. Kang D, Siddiqui S, Weiss H, et al. Are we meeting ACGME core competencies? A systematic review of literature on international surgical rotations. Am J Surg. 2018;216(4):782-6. https://doi.org/10.1016/j.amjsurg.2018.07.048. [ Links ]
6. Rout C, Aldous C, Hift R. Response to concerns expressed in the journal regarding the HPCSA requirement for registrar (MMed) research. J Anaesth Analg. 2018;24(2):48-49. [ Links ]
7. The Colleges of Medicine South Africa. Regulations for admission to the fellowship of surgeons of South Africa FCS(SA); September 2019. Available from: www.cmsa.co.za. Accessed 28 Aug 2020. [ Links ]
8. Degiannis E, Oettle GJ, Smith MD, Veller MG. Surgical education in South Africa. World J Surg. 2009;33(2):170-3. https://doi.org/10.1007/s00268-008-9815-2. [ Links ]
9. Patel N, Naidoo P, Smith M, et al. South African surgical registrar perceptions of the research project component of training: hope for the future? S Afr Med J. 2016;106(2):169-71. https://doi.org/10.7196/SAMJ.2016.v106i2.10310. [ Links ]
10. Brochu A, Aggarwal R. ScienceDirect Association for Academic Surgery Research during general surgery residency: a Web-based review of opportunities, structure and outputs. J Surg Res. 2017;223:149-54. https://doi.org/10.1016/j.jss.2017.10.024. [ Links ]
11. Souba WW, Tanabe KK, Gadd MA, Smith BL, Bushman MS. Attitudes and opinions toward surgical research. A survey of surgical residents and their chairpersons. Ann Surg. 1996;223(4):377-83. https://doi.org/10.1097/00000658-199604000-00006. [ Links ]
12. Robertson CM, Klingensmith ME, Coopersmith CM. Prevalence and cost of full-time research fellowships during general surgery residency: a national survey. Ann Surg. 2009;249(1):155-61. [ Links ]
13. Yang G, Zaid UB, Erickson BA, et al. Urology resident publication output and its relationship to future academic achievement. J Urol. 2011;185(2):642-6. https://doi.org/10.1016/j.juro.2010.09.097. [ Links ]
14. Andriole DA, Klingensmith ME, Fields RC, Jeffe DB. Is dedicated research time during surgery residency associated with surgeons' future career paths? Ann Surg. 2017;176(10):139-48. https://doi.org/10.1097/SLA.0000000000003015. [ Links ]
15. Patel N, Leusink A, Singh N, Koto MZ, Luvhengo T. Registrar perceptions on general surgical training in South Africa: a report by the South African Society of Surgeons in Training (SASSiT). S Afr J Surg. 2018;56(2):10-14. [ Links ]
16. Farrokhyar F, Amin N, Dath D, et al. Impact of the surgical research methodology programme on surgical residents' research profiles. J Surg Educ. 2014;71(4):513-20. https://doi.org/10.1016/j.jsurg.2014.01.012. [ Links ]
17. Aldous C, Clarke D, Van Wyk J, Rout C. Avoiding the distant elephant: a model to approach the research component of specialisation. BMC Med Educ. 2016;16(1):4-9. https://doi.org/10.1186/s12909-016-0661-x. [ Links ]
18. Clarke DL. Auditing the process of ethics approval for Master's degrees at a South African university. South African J Bioeth Law. 2014;7(1):23. [ Links ]
19. Nasir AA, Ameh EA, Ojo EO. Surgery in low- and middle-income countries: a survey of perceptions of surgical trainees on feedback during training in West Africa. World J Surg. 2020;44(8):2542-9. https://doi.org/10.1007/s00268-020-05535-w. [ Links ]
20. Williams CJ, Curran S. Research by senior registrars in psychiatry - lessons to be learned for the specialist registrar grade. Psychiatr Bull. 1998;22(2):102-4. https://doi.org/10.1192/pb.22.2.102. [ Links ]
21. ElobuAE, KintuA, Galukande M, et al. Evaluating international global health collaborations: perspectives from surgery and anaesthesia trainees in Uganda. Surgery. 2014;155(4):585-92. https://doi.org/10.1016/j.surg.2013.11.007. [ Links ]
22. Ng-kamstra JS, Greenberg SLM, Abdullah F, et al. Global Surgery 2030: a roadmap for high income country actors. BMJ Glob Health. 2016;1:e000011. https://doi.org/10.1136/bmjgh-2015-000011. [ Links ]
23. Harrison LM, Woods RJ, McCarthy MC, Parikh PP. Development and implementation of a sustainable research curriculum for general surgery residents: a foundation for developing a research culture. Am J Surg. 2020;220(1):105-8. https://doi.org/10.1016/j.amjsurg.2019.09.028. [ Links ]
24. Grova MM, Yang AD, Humphries MD, Galante JM, Salcedo ES. Dedicated research time during surgery residency leads to a significant decline in self-assessed clinical aptitude and surgical skills. J Surg Educ. 2017;74(6):980-5. https://doi.org/10.1016/j.jsurg.2017.05.009. [ Links ]
 Correspondence:
Correspondence:
M Barnard
Email: dr.margueritebarnard@gmail.com
Supplementary Data
The supplementary data is available in pdf: [Supplementary data]


{kind=link}