










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.60 n.4 Cape Town Dec. 2022
http://dx.doi.org/10.17159/2078-5151/SAJS3714
VASCULAR SURGERY
Aortoenteric fistulas - our experiences with surgeons' nightmare
G Altun; AC Özdemir; KY Giiven
Department of Cardiovascular Surgery, School of Medicine, Karadeniz Technical University, Turkey
ABSTRACT
BACKGROUND: Aortoenteric fistula (AEF) is a rare medical emergency, but one of the most difficult and threatening complications of gastrointestinal (GI) bleeding.
METHODS: A retrospective observational study was performed on patients hospitalised with GI bleeding and a definitive AEF diagnosis. We collected operative reports and medical records of patients operated on with an AEF diagnosis. The literature data and our data were analysed and discussed.
RESULTS: We admitted eight patients who were definitively diagnosed with AEF after reviewing our hospital records. All patients were male except one. Their ages ranged from 28 to 82, with a mean of 64. All but two patients had secondary AEF (SAEF). Four SAEF cases had open aortic surgery and three had a history of endovascular procedure. The main complaints of the patients on admission were poor general condition, abdominal pain, and GI bleeding. Melena was found in all patients. Hematemesis and hematochezia were other significant GI bleeding findings. Infected grafts were removed in all but one patient; extra-anatomical bypass surgery and bowel repairs were performed. One patient underwent endovascular repair. In all patients, the 30-day in-hospital mortality rate was 50%.
CONCLUSION: In patients presenting with GI bleeding, an aortoenteric fistula should be considered. The outcome depends on early diagnosis, the patient's medical status, the severity of infection, and the anatomic location of the affected aorta. A multidisciplinary approach, appropriate treatment planning and close follow-up after treatment lead to positive outcomes.
Keywords: aortoenteric fistula, diagnosis, gastrointestinal bleeding, surgical treatment
Introduction
Aortoenteric fistulas (AEFs) are a medical emergency and one of the rare causes of fatal gastrointestinal (GI) bleeding, often occurring after aortic aneurysm surgery and rarely as a result of primary aortic or intestinal pathologies.13 While most AEFs are regarded as a secondary complication following prior aortic surgery, they seldom develop primarily. The location of the fistula usually occurs between the abdominal aorta and the duodenum.4
Early diagnosis and surgery are required to manage AEF. Unfortunately, these types of cases often have intermittent and nonspecific findings, making diagnosis difficult.5,6 Diagnostic delay can worsen prognosis, especially in unstable septic patients with severe comorbidities. This situation simulates a nightmare for the clinicians and surgeons who are responsible for the care of the patient. The promptness of the diagnosis, the medical condition of the patient, the presence of severe infection and the anatomical site involved all affect the outcome.7 Despite all this, the use of planned up-to-date diagnostic and treatment methods and a multidisciplinary approach will reduce morbidity and mortality in AEF cases.
In this paper, we aimed to present our experiences in diagnosing and treating AEF patients in our clinic from 2010 to 2020, together with an analysis of the literature.
Materials and methods
A retrospective observational study was conducted of patients hospitalised with GI bleeding and a definitive diagnosis of AEF between 2010 and 2020 in the cardiovascular surgery department of Karadeniz Technical University. The local ethics committee approved the study protocol and stated that the study did not fall under the Medical Research Involving Human Subjects Act and, therefore, an informed consent form was not required.
We collected the operative and medical records of patients who underwent surgery with a diagnosis of AEF in the cardiovascular surgery department. Data were analysed, including demographic information, clinical manifestations and complications, physical examinations, laboratory and imaging findings, treatments and outcomes. The diagnosis of AEF was confirmed by endoscopy, radiographs and/or surgical findings. In addition, we evaluated the literature data and our data by scanning the literature.
Results
We enrolled eight patients who had a definitive diagnosis of AEF after reviewing our hospital records between 2010 and 2020. All patients were male except one. Their ages ranged from 28 to 82, with a mean of 64. All but two of the patients had secondary AEF (SAEF). In the medical history of patients with SAEF, four had open aortic surgery and two had endovascular procedures. Four SAEF cases had open aortic surgery and two had endovascular procedure in their medical histories. A patient diagnosed with primary AEF (PAEF) had a clinical history of gynaecologic surgery and radiation therapy. The fistula point in this patient was at the junction of the proximal right iliac artery and the proximal jejunum.
Although there was an endovascular aneurysm repair (EVAR) in the medical history of another patient diagnosed with PAEF, the fistula was located between the left iliac artery as a result of the expansion of the existing sigmoid tumour. There was no EVAR stent graft in this region. In this patient, AEF did not originate from the graft, but from the growth of the tumour on the intestine towards the vascular structures. The fistula localisations were at the level of the duodenum in all patients with SAEF. The main symptoms of patients on initial admission were poor general condition, abdominal pain and GI bleeding. Melena was present in all patients. Fistulas in the upper GI tract (duodenum 6/8) were mostly hematemesis as a bleeding clinic, while fistulas in the lower GI tract (colon 2/8) were in the form of hematochezia. One patient had Behcet's disease, one patient had colon cancer, and one patient had gynaecologic malignancy as concomitant diseases. Two patients had renal insufficiency, and all patients generally had pulmonary, blood pressure and diabetic problems (Table I).
Microorganisms, such as Staphylococcus hominis, Enterococcus faecalis, Enterococcus faecium, Eschericia coli, Candida albicans, Streptococcus anginosus, Enterobacter cloacae, Prevotella denticola, and Acinetobacter baumannii, were identified from patients' tissues, surgical materials and catheters. In all but one patient, infected grafts were removed, extra-anatomical bypass procedures were performed, and bowel repairs, such as omental filling and fistulectomy with duodenojejunostomy in the area of the fistula, were performed. Only one patient underwent bowel repair with an open surgical method following an endovascular vascular repair in the form of a hybrid procedure. The 30-day hospital mortality rate for all patients was 50% (Table II).
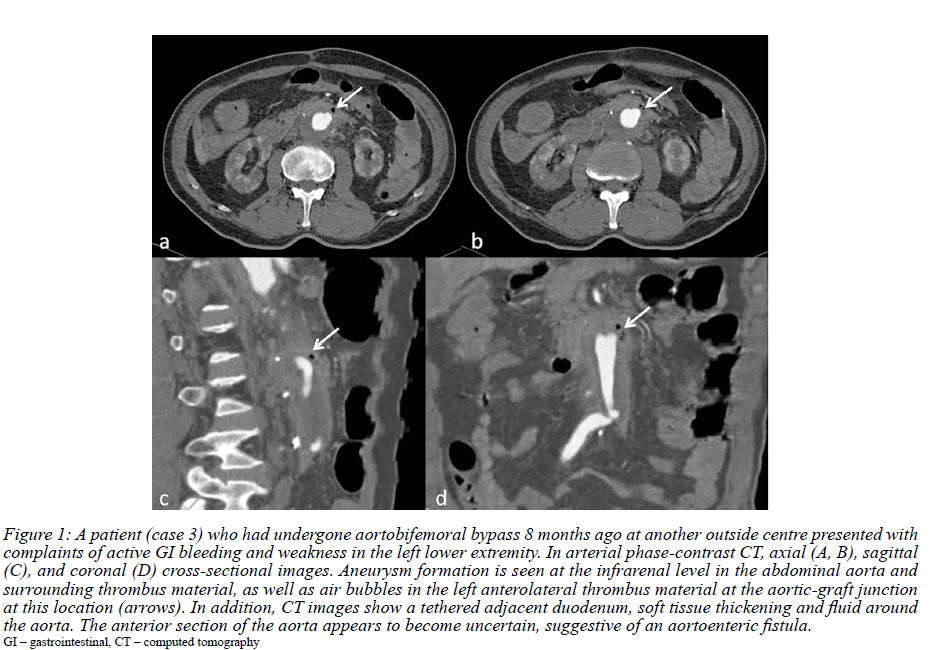
Computed tomography (CT) angio graphy was used in the final diagnosis of the patients, and oesophago-gastroduodenoscopy and/or colonoscopy were performed in appropriate patients to confirm the diagnosis (Figures 1 and 2).

Discussion
AEF is a rare and highly fatal GI bleeding cause, even in the hands of experienced surgeons. AEFs, occurring as primary or secondary, most commonly develop after open or endovascular aortic procedures.8 If a connection between the natural aorta and part of the GI system is present, it is defined as a PAEF and if a connection between an intestinal structure and a previous aortic graft is present, it is classified as a SAEF. If the aortic graft becomes infected, SAEF may develop in 20-45% of cases.9 The annual incidences of PAEF and SAEF in different series in the literature are approximately 0.04-0.07% and 0.36-2%, respectively.61011 The SAEF rate after EVAR for atherosclerotic aneurysmal disease is less than 0.5% in the literature. This rate is lower than the AEF rate observed after open aortic repair (1.6%).1213
The experience gained in our cases and the review of the literature have provided us with important and instructive information. However, the ideal level of diagnosis, follow-up and treatment has not yet been achieved. One reason is that most of the articles in the literature are case reports and the case series include a relatively small number of patients and do not include all possible complications of this clinical condition.
Because AEF is an unexpected cause of GI haemorrhage, medical history is critical to diagnosis. Early diagnosis and intervention have a beneficial and preventive effect on mortality and morbidity at this stage.14 Very few of the patients with AEF have massive bleeding. Patients with GI bleeding, regardless of signs of systemic infection, are usually in a poor clinical condition.11 The most critical aspect of effective surgical treatment is diagnosis during the precursor haemorrhage before the fatal haemorrhage. Hypotension and hematemesis are the most common symptoms of this interval, which can last from a few hours to several months. When the diagnosis and intervention are delayed, problems may progress rapidly, like a snowball becoming an avalanche. As a result, patients and doctors can experience desperate moments. Unfortunately, this situation is analogous to a nightmare.
If the patient with suspected AEF is unstable and bleeding massively, diagnostic tests can be ominously futile. Urgent laparotomy is required to control bleeding and diagnose or rule out AEF in these patients. If patients are stable, they can be evaluated by endoscopy or CT for diagnosis. However, oesophagogastroduodenoscopy can detect AEF in only about half of these patients.14 Scintigraphy and 18F-fludeoxyglucose (FDG)-positron emission tomography (PET)/CT are nearly perfect for diagnosing AEF but are technically impractical. Magnetic resonance imaging (MRI) has not been the preferred method of diagnosis because the screening time is longer and more technical expertise is required, and pulse artifacts and perigraft gas cannot be distinguished from aortic wall calcification.15
In recent years, CT has become the most commonly used procedure to confirm the diagnosis. The presence of gas or fluid around the graft or aorta can be revealed on a CT scan with contrast enhancement, which can help the diagnosis. A decrease in the periaortic fat plane, bowel wall thickness changes near the aorta, ectopic gas, tethering of adjacent thickened intestinal loops toward the aortic graft and a pseudoaneurysm in the anastomotic region are other symptoms that verify the diagnosis of AEF with CT. Aortic contrast extravasation into the bowel lumen is exceedingly uncommon, but it is the most distinguishing characteristic of AEF.10-14-16-17
The third part of the duodenum occupies anatomically a fixed position in the retroperitoneal region between the ligamentum Treitz, the aorta and the superior mesenteric artery. The proximity of this part of the duodenum to the aorta and to the proximal anastomotic region of the graft favours the development of AEF.6 Our series also reflects this situation. In our six cases, AEF formation was observed in this defined area.
One of the most important critical factors affecting survival in these individuals is immunity against the infections. In patients diagnosed with AEF, empiric broad-spectrum antibiotic treatment should be started as soon as microbiological culture samples are obtained. Further patient management and surgical preparation should be completed without waiting for culture results.16 Microbiological culture results of the cases reveal not only gram-negative or grampositive organisms but also mixed-type microorganisms. About 20% of the culture results are polymicrobial.2 Various microorganisms were also identified in our cases and in accordance with the results of the antibiogram, broad-spectrum antibiotics were given to the patients.
The main principles of AEF treatment may include extensive surgery to restore vascular circulation, closure of the fistula tract and complete removal of the infected prosthetic material.18 Considering that the potential for graft infection decreases as the graft is removed from infected surfaces, we ensured vascular continuity in our patients with an extra-anatomic bypass.19 Simultaneous bowel repair, complete excision of the infected graft, and axillobifemoral bypass procedures have been reported in the literature in patients with AEF, reducing early mortality and shortening the duration of surgery and trauma.20
Because the patency of extra-anatomic bypass grafts is low, it is appropriate to perform vascular reconstructions in these patients with bypass techniques in the anatomic position. For this purpose, graft materials, such as antibiotic or silver-coated infection-resistant prosthetic grafts, cryo-preserved grafts, and autologous vein grafts, have been developed.20,21 Each has its advantages and disadvantages. The major disadvantages of antimicrobial prosthetic grafts are the particularly low efficacy against methicillin-resistant microorganisms and the low graft patency rates.22,23 Cryopreserved arterial allografts may not be available in all centres because of their high cost. In addition, 10% of these patients have the possibility of spontaneous rupture.24 Although autologous saphenous graft (neoaortoiliac surgical reconstruction) is the most effective graft against infection, it has problems such as prolongation of surgical time in graft preparation, bleeding problems associated with the graft and clinical complaints of the extremity.24
In recent years, treatment of AEF has been associated with high morbidity and mortality, so more minimally invasive options have been tried. Endovascular repair is usually successful in the short term and has theoretical advantages with less surgical exposure and trauma, shorter operative time and less need for transfusion. EVAR may be used more frequently in patients who are not candidates for open surgery due to anatomic incompatibility or poor general health conditions caused by sepsis and haemorrhagic shock. However, the results show that in patients who are candidates for open repair, EVAR can be used as a bridging measure until definitive repair, especially in the presence of a septic condition.7,13,18,25
The insightful findings which we obtained from our cases and literature review can be summarised as follows: (i) When patients who have undergone aortoiliac surgery or intervention are admitted to the emergency department with GIS bleeding, these patients should be considered AEF until proven otherwise. (ii) Early surgery or intervention should be planned for patients with a strong suspicion of AEF. (iii) Patients' haemodynamic and clinical status should be monitored closely if their GI bleeding is stopped, because of the risk of herald bleeding. (IV) Patients with suspected or diagnosed AEF should be started on broad-spectrum anti-infective therapy as soon as possible after microbiological samples are collected.
Conclusion
In conclusion, AEFs are life-threatening conditions in which delays in diagnosis lead to catastrophic bleeding, morbidity and mortality. Outcomes depend on the early diagnosis, the medical status of the patient, the severity of infection and the anatomic location of the affected aorta. Graft excision and extra-anatomic bypass surgery or in situ graft replacement are the standard treatments for AEFs. Endovascular repair, on the other hand, has recently emerged as a viable therapeutic option. A multidisciplinary approach, appropriate treatment planning and close follow-up after treatment lead to positive outcomes.
Conflict of interest
The authors declare no conflict of interest.
Funding source
No funding was required.
Ethical approval
The medical ethical committee of Faculty of Medicine, Karadeniz Technical University approved the study protocol (24237895-567) and declared the study as not covered under WMO (Medical Research Involving Human Subjects Act) and therefore informed consent was not required (2021/171).
ORCID
G Alton https://orcid.org/0000-0003-1116-6594
AC Özdemir https://ortid.org/0000-0003-4356-0158
KY Güven https://orcid.org/0000-0002-4559-6843
REFERENCES
1. Mavilia MG, Wu GY. Aortoenteric Fistula. J Am Osteopath Assoc. 2019;119(2):135. https://doi.org/10.7556/jaoa.2019.022. [ Links ]
2. Chung J. Management of aortoenteric fistula. Adv Surg. 2018;52(1):155-77. https://doi.org/10.1016/j.yasu.2018.03.007. [ Links ]
3. Malekpour M, Irvan JL, Hashmi A, Widom KA, Ryer EJ. Aortoenteric fistula through a thrombosed graft. Am J Case Rep. 2020;21:e922153. https://doi.org/10.12659/AJCR.922153. [ Links ]
4. Saers SJ, Scheltinga MR. Primary aortoenteric fistula. Br J Surg. 2005;92(2):143-52. https://doi.org/10.1002/bjs.4928. [ Links ]
5. Rehman ZU, Sophie Z. Aortoenteric fistula: a difficult situation requiring multiple treatment options. J Coll Physicians Surg Pak. 2019;29(10):1015. https://doi.org/10.29271/jcpsp.2019.10.1015. [ Links ]
6. Ranasinghe W, Loa J, AllafN, Lewis K, Sebastian MG.Primary aortoenteric fistulae: the challenges in diagnosis and review of treatment. Ann Vasc Surg. 2011;25(3):386.e1-5. https://doi.org/10.1016/j.avsg.2010.09.021. [ Links ]
7. Kakkos SK, Antoniadis PN, Klonaris CN, et al. Open or endovascular repair of aortoenteric fistulas? A multicentre comparative study. Eur J Vasc Endovasc Surg. 2011;41(5):625-34. https://doi.org/10.1016/j.ejvs.2010.12.026. [ Links ]
8. Rossi UG, Cariati M. Aortoenteric fistula. J Cardiovasc Comput Tomogr. 2015;9(5):461-2. https://doi.org/10.1016/j.jcct.2015.03.009. [ Links ]
9. Batt M, Jean-Baptiste E, O'Connor S, et al. Early and late results of contemporary management of 37 secondary aortoenteric fistulae. Eur J Vasc Endovasc Surg. 2011;41(6):748-57. https://doi.org/10.1016/j.ejvs.2011.02.020. [ Links ]
10. Vu QD, Menias CO, Bhalla S, et al. Aortoenteric fistulas: CT features and potential mimics. Radiographics. 2009;(29):197-209. https://doi.org/10.1148/rg.291075185. [ Links ]
11. Luo CY, Lai CH, Wen JS, Lin BW. Secondary aortocolic fistula: case report and review of the literature. Ann Vasc Surg. 2010;24(2):256.e5-12. https://doi.org/10.1016/j.avsg.2009.07.025. [ Links ]
12. Kahlberg A, Rinaldi E, Piffaretti G, et al. Results from the Multicentre Study on Aortoenteric Fistulisation After Stent Grafting of the Abdominal Aorta (MAEFISTO). J Vasc Surg. 2016;64(2):313-320.e1. https://doi.org/10.1016/j.jvs.2016.04.008. [ Links ]
13. McCarthy MJ. Open or endovascular repair of secondary aortoenteric fistulae? Eur J Vasc Endovasc Surg. 2011;41(5): 635-6. https://doi.org/10.1016/j.ejvs.2011.01.011. [ Links ]
14. Yoshimoto K, Shiiya N, Onodera Y, Yasuda K. Secondary aortoenteric fistula. J Vasc Surg. 2005;42(4):805. https://doi.org/10.1016/j.jvs.2004.06.029. [ Links ]
15. Xiromeritis K, Dalainas I, Stamatakos M, Filis K.Aortoenteric fistulae: present-day management. Int Surg. 2011;96:266-73. https://doi.org/10.9738/0020-8868-96.3.266. [ Links ]
16. Ozdemir AC, Gemalmaz H, Yilmaz F. Aortoenteric fistulas: a case report and current status. Cardiovasc Surg Int. 2020;7(3):193-8. https://doi.org/10.5606/e-cvsi.2020.954. [ Links ]
17. Hagspiel KD, Turba UC, Bozlar U, et al. Diagnosis of aortoenteric fistulas with CT angiography. J Vasc Interv Radiol. 2007;18(4):497-504. https://doi.org/10.1016/jjvir.2007.02.009. [ Links ]
18. Lonn L, Dias N, Schroeder VT, Resch T. Is EVAR the treatment of choice for aortoenteric fistula? J Cardiovasc Surg. 2010;51(3):319-27. [ Links ]
19. Madan AK, Santora TA, Disesa VJ. Extra-anatomic bypass grafting for aortoesophageal fistula: a logical operation. J Vasc Surg. 2000;32(5):1030-3. https://doi.org/10.1067/mva.2000.107767. [ Links ]
20. Armstrong PA, Back MIR, Wilson JS, et al. Improved outcomes in the recent management of secondary aortoenteric fistula. J Vasc Surg. 2005;42(4):660-6. https://doi.org/10.1016/jjvs.2005.06.020. [ Links ]
21. Janko MR, Woo K, Hacker RI, et al. In situ bypass and extra-anatomic bypass procedures result in similar survival in patients with secondary aortoenteric fistulas. J Vasc Surg. 2021;73(1):210-21.e1. https://doi.org/10.1016/j.jvs.2020.04.515. [ Links ]
22. Bandyk DF, Novotney ML, Johnson BL, Back MR, Roth SR. Use of rifampin-soaked gelatin-sealed polyester grafts for in situ treatment of primary aortic and vascular prosthetic infections. J Surg Res. 2001;95:44-49. https://doi.org/10.1006/jsre.2000.6035. [ Links ]
23. Koshiko S, Sasajima T, Muraki S, et al. Limitations in the use of rifampicin-gelatin grafts against virulent organisms. J Vasc Surg. 2002;35:779-85. https://doi.org/10.1067/mva.2002.121850. [ Links ]
24. Oderich GS, Bower TC, Hofer J, et al. In situ rifampin-soaked grafts with omental coverage and antibiotic suppression are durable with low reinfection rates in patients with aortic graft enteric erosion or fistula. J Vasc Surg. 2011;53(1):99-107.e7. https://doi.org/10.1016/jjvs.2010.08.018. [ Links ]
25. Kakkos SK, Bicknell CD, Tsolakis IA, Bergqvist D; Hellenic Co-operative Group on Aortic Surgery. Editor's Choice -Management of secondary aorto-enteric and other abdominal arterio-enteric fistulas: a review and pooled data analysis. Eur J Vasc Endovasc Surg. 2016;52:770-86. https://doi.org/10.1016/j.ejvs.2016.09.014. [ Links ]
 Correspondence:
Correspondence:
email: gokalpaltun@gmail.com


{kind=link}
{kind=link}
{kind=link}