










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Surgery
versión On-line ISSN 2078-5151
versión impresa ISSN 0038-2361
S. Afr. j. surg. vol.60 no.4 Cape Town dic. 2022
http://dx.doi.org/10.17159/2078-5151/SAJS3737
GENERAL SURGERY
A comparative analysis of the upper gastrointestinal endoscopic reporting systems within the Durban Metropolitan complex
MT UmarI; MANoorbhaiII
IDepartment of Surgery, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, South Africa
IINetcare Umhlanga Hospital, South Africa
ABSTRACT
BACKGROUND: The minimal standard terminology (MST) was developed by the World Endoscopy Organization (WEO) to standardise endoscopic reporting. This study compared current reporting within the Durban Metropolitan complex with the MST
METHODS: This observational retrospective study included 130 upper gastrointestinal endoscopy reports from five different hospitals. The data were compared to the current reporting standard in the MST. The Noorbhai Maharaj (NM) score was used to assess and grade the quality of reporting
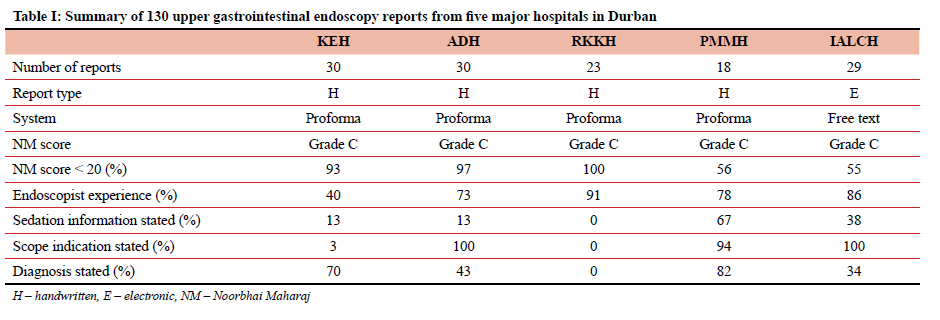
RESULTS: Each of the five hospitals has different endoscopic reporting systems. One hundred and thirty patients were included in the study, of which 60 were female. The indications for upper endoscopy were stated in 77 reports (59%). The commonest indications were epigastric pain (23%), dyspepsia (10%) and heartburn (10%). Sedation information per hospital was mostly seen at Inkosi Albert Luthuli Central Hospital (IALCH) (83%), followed by Prince Mshiyeni Memorial Hospital (PMMH) (67%), Addington (ADH) (13%), King Edward VIII Hospital (KEH) (13%), and RK Khan Hospital (RKKH) (0%). Consultant endoscopies per hospital were RKKH (91%), IALCH (86%), PMMH (78%), ADH (73%) and KEH (40%). All 130 reports were graded as NM Grade C. Scores of less than 20 points were seen in 106 reports (82%) and reflected across the different hospitals as follows: RKKH (100%), ADH (97%), KEH (93%), PMMH (56%) and IALCH (55%
CONCLUSION: There is no uniform structured endoscopic reporting system within the Durban Metropolitan Hospital complex. The current reporting methods do not meet the MST. The introduction of a structured standard endoscopic reporting system could improve the quality of reporting
Keywords: upper gastrointestinal endoscopic reporting systems, comparative analysis
Background
There is currently no universal/uniform reporting system for upper gastrointestinal endoscopic procedures that is shared between the different hospitals in Durban, South Africa. Each of the five hospitals in the Durban Metropolitan complex performs upper gastrointestinal endoscopy for various indications based on symptoms or disease processes, and the system of reporting may vary from handwritten reports to simplistic, computerised data collection (word processor) type reporting. Previous authors have suggested standardised endoscopic reporting, which could be used by individual hospitals.1-4 This would serve as a guideline for accurate and uniform reporting which would allow for inhospital and inter-hospital data analysis.
The minimal standard terminology (MST) is an internationally accepted guideline suggested by the World Endoscopy Organization (WEO). It details the type of indications, therapeutic procedures and diagnoses that may be observed during an endoscopic procedure and guides the endoscopist on accurate reporting of the procedure.5 The MST forms the basis for standardised endoscopic reporting by utilising uniform structures and terminology and limiting subjective, free-text phrases. This type of system affords substantial benefits to medical practice, such as data collection and auditing for quality assurance programmes and formation of databases for clinical research.4 Utilisation of a standardised system also offers the opportunity for registrars and specialists to become more knowledgeable on endoscopic reporting. This knowledge is furthermore of use when preparing for the Colleges of Medicine of South Africa (CMSA) fellowship and subspecialist exams.6,7 Overall, the impact of utilising such a system leads to improved patient care and outcomes.
A previous single-centre study by Maharaj et al. found that endoscopy reports were incomplete at King Edward VIII hospital as the MST guidelines were not routinely utilised.8 We have now expanded this study to include the five major hospitals in the Durban Metropolitan complex to assess whether current reporting systems meet the MST guidelines.
Methods
Study setting
This retrospective, descriptive study was conducted at the five major hospitals in Durban, namely King Edward VIII (KEH), Inkosi Albert Luthuli Central (IALCH), RK Khan (RKKH), Prince Mshiyeni Memorial (PMMH) and Addington (ADH). It included all patients who had undergone upper gastrointestinal endoscopy during the study period, with no distinction being made between elective and emergency procedures. Endoscopy reports were retrieved at random from each hospital's filing system. The data were de-identified prior to assessment.
Study design
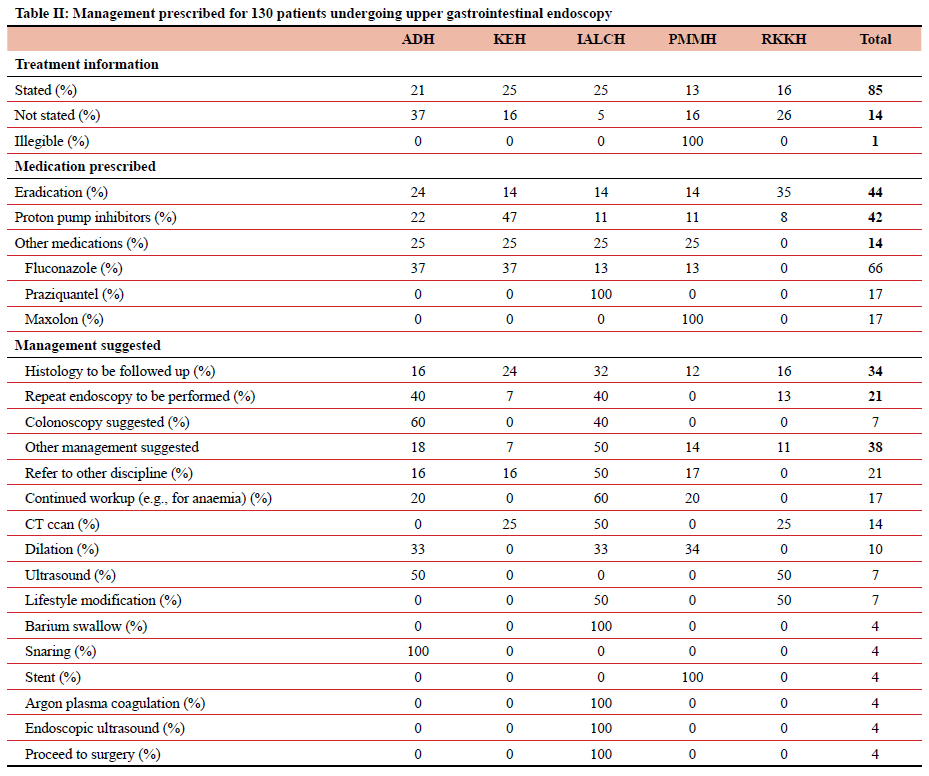
The study period was from 1 January 2017 to 31 December 2019. The variables analysed were extracted from each hospital's existing upper gastrointestinal reporting proforma. These included patient demographics, indication for endoscopy, use of sedation and specific variables as detailed in Table I. The following MST-based pathology-specific classification systems were evaluated: Los Angeles (LA) classification of erosive oesophagitis,9 Baveno consensus classification of varices,10 Prague classification of Barrett's oesophagus,11 Forrest classification of bleeding ulcers,12 Paris classification of superficial neoplastic lesions,13 and the Japanese Gastric Cancer Association (JGCA) classification of gastric carcinoma.14 Details of further management were documented as shown in Table II.
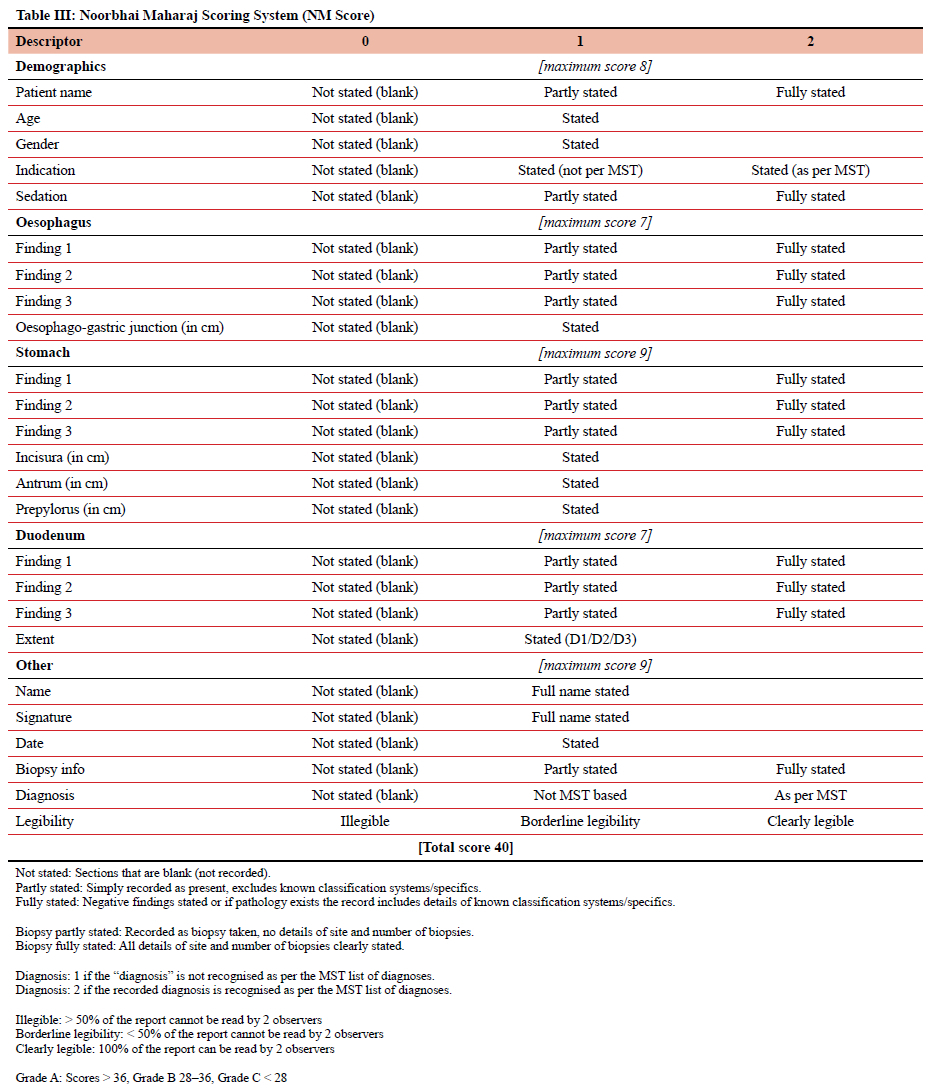
We also analysed the legibility of the endoscopy report, level of experience of the endoscopist (specialist versus trainee), procedures performed during the endoscopy and any omitted details. The variables and details extracted from the endoscopy reports were compared to the current reporting standard as listed in the MST, version 3.0.5 The Noorbhai Maharaj score (NM score) was used to assess the quality of reporting, based on its conformity to the MST (Table III).8 Each report was graded by the detail of information provided as well as the knowledge of the endoscopist on relevant classification systems.
Patient reports
Thirty endoscopy reports were included from each hospital. The number of reports required was based on the previous study conducted by Maharaj et al.8 Each hospital's endoscopy register was accessed, and random hospital numbers were selected. Endoscopy reports were then requested from the filing system. During the year of 2018, PMMH did not perform any upper gastrointestinal endoscopies due to a lack of equipment, and endoscopy records for the year of 2017 were missing at RKKH. Thus, the final sample size was 130. Data was extracted collected and analysed in Microsoft Excel.
Results
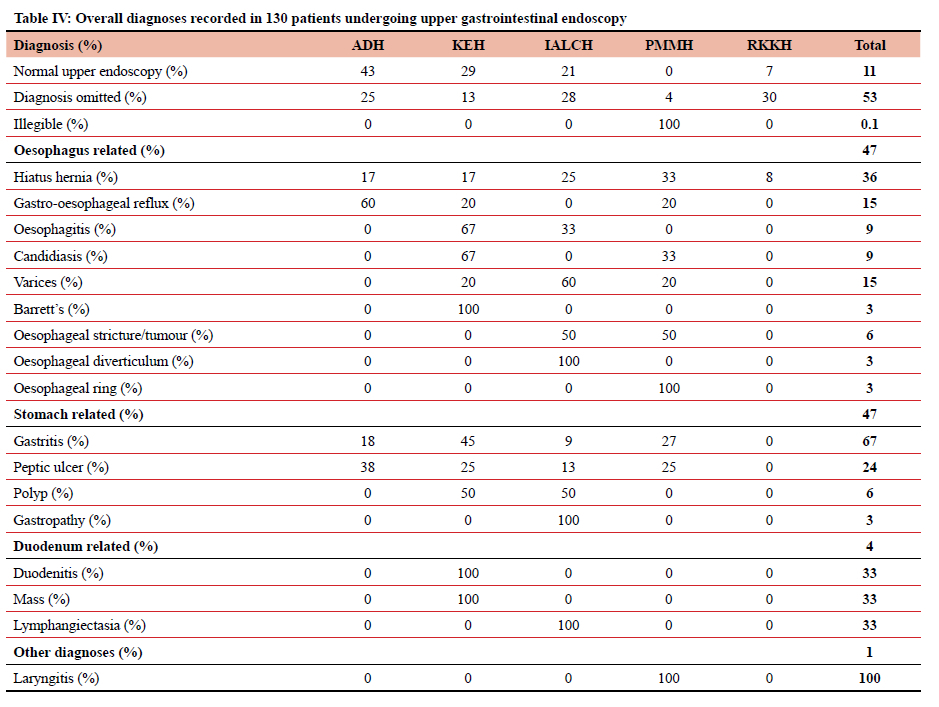
Four of the five hospitals included in this study used handwritten reports based on a "proforma" template with different variables. IALCH utilises a computer-based word processor system, which provides a generic, free-form text-based report. One hundred and thirty patients were included in the study, of which 60 were female, 50 were male, and in 20 gender was not recorded. The mean age of included patients was 53 years (IQR 19-79) and the median age 54 (SD ± 15) years. The indications for upper gastrointestinal endoscopy were stated in 77 reports (59%). These included epigastric pain (23%), dyspepsia (10%), heartburn (10%), dysphagia (5%), anaemia (5%), hematemesis (4%), weight loss (4%), oncology workup (4%) and melena (3%). There were 11 reports where a pre-existing diagnosis was stated, including trachea-oesophageal fistula (n = 2), portal gastropathy (n = 2) and oesophageal cancer (n = 1) (Table IV).
Information regarding the use of pre-procedural sedation was not stated in 89 (68%) reports. Overall, two reports recorded the use of pre-procedural sedation (midazolam). Throat spray local anaesthesia was recorded in 24 (18%) patients. The reports were either typed (22%) or handwritten (78%). Reports were clearly legible in 117 (90%), borderline legible in 12 (9%), and illegible in one (1%). Most of the upper endoscopies (73%) were performed by consultants: RKKH (91%), IALCH (86%), PMMH (78%), ADH (73%) and KEH (40%).
Endoscopic findings are summarised in Table IV. In patients with a hiatus hernia, the type of hiatus hernia was stated in 12 (46%) and not stated in 14 (54%) cases. Of the 15 reports where oesophagitis was diagnosed, the LA classification was not used in seven (47%). The oesophageal varices grade and Prague classifications for Barrett's dysplasia were not reported. In patients with gastritis, the site was stated in 34 (56%), the grading in 23 (18%) and biopsies were reported as taken in three (5%) patients. In patients with peptic ulceration, the ulcer site was recorded in 11 (85%) and the Forrest classification in five (38%) patients. The size of the ulcer was not stated in any of the reports. Biopsies were recorded as taken in five (38%) reports. In the five (4%) reports where gastric polyps were noted, the polyp site was stated in four (80%) and biopsies taken in three (60%). In patients with duodenitis, the site of the duodenitis was reported in three (25%). In patients with duodenal ulceration, the site of the ulcer was reported in three (100%), of which two (67%) were biopsied. In patients with a duodenal mass noted, the site of the mass was stated in one (33%) and the mass was biopsied in two (67%).
Of the 130 reports, an overall diagnosis was stated in 60 reports (46%), omitted in 69 reports (53%) while one report was illegible. Of the 60 reports in which a diagnosis was stated, a normal upper endoscopy was recorded in 14 (23%) patients. Further management is summarised in Table II. Proposed management was recorded in 110 (85%) reports, 19 (15%) reports were left blank and 1 was illegible. The NM score was applied to all reports. All 130 reports (100%) were Grade C and scores of less than 20 points were seen in 106 reports (82%).
Discussion
Gastrointestinal endoscopy is an integral part of surgical practice. The accuracy and adequacy of endoscopic reporting and determining a correct diagnosis are crucial for optimal treatment planning. It is important for these reports to contain adequate and relevant information clear to all treating physicians. Endoscopic reports should follow a structured standardised format, including key positive and negative findings that are stated in correct terminology and making use of widely accepted classification systems. To standardise endoscopic reporting, the WEO has suggested a guideline detailing the indications, therapeutic procedures and diagnoses that may be observed during an endoscopic procedure.5 This MST includes a standardised reporting structure and suggested terminology. It promotes accurate reporting and is well understood by all colleagues.
A single-centre study by Maharaj et al. demonstrated that the MST is not routinely utilised and that reports were incomplete.8 In the current study, all reports were found to be inadequate (Grade C). We have found that the reports lack uniformity with different formats used in each of the five centres. This results in lack of uniformity in reporting between the centres and inconsistency in the variables reported. The major contributing factor to the low scoring is the nature and completeness of data recorded on these reports. MST-specific report variables are also inconsistently used. With many sections of the proforma being left blank, especially the diagnosis and management sections, it was not clear whether there was no abnormality present, or whether the parameter was not assessed at all.
The MST guidelines allow for standardised reporting and uniform data capturing into searchable databases. Such databases are valuable for quality assurance programmes and personal and unit trends may be tracked over time. Indications and volume as well as performance measures can be accurately monitored, including morbidity and mortality. Quality assurance programmes improve overall quality of patient care and limit unnecessary procedures.15-17
Standardised reporting systems also have educational value in offering a structured approach to endoscopic examinations. Knowledge of the MST is likely to improve detection and improve the quality of the procedure in general. Having a standardised endoscopy reporting system will also facilitate objective assessments, by comparing trainee endoscopist reports to a set of recognised benchmarks to assess completeness and proficiency.1819
Study limmitations
We acknowledge that this is a small retrospective study. The numbers are not evenly distributed across the hospitals because one hospital could not find records for a particular year, and another hospital did not perform any endoscopic procedures for an entire year due to a lack of equipment.
Conclusion
This study clearly demonstrates the shortcomings in upper gastrointestinal endoscopy reporting and the need for a standardised reporting system across all hospitals. The many advantages of electronic MST-based reporting systems will improve the quality of investigations which will result in better patient care. It will facilitate the standardisation of endoscopic teaching and training, as well as serve as a data bank for measuring outcomes and for research.
Conflict of interest
The authors declare no conflict of interest.
Ethical approval
The study was approved by the Biomedical Research Ethics Committee (BE 269/15) of the University of KwaZulu-Natal, Durban, South Africa.
ORCID
MT Umar https://orcid.org/0000-0003-6516-6023
MANoorbhai https://orcid.org/0000-0002-0226-7986
REFERENCES
1. Delvaux M, Crespi M, Korman L, et al. Minimal standard terminology for digestive endoscopy. Terms and attributes, Version 2.0. Normed Verlag, Bad Homburg: Englewood NJ; 2002. [ Links ]
2. Delvaux M, Korman L, Armengol-Miro J, et al. The minimal standard terminology for digestive endoscopy: introduction to structured reporting. Int J Med Inform. 1998;48(1):217-25. https://doi.org/10.1016/S1386-5056(97)00128-7. [ Links ]
3. Delvaux MM. Standardisation of the endoscopic report. In: Waye JD, Rex DK, Williams CB. Colonoscopy: principles and practice. Massachussets: Blackwell; 2003. p.183-98. [ Links ]
4. Korman LY, Delvaux M, Crespi M. The minimal standard terminology in digestive endoscopy: perspective on a standard endoscopic vocabulary. Gastrointest Endosc. 2001;53(3):392-6. https://doi.org/10.1016/S0016-5107(01)70431-2. [ Links ]
5. Aabakken L, Rembacken B, LeMoine O, et al. Minimal standard terminology for gastrointestinal endoscopy-MST 3.0. Endoscopy. 2009;41(8):727-8. https://doi.org/10.1055/s-0029-1214949. [ Links ]
6. College of Medicine of South Africa (CMSA). Regulations for admission to the fellowship of the College of Surgeons of South Africa FCS (SA) Johannesburg: CMSA; 2019. Available from: www.collegemedsa.ac.za/view_exam.aspx?examid=46. Accessed Jul 2019. [ Links ]
7. College of Medicine of South Africa (CMSA). Regulations for admission to the examination for Sub-Specialty Certificate in Gastroenterology Johannesburg: CMSA; 2019. Available from: www.collegemedsa.ac.za/view_exam.aspx?examid=92. Accessed Jul 2019. [ Links ]
8. Maharaj SP, Noorbhai MA, Madiba TE. Does the reporting of gastro-intestinal endoscopy meet the minimal terminology standard at King Edward VIII Hospital? S Afr J Surg. 2017;55(4):36-42. [ Links ]
9. Sami SS, Ragunath K. The Los Angeles Classification of Gastroesophageal Reflux Disease. Video Journal and Encyclopaedia of GI Endoscopy. 2013;1(1):103-4. https://doi.org/10.1016/S2212-0971(13)70046-3. [ Links ]
10. De Franchis R, Baveno VI Faculty. Expanding consensus in portal hypertension: report of the Baveno VI Consensus Workshop: stratifying risk and individualising care for portal hypertension. J Hepatol. 2015;63(3):743-52. https://doi.org/10.1016/j.jhep.2015.05.022. [ Links ]
11. Sharma P, Dent J, Armstrong D, et al. The development and validation of an endoscopic grading system for Barrett's oesophagus: the Prague C & M criteria. Gastroenterology. 2006;131(5):1392-9. https://doi.org/10.1053/j.gastro.2006.08.032. [ Links ]
12. Forrest JAH, Finlayson NDC, Shearman DJC. Endoscopy in gastrointestinal bleeding. Lancet. 1974;2(7877):394-7. https://doi.org/10.1016/S0140-6736(74)91770-X. [ Links ]
13. Endoscopic Classification Review Group. Update on the Paris classification of superficial neoplastic lesions in the digestive tract. Endoscopy. 2005;37(6):570-8. https://doi.org/10.1055/s-2005-861352. [ Links ]
14. Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma. 3rd English ed. Gastric Cancer. 2011;14(2):101-12. https://doi.org/10.1007/s10120-011-0041-5. [ Links ]
15. Korman LY. Standardisation of endoscopic reporting - Déjà vu all over again? Clin Gastroenterol Hepatol. 2012;10(9):956-9. https://doi.org/10.1016/j.cgh.2012.07.001. [ Links ]
16. O'Mahony S, Naylor G, Axon A. Quality assurance in gastrointestinal endoscopy. Endoscopy. 2000;32(6):483-8. https://doi.org/10.1055/s-2000-649. [ Links ]
17. Manfredi MA, Chauhan SS, Enestvedt BK, et al. Endoscopic electronic medical record systems. Gastrointest Endosc. 2016;83(1):29-36. https://doi.org/10.1016/j.gie.2015.09.036. [ Links ]
18. Siau K, Green JT, Hawkes ND, et al. Impact of the Joint Advisory Group on Gastrointestinal Endoscopy (JAG) on endoscopy services in the UK and beyond. Frontline Gastroenterol. 2019;10(2):93-106. https://doi.org/10.1136/flgastro-2018-100969. [ Links ]
19. Freeman ML. Training and competence in gastrointestinal endoscopy. Rev Gastroenterol Disord. 2001;1(2):73-86. [ Links ]
 Correspondence:
Correspondence:
email: surgeonza@yahoo.com


{kind=link}
{kind=link}
{kind=link}
{kind=link}