










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.60 no.3 Cape Town Set. 2022
http://dx.doi.org/10.17159/2078-5151/sajs3855
CASE REPORT
Small bowel intussusception caused by a metastatic testicular germ cell tumour
J JohnI, II; B MaraisI; P SwanepoelIII; M SmitIII; N ComleyIV; D LouwIV
IDivision of Urology, Department of Surgery, Frere Hospital and Walter Sisulu University (East London), South Africa
IIDivision of Urology, Department of Surgery, Groote Schuur Hospital and University of Cape Town, South Africa
IIIAmpath Laboratories, South Africa
IVLife Healthcare, South Africa
SUMMARY
Intussusception from a testicular germ cell tumour is extremely rare. Metastatic gastrointestinal implants outgrow their blood supply leading to central necrosis. This results in erosions and ulcerations, which can be visualised as submucosal polypoid masses. These masses can then serve as a lead point for intussusception. We report a case of a 25-year-old patient with small bowel obstruction due to an intussuscepted choriocarcinoma in the absence of any other apparent retroperitoneal disease. Urologists must exclude gastrointestinal tract (GIT) involvement in testicular cancers, and similarly, surgeons need to exclude testicular tumours in young men with unexplained GIT haemorrhage, bowel obstruction or intussusception.
Keywords: germ cell tumour, choriocarcinoma, intussusception, testicular mass, orchidectomy, metastases, small bowel obstruction
Case presentation
A 25-year-old Caucasian male was referred with a six-month history of a progressively worsening swelling of the right hemiscrotum. There was no significant medical, surgical or family history. During the initial consultation, he had odd mannerisms, with random inappropriate outbursts and the patient's mother confirmed a change in behaviour over the preceding four months. Vital signs were normal, there was no evidence of gynaecomastia, and no lymph nodes were palpated. The abdominal examination was normal. Palpation and bedside ultrasound of the right hemiscrotum revealed a mass on the upper pole of the testis. The left testis was normal. Serum alpha-fetoprotein (AFP -41 ng/ml), beta-human chorionic gonadotropin (B-HCG -640 929 miU/ml) and lactate dehydrogenase (LDH -1 292 U/l) were all elevated. The rest of the blood work was unremarkable. An urgent right radical orchidectomy was performed.
Examination revealed a lobulated tumour (85 x 70 x 60 mm) of the upper pole of the right testis confined to the testis and epididymis (pT2) with large areas of necrosis and haemorrhage. Histopathological analysis showed a mixed non-seminomatous germ cell tumour (NSGCT) with a predominant choriocarcinoma component (90%) as well as yolk sac tumour (5%) and mature teratoma (5%) components. There was evidence of angiolymphatic invasion. He had an uneventful postoperative course after the radical orc-hidectomy and was discharged the following day with a follow-up with oncology for complete staging and initiation of chemotherapy. A day later, he presented to oncology with abdominal pain, distension and bilious vomiting. Physical examination showed a blood pressure of 138/72 mmHg, heart rate of 82 bpm, and respiratory rate of 18 breaths/ minute. His abdomen was soft but diffusely distended and tender to palpation, with reduced bowel sounds. No melaena was detected on digital rectal examination.
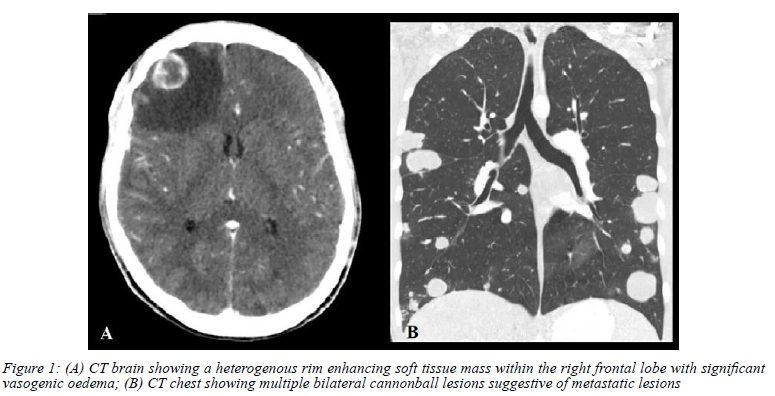
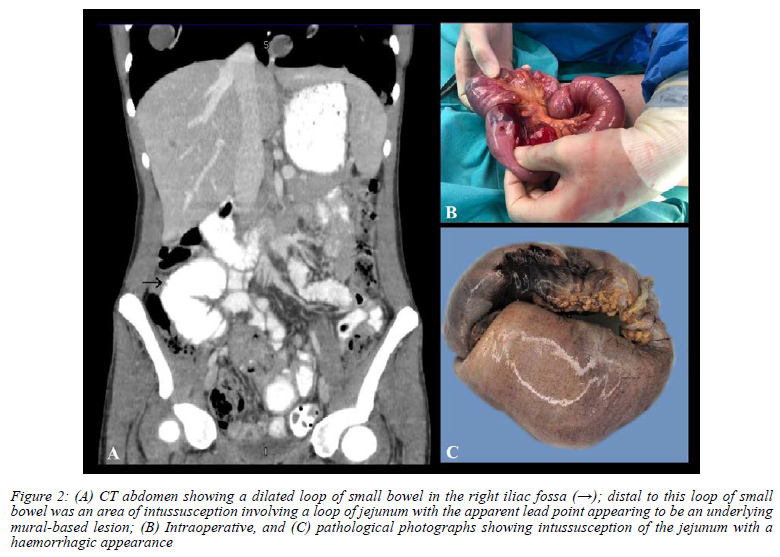
Further investigations confirmed the presence of extensive intra-abdominal, cranial and pulmonary metastatic disease (Figure 1 and 2A). CT abdomen revealed a dilated loop of small bowel in the right iliac fossa. Distal to this loop of small bowel, was an area of intussusception involving a loop of jejunum with the apparent lead point appearing to be an underlying mural based soft tissue mass measuring approximately 22 mm x 21 mm (T x AP) (Figure 2A). The patient was referred to our surgical colleagues for an explorative laparotomy. Intraoperatively, intussusception of the jejunum was confirmed with marked upstream dilatation and distal collapse and multiple mesenteric border metastases (Figure 2B). The affected segment of the bowel was resected and bowel continuity established by primary anastomosis. Examination of the intussuscepted small bowel showed mucosal ulceration and microscopy confirmed the presence of metastatic choriocarcinoma (Figure 2C). Both surgical margins and the excised lymph nodes were clear of disease.
Initially, there was clinical improvement post bowel resection. Chemotherapy (bleomycin, etoposide, and cisplatin) was initiated on day five post-resection. However, despite physiotherapy and early mobilisation, the patient developed Klebsiella pneumonia with rapid deterioration. Despite maximal organ support, his clinical condition deteriorated over the following days with the evolution of pancytopenia, and he died 18 days after his laparotomy.
Discussion
Testicular carcinoma, broadly classified into germ cell and non-germ cell tumours, is the most common solid organ malignancy affecting men between 15-45 years of age. It represents 1% of all male tumours and 5% of urological malignancies. While the incidence has been increasing over the years, cure rates for germ cell tumours (GCTs) are as high as 90%, and a 5-year survival rate of more than 95%.1,2 While retroperitoneal lymph nodes remain the most common site of metastases, the lungs, liver and brain are also frequently involved. Gastrointestinal tract (GIT) disease from metastatic GCT is sporadic, with clinically apparent GIT involvement occurring in less than 5% of cases.3,4 They occur in advanced disease due to either direct extension from affected retroperitoneal lymph nodes that drain the testes, haematogenous spread or peritoneal seeding.56 Metastatic implants generally fail to pass through the capillary barrier and deposit into the submucosa. Here, the tumour deposits outgrow their blood supply resulting in central necrosis leading to submucosal (occasionally even mucosal) erosions and ulcerations which can be visualised as submucosal or polypoid masses on endoscopy.7 These masses can form a lead point for intussusception.
Only a handful of cases7-10 of intestinal intussusception caused by metastatic deposits from GCTs have been reported. Abdominal pain and melena appear to be the most common presenting complaint. This is consistent with other reports in the literature where the main symptoms of GI metastasis from GCT are related to the presence of haemorrhage (melena, haematemesis and haematochezia) or bowel obstruction (abdominal pain, abdominal distension, vomiting) or perforation.
Of the four reported cases, histology from three was reported as metastatic non-seminomatous GCT - two pure choriocarcinomas7,8 and one a mixed germ cell tumour (embryonal carcinoma with yolk sac tumour).9 In one case, the tumour was only reported as a metastatic germ cell tumour, and no distinction between the subtypes was included.10 This reaffirms reports from other authors that pure seminomas are least likely to metastasise to the GIT.5
In the early 1970s, metastatic testicular cancer was associated with only 5% survival. With contemporary multimodal techniques involving chemotherapy, radiation and promising surgical procedures, 80% of patients will survive their disease.7 Based on the International Germ Cell Cancer Collaborative Group (IGCCCG), our patient falls into the poor prognostic category with a 5-year survival of 67%. As was the case with our patient, two of the other four patients died in the perioperative period or after the initiation of intense chemotherapy.8,9 However, patients with GIT metastases represent a group of patients with a much poorer prognosis. The histology of the primary testicular tumour may also contribute to the poor prognosis, as was the case in our patient. Choriocarcinomas are highly malignant lesions with a propensity for early, haematogenous metastases to distant organs, making it the GCT with the worst long term prognosis. In addition, intussusception and surgery delayed treatment and certainly compromised our patient's prognosis although he had a really heavy burden of metastatic disease.
Conclusion
Intussusception from a metastatic GCT is an infrequent finding, and we present only the fourth such case published. Nevertheless, surgeons need to be aware of this critical association. Urologists must exclude GIT involvement in testicular cancers and, similarly, surgeons need to exclude any testicular tumours in young men presenting with unexplained upper GIT haemorrhage, bowel obstruction or intussusception.
Conflict of interest
The authors declare no conflict of interest.
Funding source
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient's family for the anonymised information and the accompanying images published in this article.
ORCID
J John https://orcid.org/0000-0002-6139-810X
B Marais https://orcid.org/0000-0003-0637-0339
P Swanepoel https://orcid.org/0000-0002-3036-3115
M Smit https://orcid.org/0000-0002-9510-6435
N Comley https://orcid.org/0000-0001-7060-5855
D Louw https://orcid.org/0000-0002-4223-9998
REFERENCES
1. Baird DC, Meyers GJ, Hu JS. Testicular cancer: diagnosis and treatment. Am Fam Physician. 2018;97(4):261-8. [ Links ]
2. Smith ZL, Werntz RP, Eggener SE. Testicular cancer: epidemiology, diagnosis, and management. Med Clin North Am. 2018;102(2):251-64. https://doi.org/10.1016/j.mcna.2017.10.003. [ Links ]
3. Shogbesan O, Abdulkareem A, Jehangir A, et al. Gastrointestinal involvement of testicular germ cell tumour: a case report and literature review. Case Rep Gastrointest Med. 2017;2017:4789259. https://doi.org/10.1155/2017/4789259. [ Links ]
4. Senadhi V, Dutta S. Testicular seminoma metastasis to the gastrointestinal tract and the necessity of surgery. J Gastrointest Cancer. 2012;43(3):499-501. https://doi.org/10.1007/s12029-011-9274-0. [ Links ]
5. Chait MM, Kurtz RC, Hajdu SI. Gastrointestinal tract metastasis in patients with germ-cell tumor of the testis. Am J Dig Dis. 1978;23(10):925-8. https://doi.org/10.1007/BF01072468. [ Links ]
6. Johnson DE, Appelt G, Samuels ML, Luna M. Metastases from testicular carcinomal. Study of 78 autopsied cases. Urology. 1976;8(3):234-9. https://doi.org/10.1016/0090-4295(76)90374-5. [ Links ]
7. Elzamly S, Torabi A, Padilla O. Testicular choriocarcinoma metastasizing to the small bowel causing intussusception: case report. J Gastrointest Cancer. 2019;50(4):1005-8. https://doi.org/10.1007/s12029-018-0172-6. [ Links ]
8. Dassouli C, El Manjra C, Errami AA, et al. Small bowel metastases from a testicular choriocarcinoma revealed by gastrointestinal bleeding: a case report. Pan Afr Med J. 2021;39:259. https://doi.org/10.11604/pamj.2021.39.259.30325. [ Links ]
9. Oge O, Daphan C, Ozen H, Ayhan A. Intestinal testis tumor metastasis as a cause of intussusception: a case report. Int Urol Nephrol. 2000;32(1):93-94. https://doi.org/10.1023/A:1007128822701. [ Links ]
10. Hollander R, Beckes D, Kapre S, Matolo N, Liu S. A case of jejunal intussusception with gastrointestinal bleeding caused by metastatic testicular germ cell cancer. Dig Surg. 1999;16(5):439-40. https://doi.org/10.1159/000018764. [ Links ]
 Correspondence:
Correspondence:
J John
Email: jeffveenajohn@gmail.com


{kind=link}
{kind=link}