










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.60 n.3 Cape Town Sep. 2022
http://dx.doi.org/10.17159/2078-5151/sajs3281
GENERAL SURGERY
The spectrum, management and outcome of cellulitis in subtropical South Africa
S VariawaI; JJP BuitendagII; N JassiemI; GV OosthuizenI
IDepartment of Surgery, Ngwelezana Hospital, University of KwaZulu-Natal, South Africa
IIDepartment of Surgery, Tygerberg Hospital, Stellenbosch University, South Africa
ABSTRACT
BACKGROUND: This study aimed to ascertain the microbiology, severity stratification, and clinical outcomes of cellulitis based on our current management for comparison with international reports
METHODS: A retrospective chart review was conducted of all patients with cellulitis treated by the department of surgery at Ngwelezana Hospital over an 18-month period. Severity of cellulitis was graded, and a comparison was made of the Eron and Modified Dundee classifications. Superficial swabs were taken for culture on patients who had cellulitis with open wounds or blisters. Culture results, antibiotics used, need for surgical intervention, and length of hospital stay were documented and analysed
RESULTS: One hundred and thirty-four patients had cellulitis. Severity grading for classes I-IV in the Eron classification was 3%, 57%, 39% and 1%, respectively, and for the Modified Dundee classification, 47%, 11%, 38%, and 4%, respectively. Co-amoxiclav was the most used antibiotic (73%). Superficial skin swabs were taken from 49 patients and 34 cultured 44 specific organisms. The most common organism identified was Staphylococcus aureus (30%). Several gram-negative and anaerobic organisms were cultured. Fifty-three patients required surgical debridement of the infected area and one patient required an above-knee amputation. Mean hospital stay for patients who did not receive surgical intervention was 6 days (IQR 3) and 7 days (IQR 4) for those who did. There were no deaths
CONCLUSION: The Dundee classification triages fewer patients as class 2 severity than the Eron system and its use has the potentail to reduce the number of patients hospitalised. Gram-positive organisms predominated in those cultured, but gram-negative cultures were frequent compared to other reported series. Co-amoxiclav is effective as first-line antimicrobial therapy in our environment
Keywords: cellulitis, microbiology, culture, tissue specimen, comorbidities
Introduction
Cellulitis is defined as acute inflammation of the skin with involvement of the dermal and subcutaneous tissue layers secondary to bacterial infection.1 Cellulitis is commonly encountered with 75 838 inpatient admissions and 114 190 patients managed as outpatients annually in the UK.23 Multiple risk factors have been associated with the development of cellulitis. Local factors include any breach in the protective skin barrier, the presence of tinea pedis, lower limb ulcers due to venous insufficiency, pressure ulcers, untreated traumatic wounds and lymphoedema. General risk factors include raised BMI, immunocompromise, history of previous cellulitis, peripheral vascular disease and chronic alcoholism.14 The median age of presentation is 63 years in England compared to 52 years in Cameroon with females being more commonly affected than males in both studies.5,6 In South Africa, the Standard Treatment Guidelines and Essential Medicines List for hospitals recommend treatment with a combination of general measures that include limb elevation, adequate analgesia and antibiotics.7 Intravenous cloxacillin then oral flucloxacillin once clinical improvement is noted for 5-10 days is recommended. Clindamycin may be used in cases of penicillin allergy.7 These guidelines do not account for severity of disease, comorbidities or the presence of a preceding causative injury.7 International guidelines recommend that patients with purulent soft tissue infection require surgical intervention as well as antibiotic therapy and recognise the need to modify the route of delivery of antimicrobial and the need for hospitalisation based on the severity of the cellulitis as defined by either the Eron or Dundee classifications.6 In patients with nonpurulent soft tissue infection, the suggested first-line therapy is flucloxacillin either orally or intravenously for Dundee class I-II infection or class III-IV, respectively.8 Broader spectrum antibiotics such as clindamycin may be required for additional anaerobic cover in cases due to animal bites or where the soft tissue infection is classified as severe or necrotising.8
There is currently no published Southern African literature on cellulitis from a surgical perspective. Current management algorithms are guided by local facility practice guidelines based mostly on international literature and expert opinion.
At Ngwelezana Hospital, we see a significant number of patients with severe cellulitis with blisters or denuded areas, especially during extremely hot weather conditions, and mostly from rural areas. This prompted us to postulate that these infections may not be typical gram-positive infections as commonly referred to in international literature. The aim of this study was to ascertain the microbiology, severity stratification, and clinical outcomes based on our current management for comparison with international reports and as a baseline reference standard for future studies in the region.
Methods
Ngwelezana Hospital is a 554-bed hospital, designated as a tertiary hospital for the northern part of the province of KwaZulu-Natal. The hospital receives referrals from 18 hospitals for regional and tertiary care. All patients admitted with cellulitis by the department of surgery at Ngwelezana Hospital, within the 18-month period (1 May 2018-31 October 2019) were included in the study. Patients with a subsequent diagnosis of deep vein thrombosis of the affected limb were excluded from this study. Patients were identified from our electronic admissions register, and retrospective chart review followed. Severity of cellulitis was graded using both the Eron and Modified Dundee classifications (Table I). Patients were treated according to local policy. First line antimicrobial treatment for cellulitis at Ngwelezana Hospital is oral or intravenous flucloxacillin/cloxacillin; if not available, co-amoxiclav the second-line treatment was used. During the study period, superficial swab cultures were taken on patients who had cellulitis with open wounds or blisters. Superficial swabs were taken via a standardised method and in a sterile fashion. No tissue samples were taken for culture. Culture results and the antibiotic regimen were correlated. Patient demographics, comorbidities, physiological parameters and morbidities were recorded. The need for surgical debridement or amputation, escalation of antibiotics, and any deaths were also documented.
Statistics
Descriptive statistics were used. Continuous variables were expressed as mean and interquartile range (IQR) or standard deviation (SD) as appropriate. Chi-squared analysis was also used to assess other categorical variables between groups, including mortality, morbidity and injury mechanism. The different severity classifications were also compared.
Results
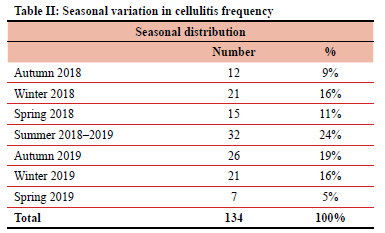
One hundred and thirty-four patients presented to our department with cellulitis during the study period. Ninety (67%) were female. The median age of presentation was 50 years (IQR 28 years). Cellulitis occurred most commonly during the summer months, from December to February (Table II).
Ninety per cent of patients presented with unilateral lower limb cellulitis, 7% with unilateral upper limb cellulitis and 3% with bilateral lower limb cellulitis. In 83 patients (62%) there was no history of a predisposing factor for the development of cellulitis, 44 patients (33%) had a history of preceding trauma to the involved limb of which 13 were animal/insect bites, and in the remaining seven patients other risk factors were identified that included the use of traditional healing methods and lymphoedema. Thirty-four per cent of patients had chronic hypertension, 31% were known with retroviral disease, 21% had diabetes mellitus, and 8% had documented peripheral vascular disease.
The majority of presenting patients were found to be haemodynamically stable. The median heart rate, respiratory rate, systolic and diastolic blood pressure were found to be within normal range. The mean white cell count was 14.9X109/L (range 3.2 X109/L to 63.2X109/L).
Comparison of the Eron and Dundee severity grading classifications is shown in Table I. The main difference is the reversal of the frequency of class I and II categories with far more being categorised as class I/milder infection in the Dundee classification.
Management
Of the 134 patients identified, four were managed with oral antibiotics on an outpatient basis, one declined treatment, and the remainder were admitted for initiation of intravenous antibiotics. Co-amoxiclav was the most commonly used antimicrobial (73%), followed by 12% of patients initiated on flucloxacillin/cloxacillin. Other less commonly used antibiotics were clindamycin for penicillin allergy and ciprofloxacin. In two patients, antimicrobials were changed from cloxacillin to co-amoxiclav and one from co-amoxiclav to ciprofloxacin during their admission based on culture results.
Eighty patients did not require surgical intervention. Fifty-three patients (40%) required surgical debridement of the infected area, and one patient required an above-knee amputation. The mean length of stay for patients who received surgical intervention was 7 days with an IQR of 4 days compared with a mean length of stay of 6 days with an IQR of 3 days for patients who did not receive surgical intervention.
Microbiology
Superficial skin swabs were taken on 49 patients with open wounds or denuded areas. No tissue samples were sent for culture. There was no growth on 11 swabs, a mixed growth on four swabs and specific organisms were cultured on 34 swabs. Forty-four organisms were identified with 10 patients culturing two organisms.
Staphylococcus aureus was the most common organism cultured (30%). Other organisms cultured were Acinetobacter baumannii (11%), Pseudomonas aeruginosa (11%), Streptococcus pyogenes (9%), Klebsiella pneumoniae (9%), Streptococcus dysgalactiae subsp. equisimilis (5%), Escherichia coli (5%), Enterobacter cloacae (5%) and Enterococcus faecalis (5%). These results showed no direct relation between predisposing risk factors or grading and positive cultures for atypical organisms.
Median length of stay was 6 days with an IQR of 4 days. There were no recorded mortalities related to cellulitis during this time period.
Discussion
During the summer months, there is an increase in the number of patients presenting and admitted with cellulitis at Ngwelezana Hospital. Zhang et al. showed an increase in the public's interest in cellulitis solely on the Google trends for that time period and suggested clinical data to validate their finding.9 Recent studies performed by Manning et al. and Peterson et al. showed similar results to our own. In non-tropical regions, lower limb cellulitis was more prominent in the summer months, whereas tropical regions reported lower limb cellulitis throughout the whole year.10,11 The study conducted by Peterson et al. showed that the odds of admission with cellulitis increased with higher temperatures in a dose-response fashion. In the summer months, the odds of being diagnosed with cellulitis are 66.6% higher than in winter months. These studies strengthen our observation that cellulitis is more common in the summer months, thus explaining the increase in presentations and admissions with cellulitis during this period.
An African study was conducted in a resource-limited, secondary-level setting in Cameroon aimed at identifying the burden of disease as well as common risk factors and organisms involved in the pathogenesis of cellulitis in the sub-Saharan region of Africa. Sixty-one patients admitted with cellulitis were included in this study and superficial skin swabs with gram staining were obtained for all patients included in the study. The vast majority of cultures were positive for streptococcal species (82%), while 15% of cultures were positive for staphylococcal species. No gram-negative species were identified.5
The above microbiology is in keeping with international literature indicating that gram-positive cocci are the pre-dominant species identified with superficial swab or tissue culture.12 Atypically, gram-negative species such as Pasteurella and Capnocytophaga or Aeromonas species have been associated with animal bites and immersion injuries respectively. Atypical organisms are also more common in patients with chronic comorbidities or immunosuppression.12 In comparison to our results, the majority of organisms identified on positive cultures were gram-positive staphylococcal and streptococcal species; however, there was also a significant number of gramnegative organisms cultured. Atypical organisms were not exclusively isolated in patients with immunosuppression or a history of animal bites.
We undertook to perform cultures on patients presenting with blisters or open wounds for the purpose of this study as we were unclear whether the spectrum of bacteria causing cellulitis was similar to that reported in international studies and provide a basis for empirical antimicrobial therapy. In a USA, study the sampling for culture was not routinely recommended due to poor yield. We concur that the yield is poor and that the results of culture rarely result in a change from the initial antimicrobial therapy, and recommend tissue cultures only be performed if the patient is systemically ill or immunocompromised at presentation. Deep tissue cultures have been shown to yield superior results when compared to superficial swab cultures and should be considered in cellulitis following human or animal bites or exposure of open wounds to salt or fresh water as these may yield atypical organisms.6,8,12,13 In this study, the majority of organisms cultured were gram-positive staphylococcal and streptococcal species; however, there was a significant number of gram-negative organisms cultured. There was no direct relation found between predisposing risk factors or severity grading and the organisms identified.
The severity of cellulitis can be classified according to the Eron classification or the Dundee classification.6,14 The Eron classification is based on expert opinion and has been incorporated into the CREST and NHS guidelines.14,15 We also used the Eron classification in our study to decide on the need for admission and found its application to be unclear at times, resulting in a high admission rate. The Dundee classification has become more commonly used in clinical practice and provides clear criteria for severity grading.14,15 It takes into account the markers for systemic sepsis and comorbidities using the Standardised Early Warning Score (SEWS).15 A study conducted by Marwick et al. showed that 70% of patients, based on the Eron classification, required inpatient antibiotic treatment. The same patient group based on the Dundee classification could have been managed on an outpatient basis.14 This concurs with the findings of this study, where 97% of patients required admission according to the Eron classification and only 53% of patients required admission according to the Dundee classification. Thus, we intend to use the Dundee classification for ease of use in clinical practice and to avoid unnecessary admissions to an already overburdened system.
The median length of stay for cellulitis was 3 days in the UK. In this study, it was double that and half of that in Cameroon.5,6 These variations are difficult to interpret as they are dependent on not only the severity of cellulitis but on hospital logistics which are difficult to quantify.
Unavailability of oral flucloxacillin and IV cloxacillin due to pharmacy logistics meant that co-amoxiclav was the primary treatment for over 70% of our patients. It provided excellent clinical response and we believe it is a good alternative as first-line therapy and perhaps the preferred first-line therapy in the categeory of patients we took culture swabs from, due to the significant presence of gram-negative organisms.
Conclusion
Based on the findings of this study, we believe that using the Dundee classification of cellulitis as a triage tool for admission can reduce hospital admissions. Skin culture results showed gram-positive species remain the dominant cause of cellulitis; however, a significant number of gram-negative organisms cultured had no direct relation to predisposing risk factors or severity grading. Co-amoxiclav either orally or intravenously, depending on severity grade, is effective as first-line antimicrobial therapy in our setting. We also recommend that tissue sampling be reserved for patients who do not show an adequate response to first-line therapy within 48 hours or where the diagnosis is uncertain.
Ethical approval
Ethics approval for this study was granted by the Biomedical Research Ethics Committee of the University of KwaZulu-Natal.
ORCID
S Variawa https://orcid.org/0000-0001-7672-1259
JJP Buitendag https://orcid.org/0000-0001-7169-129X
N Jassiem https://orcid.org/0000-0002-2667-8288
GV Oosthuizen https://orcid.org/0000-0001-6898-2969
REFERENCES
1. Raff AB, Kroshinsky D. Cellulitis. A review. JAMA. 2016;316(3):325-37. https://doi.org/10.1001/jama.2016.8825. [ Links ]
2. NHS Digital. Hospital Episode Statistics for England 2014-15. Available from: https://digital.nhs.uk/catalogue/PUB19124. [ Links ]
3. Bailey E, Kroshinsky D. Cellulitis: diagnosis and management. Dermatol Ther. 2011;24:229-39. https://doi.org/10.1111/j.1529-8019.2011.01398.x. [ Links ]
4. Tianyi FL, Mbanga CM, Danwang C, Agbor VN. Risk factors and complications of lower limb cellulitis in Africa: a systematic review. BMJ Open. 2018;8(7):e021175. https://doi.org/10.1136/bmjopen-2017-021175. [ Links ]
5. Njim T, Aminde LN, Agbor VN, et al. Risk factors of lower limb cellulitis in a level-two healthcare facility in Cameroon: a case-control study. BMC Infect Dis. 2017;17(1):418. https://doi.org/10.1186/s12879-017-2519-1. [ Links ]
6. Sullivan T, De Barra E. Diagnosis and management of cellulitis. Clin Med J. 2018;18(2):160-3. https://doi.org/10.7861/clinmedicine.18-2-160. [ Links ]
7. Republic of South Africa. Essential Drugs Programme. Hospital level (Adults) Standard Treatment Guidelines and Essential Medicines List. 4th ed. Republic of South Africa: National Department of Health; 2015. Available from: http://www.health.gov.za/index.php/standard-treatment-guidelines-and-essential-medicines-list. [ Links ]
8. Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections - 2014 update by the Infectious Diseases Society of America. Clin Infect Dis. 2014;59(2):e10-52. [ Links ]
9. Zhang X, Dang S, Ji F, et al. Seasonality of cellulitis - evidence from Google Trends. Infect Drug Resist. 2018;11:689-93. https://doi.org/10.2147/IDR.S163290. [ Links ]
10. Manning L, Cannon J, Dyer J, Carapetis J. Seasonal and regional patterns of lower leg cellulitis in Western Australia. Intern Med J. 2019;49(2):212-6. https://doi.org/10.1111/imj.14034. [ Links ]
11. Peterson RA, Polgreen LA, Sewell DK, Polgreen PM. Warmer weather as a risk factor for cellulitis: a population-based investigation. Clin Infect Dis. 2017;65(7):1167-73. https://doi.org/10.1093/cid/cix487. [ Links ]
12. Eron LJ, Lipsky BA. Use of cultures in cellulitis: when, how, and why? Eur J Clin Microbiol Infect Dis. 2006;25:615-7. https://doi.org/10.1007/s10096-006-0187-y. [ Links ]
13. Mutluoglu M, Uzun G, Turhan V, et al. How reliable are cultures of specimens from superficial swabs compared with those of deep tissue in patients with diabetic foot ulcers? J Diabetes Complications. 2012;26(3):225-9. https://doi.org/10.1016/j.jdiacomp.2012.03.015. [ Links ]
14. Marwick C, Broomhall J, McCowan C, et al. Severity assessment of skin and soft tissue infections: cohort study of management and outcomes for hospitalised patients. J Antimicrob Chemother. 2011;66(2):387-97. https://doi.org/10.1093/jac/dkq362. [ Links ]
15. Benjamin A, Lipsky MH, Silverman WS. A proposed new classification of skin and soft tissue infections modelled on the subset of diabetic foot infection. Open Forum Infect Dis. 2017;4(1):ofw255. https://doi.org/10.1093/ofid/ofw255. [ Links ]
 Correspondence:
Correspondence:
JJP Buitendag
Email: johan_buitendag@yahoo.com



{kind=link}