










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.60 n.2 Cape Town Jun. 2022
http://dx.doi.org/10.17159/2078-5151/SAJS3625
ENDOCRINE
The impact of non-closure of the platysma muscle layer on the cosmesis of thyroidectomy scar – a randomised double-blind controlled trial
OO AyandipoI; AO AfolabiI; CJ OnwudinjorII; C EzemeII; TAAdigunIII; S BelloIV
IDepartment of Surgery, College of Medicine, University of Ibadan and University College Hospital, Nigeria
IIDepartment of Surgery, University College Hospital, Nigeria
IIIDepartment of Anaesthesia, College of Medicine, University of Ibadan and University College Hospital, Nigeria
IVDepartment of Epidemiology and Medical Statistics, College of Medicine, University of Ibadan, Nigeria
ABSTRACT
BACKGROUND: The relevance of closing the platysma muscle layer after open thyroidectomy has received little interest in terms of research. The objective was to determine whether non-closure of the platysma muscle layer after open thyroidectomy impacts significantly on the cosmetic outcome of the resulting collar scar.
METHODS: In this prospective randomised controlled clinical trial, patients were assigned randomly to have the platysma muscle layer closed or not closed. The primary endpoint was the cosmesis of the collar scar six weeks after surgery assessed using the patient and observer scar assessment scale (POSAS). Additional endpoints included operation time and early postoperative wound complications.
RESULTS: Ninety-two patients were recruited, with 46 randomised to each group. The patient scar assessment subscale (PSAS) of the POSAS showed no significant difference in the scar cosmesis between the two groups six weeks after surgery (median PSAS: 16.5 vs 17.5; p = 0.514). The observer scar assessment subscale (OSAS) showed that the platysma muscle layer closure group had marginally better scars (median OSAS: 15 vs 17; p = 0.045). The size of the goitre did not make any significant difference in the scar cosmesis. There was no significant difference in the incidence of early postoperative wound complications as well as the median operation time.
CONCLUSION: Not closing the platysma muscle layer had no significant impact on the scar cosmesis six weeks after open thyroidectomy, with no significant difference in the incidence of early postoperative wound complications and the operation time.
Keywords: thyroidectomy, platysma, cosmesis, Ibadan
Introduction
Thyroidectomy is the most common endocrine surgical procedure performed throughout the world.1 In the city of Ibadan, Oyo State, Nigeria, it is one of the common elective surgical procedures performed.2 Open thyroidectomy is indicated for both benign and malignant thyroid conditions.3 Access to the thyroid gland usually commences by cutting through the skin and the platysma, which is a broad sheet of thin muscle located immediately under the subcutaneous fat, and covering the anterior neck as well as the upper chest regions on both sides. Due to its insertion to the skin, the platysma plays a part in facial expression, and may assist in opening the mouth.4
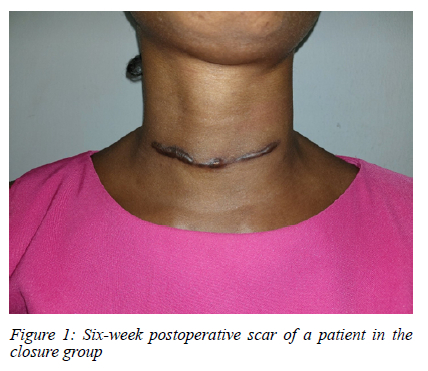
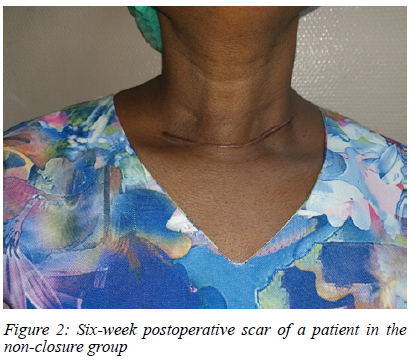
Being a surgery performed mostly on young women and on the anterior neck, an aesthetically appealing collar scar is of great importance following an open thyroidectomy. To achieve this, various methods of skin closure have been employed, ranging from the use of sutures to the use of staples, adhesive tapes and glue.5-7 The cosmetic advantages of the latter methods of skin closure over the use of sutures include minimal tissue reaction as well as lower risk of wound infection. However, the apparently common practice of closing the platysma muscle layer during the closure of open thyroidectomy wounds has not been scientifically proven to impact significantly on the aesthetic outcomes of the resulting collar scars.
The aim of this study was to determine whether non-closure of the platysma muscle layer following open thyroidectomy significantly influences the cosmesis of the scar, while the secondary objectives were to determine whether this impacts significantly on the operation time as well as the incidence of early postoperative wound complications.
Our hypothesis was that there is no significant impact of non-closure of the platysma muscle layer on the quality of the thyroidectomy scar.
Methods
This multi-centre prospective randomised controlled clinical trial was conducted in three hospitals in the Ibadan metropolis, namely the University College Hospital (UCH), St Mary's Catholic Hospital, and Oluyoro Catholic Hospital.8 Patients above 18 years old who had open thyroidectomy in these hospitals were recruited between September 2018 and September 2019. This trial was not registered with clinicaltrials.gov because we were not studying a drug or a device that has great impact on human life. However, it was registered with the West African College of Surgeons prior to its commencement. Exclusion criteria were previous thyroidectomy and a predisposition to keloid formation.
The subjects were recruited via the outpatient clinics and randomised on admission for surgery into two groups. Group A (intervention group) did not have platysma muscle layer closure, while group B (control group) had platysma muscle layer closure. Ethical approval was obtained from the University of Ibadan/University College Hospital (UI/ UCH) ethical review committee, and conduct followed the guidelines of the Helsinki declaration on biomedical research in human subjects.9 Confidentiality of the identity of the patients and personal health information was also maintained. Data were obtained using a proforma.
Preoperative workup
All the patients were evaluated clinically by the attending physicians, with their goitre sizes estimated using the World Health Organization (WHO) grading system.10 Investigations such as the thyroid function tests, plain radiographs of the neck, thyroid ultrasound scan and fine needle aspiration biopsy were also carried out and findings recorded prior to surgery. Laryngoscopy (direct or indirect) was performed by an otorhinolaryngologist.
Randomisation
Blocked randomisation with blocks of10 was used to allocate patients into the two groups. A randomisation sequence was computer-generated using STATA 12.0, and the sequence was concealed using brown opaque envelopes. The patients were randomised at admission in preparation for surgery. The patient and the observer were completely blinded, while the surgeon and the principal investigator were only made aware of the patient's randomisation group after apposing the strap muscles during wound closure.
Surgical technique
All operations were performed by consultant surgeons, according to a standard protocol for open thyroidectomy. This involved putting the patient under general anaesthesia (with a non-kinking endotracheal tube). The patient was then positioned at 15 degrees in reverse Trendelenburg, a sandbag placed under the scapulae, the neck extended, the occiput supported on a head-ring, and the upper limbs strapped by the sides of the body. Skin preparation was done using savlon (cetrimide and chlorhexidine gluconate combination), 10% povidone-iodine (polyvinylpyrrolidone and elemental iodine complex) and 70% isopropyl alcohol solution.
For all the surgeries, a skin incision was made using scalpel, while a horizontal incision on the platysma was made using monopolar electrocautery. The midline raphe of the strap muscles was split using electrocautery. Capsular dissection method was used to mobilise the gland in all the cases. After completion of the gland excision, haemostasis was secured using a combination of monopolar electrocautery, suture ligation and gauze packing.
For the wound closure, the strap muscles were apposed in interrupted fashion using synthetic absorbable coated 2.0 polyglycolic acid (safil) sutures, batch number HR37 (B Braun surgical). For those who had platysma muscle layer closure, this was done separately following the strap muscles closure, and in interrupted fashion using synthetic absorbable coated 2.0 polyglycolic acid (safil) sutures, batch number HR37 (B Braun surgical). This step was, however, omitted in the non-closure group (group A). Finally, the skin in each patient was closed using synthetic non-absorbable size 1 polypropylene (premilene) suture, batch number 1DS39 (B Braun surgical), using a subcuticular skin closure pattern with loops at the ends for easy removal. Pressure thyroidectomy dressing was applied afterwards. None of the patients recruited for the study had a wound drain inserted.
Postoperative management
Each wound was examined a few days after surgery, with the skin stitch removed on the fifth day. Each patient was followed up at two weeks post-surgery (for wound review and review of histology) and at six weeks (for scar evaluation and assessment of adequacy of the l-thyroxine dose).
Outcome measures and data collection
The primary outcome measures assessed included: the patient's satisfaction with the scar and an observer's satisfaction with the scar - both assessed six weeks after surgery using the validated patient and observer scar assessment scale (POSAS).1115 Two surgical resident doctors were trained to assess the scars using the POSAS, and they completed the observer part of the scale while the patients completed the patient part of the scale. The two surgical residents, as well as the patients, were all blinded to the randomisation. Other outcome measures included: operation time, incidence of early postoperative wound complications (haematoma and seroma formations, wound discharge, dehiscence, excess granulation tissue).
Statistical analysis
The sample size was calculated taking into consideration the standard deviation of patient scar assessment subscale (PSAS) score of 3.18 in conventional access thyroidectomy.16 To achieve a power of 80% and an attrition rate of 10%, the calculated sample size was 44 for each arm. The p-value for significance was set at 0.05.
Analysis was done on an intention-to-treat basis, with all patients analysed in their assigned groups.
Data were analysed using the IBM Statistical Package for Social Sciences version 25 (SPSS version 25). Continuous variables were summarised using means and standard deviations, and quartiles were used for the ordinal ones. Test of association between categorical variables was done using the Fisher's exact test, and that between continuous variables done using the Mann-Whitney U test.
Results
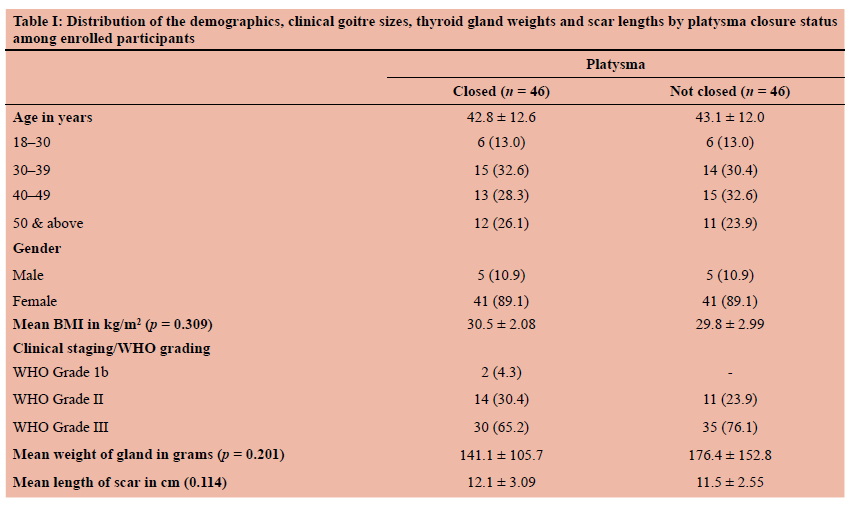
Ninety-two (92) participants were enrolled in the study and randomised into two groups, with 46 in each. The mean age of the enrolled participants was 43 ± 12 years, with an age range of 18-65 years for the platysma closure group and 21-65 years for the non-closure group. A quarter of them were aged 50 years and above. Furthermore, 82 (89.1%) of the participants were female, giving a female to male ratio of 8.2:1 (Table I). Out of all the surgeries, 90 were total thyroidectomies, while the remaining two were subtotal thyroidectomy and lobectomy respectively.
The majority of the goitres (65 in total) were WHO grade III goitres, with 30 of them in the closure group and 35 in the non-closure group (Table I). On average, the surgeries in which the platysma muscle layer was closed took slightly less time than those in which the platysma muscle layer was not closed. However, this was not statistically significant. Irrespective of the group, the average time it took to complete the thyroidectomies was 2 hours and 3 minutes (123 minutes). There was no significant difference in the time spent in the surgeries in both groups (p = 0.653). One participant in each group had wound dehiscence and seroma respectively; two participants had wound discharge and were both in the non-closure group; while the two participants who had haematoma and the only one who had excess granulation tissue were in the platysma closure group. There was no statistically significant association between any of the observed early postoperative wound complications and the experimental group. There was no limitation of mouth function in any of the participants. Furthermore, there was no statistically significant difference in the mean lengths of the scars for both groups as well as their mean body mass indices (BMI) as seen in Table I. The only participant who had a malignant goitre was in the non-closure group; the other 91 participants had simple goitres following the final pathological evaluation.
The patient scar assessment scale
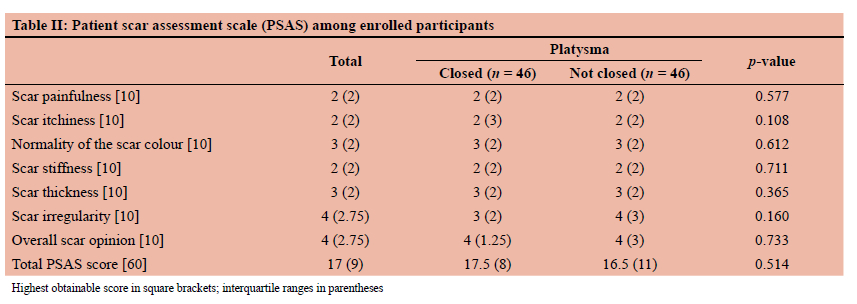
The results from the POSAS score as evaluated by the patients (the patient subscale) are presented in Table II. Each of the patients' scar characteristics were assessed by all patients. The scores for each of the scar characteristics by patients in both groups ranged from 1 to 10 out of 10. In the platysma muscle layer closure group, a median score of 2 was found for scar painfulness, scar itchiness and scar stiffness, while a median score of 3 was found for scar colour, scar thickness and scar irregularity. In the non-closure group, the median was 2 for scar painfulness, scar itchiness and scar thickness; 3 for scar colour and scar thickness; and 4 for scar irregularity. The median total PSAS score for the participants in the closure group was 17.5 out of 60, while that for the non-closure group was 16.5 out of 60 (Table II).
A comparison between the scar assessment scores of participants in the two groups using the Mann-Whitney U test showed no statistically significant difference in any of the evaluated scar parameters. There was also no statistically significant difference in the total PSAS scores between participants of the two groups (Table II).
The observer scar assessment scale
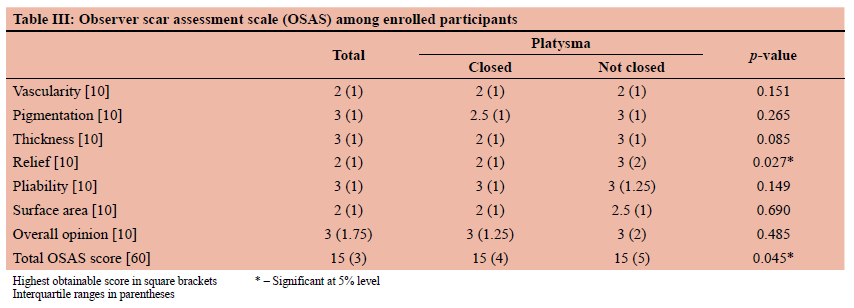
From the observer's evaluation, each of the scar parameters, as assessed in both groups, is presented in Table III. In the closure group, the parameters with the least median scores were vascularity, thickness, relief and surface area, with a score of 2 out of 10 each. The remaining parameters in this group, pigmentation and pliability, had median scores of 2.5 and 3 out of 10 respectively. In the non-closure group, vascularity and surface area had median scores of 2 and 2.5 out of 10 respectively, while the other parameters each had a median score of 3 out of 10. The median total OSAS score was 15 out of 60 for both groups (Table III).
The test of difference in OSAS score between participants from the two groups showed that only one of the scar parameters (the relief) and the total OSAS score were statistically significant (p = 0.027 for the relief score and p = 0.045 for the total OSAS score). Scores from the other parameters - vascularity, pigmentation, thickness, pliability, surface area, as well as the overall opinion, were not significantly different between the two groups (Table III).
Worthy of note from the relief score is that participants in the closure group had a lower median score (2 of 10) than those in the non-closure group (3 of 10). In a similar manner, the median total OSAS scores for both groups were marginally different. While one-quarter and three-quarters of those in the closure group had a score of 13 and 17 from 60 respectively with an average score of 15 from 60, participants in the non-closure group had a first quartile and third quartile score of 14 and 19 from 60 respectively, averaging 17 from 60 (Table III).
Discussion
Closure of the platysma muscle layer during open thyroid-ectomy seems to be a common practice among thyroid surgeons. The paucity of prospective studies in the literature in support of this practice makes it appear to be just a 'ritual' rather than an evidence-based practice of clinical relevance.17 In describing the surgeon's approach to the thyroid gland, Bliss et al. inferred without any formal scientific evidence that leaving the platysma muscle layer unsutured even offers better cosmetic results than when the platysma muscle layer is closed.18
In this study, the validated POSAS was used to evaluate the cosmesis of the collar scar six weeks after surgery. A comparison of the scar assessment parameter scores by the participants in both groups showed no statistically significant difference in both the individual scar parameters as well as the total PSAS scores. From the observer's point of view, a test of difference between the two groups showed that there was no statistically significant difference in all its parameters except for the relief and total OSAS scores in which the participants in the closure group had marginally better scores than those in the non-closure group. Thus, inference can be made that from the observer's point of view, participants in the closure group had a marginally better scar outcome than those in the non-closure group. These results are similar to those of a randomised clinical trial conducted by Senne et al. in 2016 at the University Hospital of Tubingen, Germany, in which they found no statistically significant difference in the POSAS parameters between two groups of patients (41 each) who had sutured or unsutured platysma muscle layers after thyroidectomy. They, however, stated that their study was not powered enough to detect minor differences in POSAS scores, thus not ruling out completely the possibility of a type II error.17
There was no statistically significant relationship found between any of the early postoperative wound complications and the groups to which the patients belonged. However, the two patients who had wound discharge were in the non-closure group, while the two who had haematoma and the one who had excess granulation tissue belonged to the closure group. In the study by Senne et al., a similar observation was made as there were no significant differences in clinically relevant seroma/haematoma formation or wound infection observed between patients in the closure group and those in the non-closure group. Owing to the relatively small number of patients in the study, and the low incidence of seroma formation in both groups, Senne and associates could not make any definitive statements regarding this finding.17
In our trial, the average overall operation time for the thyroidectomy was 123 minutes. There was no significant difference in the average operation time between the two groups. However, the average time spent in performing the surgeries that involved closing the platysma muscle layer was slightly less than that of those in which it was not closed. This could be due to the fact that most of the surgeries that required difficult and extensive dissection were coincidentally in the non-closure group. On the other hand, Senne et al. found out that the average operation time was significantly shorter in the non-closure group. This they explained by the fact that three surgeries that took especially long durations to complete were those in the closure group and so could have contributed to skewing the results in favour of the non-closure group.17
Conclusion
This study shows that the seemingly 'routine' practice of closing the platysma muscle layer before closing the skin following open thyroidectomy does not impact significantly on the cosmetic outcome of the collar scar. The closing or not closing of the platysma muscle layer does not make any significant difference in terms of the incidence of early postoperative wound complications. Finally, there is no significant difference that closure or non-closure of the platysma muscle layer makes with respect to the overall duration of the surgical procedure.
We, therefore, conclude that the closure of the platysma muscle layer is not mandatory during thyroidectomy.
However, the discretion of the surgeon may be applied in specific patient-centred situations.
Conflict of interest
The authors declare no conflict.
Funding sources
No funding was required.
Ethical approval
This study was conducted in accordance with declaration of Helsinki. Ethical approval was obtained from the joint University of Ibadan/University College Hospital Ethics Committee. NHREC/05/01/2008a.
ORCID
OO Ayandipo https://orcid.org/0000-0002-6806-8015
AO Afolabi https://orcid.org/0000-0002-6195-6669
CJ Onwudinjor https://orcid.org/0000-0002-6826-8332
C Ezeme https://orcid.org/0000-0001-9817-978X
TA Adigun https://orcid.org/0000-0002-6340-2221
S Bello https://orcid.org/0000-0003-0665-223X
REFERENCES
1. Bajwa SS, Sehgal V. Anesthesia and thyroid surgery -the never-ending challenges. Indian J Endocrinol Metab. 2013;17(2):228-34. https://doi.org/10.4103/2230-8210.109671. [ Links ]
2. Afolabi AO, Ayandipo OO, Afuwape OO, Ogundoyin OA. A fifteen-year experience of total thyroidectomy for the management of simple multinodular goitres in a low medium income country. S Afr J Surg. 2016;54(4):40-5. [ Links ]
3. Doherty GM. Current Diagnosis and Treatment Surgery. 14th ed. Chapter 16, Thyroid & Parathyroid. New York: McGraw Hill Education; 2015. p. 281. [ Links ]
4. McMinn RMH. Last's Anatomy. Regional and Applied. 9th ed. Chapter 6, Head and Neck. Edinburgh: Churchill Livingstone; 1998. p. 435. [ Links ]
5. O'Leary DP, Clover AJ, Galbraith JG, et al. Adhesive strip wound closure after thyroidectomy/parathyroidectomy - a prospective randomised controlled trial. Surgery. 2012;153(3):408-12. https://doi.org/10.1016/j.surg.2012.08.063. [ Links ]
6. Ridgway DM, Mahmood F, Moore L, Bramley D, Moore PJ. A blinded, randomised, controlled trial of stapled versus tissue glue closure of neck surgery incisions. Ann R Coll Surg Engl. 2007;89(3):242-6. https://doi.org/10.1308/003588407X179062. [ Links ]
7. Consorti F, Mancuso R, Piccolo A, Pretore E, Antonaci A. Quality of scar after total thyroidectomy - a single blinded randomised trial comparing octyl cyanoacrylate and subcuticular absorbable suture. ISRN Surg. 2013;2013:270953. https://doi.org/10.1155/2013/270953. [ Links ]
8. Wikipedia contributors. Ibadan. Wikipedia, The Free Encyclopedia. November 14, 2018,11:39UTC. Available from: https://en.wikipedia.org/w/index.php?title=Ibadan&oldid=868781013. Accessed 1 Dec 2018. [ Links ]
9. Williams JR. The Declaration of Helsinki and public health. Bull World Health Organ. 2008;86(8):650-2. https://doi.org/10.2471/BLT.08.050955. [ Links ]
10. Archampong EQ, Naaeder SB, Ugwu B. Baja's Principles and Practice of Surgery - including pathology in the tropics. 5th ed. Vol. 1. Chapter 22, The Thyroid and Parathyroid glands. Ghana: Repro India Ltd; 2015. p. 368. [ Links ]
11. Nguyen TA, Feldstein SI, Shumaker PR, Krakowski AC. A review of scar assessment scales. Semin Cutan Med Surg. 2015;34(1):28-36. https://doi.org/10.12788/j.sder.2015.0125. [ Links ]
12. Draaijers LJ, Tempelman FR, Botman YA, et al. The patient and observer scar assessment scale - a reliable and feasible tool for scar evaluation. Plast Reconstr Surg. 2004;113(7):1960-5; discussion 1966-7. https://doi.org/10.1097/01.PRS.0000122207.28773.56. [ Links ]
13. Van de Kar AL, Corion LU, Smeulders MJ, et al. Reliable and feasible evaluation of linear scars by the patient and observer scar assessment scale. J Plast Reconstr Aesthet Surg. 2005;116:514-22. https://doi.org/10.1097/01.prs.0000172982.43599.d6. [ Links ]
14. Van der Wal MBA, Tuinebreijer WE, Bloemen MCT, et al. Rasch analysis of the patient and observer scar assessment scale (POSAS) in burn scars. Qual Life Res. 2012;21(1):13-23. https://doi.org/10.1007/s11136-011-9924-5. [ Links ]
15. Truong PT, Lee JC, Soer B, Gaul CA, Olivotto IA. Reliability and validity testing of the patient and observer scar assessment scale in evaluating linear scars after breast cancer surgery. Plast Reconstr Surg. 2007;119(2):487-94. https://doi.org/10.1097/01.prs.0000252949.77525.bc. [ Links ]
16. Ma X, Xia QJ, Li G, Wang TX, Li Q. Aesthetic principles access thyroidectomy produces the best cosmetic outcomes as assessed using the patient and observer scar assessment scale. BMC Cancer. 2017;17(1):654. https://doi.org/10.1186/s12885-017-3645-2. [ Links ]
17. Senne M, Zein R, Falch C, et al. Randomised clinical trial of platysma muscle suture versus no suture for wound closure after thyroid surgery. Br J Surg. 2018;105(6):645-49. https://doi.org/10.1002/bjs.10829. [ Links ]
18. Bliss RD, Gauger PG, Delbridge LW. Surgeon's approach to the thyroid gland - surgical anatomy and the importance of technique. World J Surg. 2000;24(8):891-7. https://doi.org/10.1007/s002680010173. [ Links ]
 Correspondence:
Correspondence:
email: globalchiko@yahoo.com


{kind=link}
{kind=link}
{kind=link}