










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Surgery
versión On-line ISSN 2078-5151
versión impresa ISSN 0038-2361
S. Afr. j. surg. vol.60 no.1 Cape Town mar. 2022
http://dx.doi.org/10.17159/2078-5151/2022/v60n1a3556
SURVEY
Patient perceptions of surgical training in the private sector in South Africa - a single centre survey
D LutrinI, II; H EtheredgeI, III; J FabianI, IV; C BouterI; S TagerI
IWits Donald Gordon Medical Centre, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, South Africa
IIDepartment of Surgery, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, South Africa
IIISteve Biko Centre for Bioethics, School of Clinical Medicine, Faculty ofHealth Sciences, University of the Witwatersrand, South Africa
IVDepartment of Internal Medicine, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, South Africa
ABSTRACT
BACKGROUND: As the worldwide demand for specialist surgeons increases, and to complement surgical training provided through governmental institutions, private hospitals are increasingly hosting trainees. Wits Donald Gordon Medical Centre (WDGMC) is a private academic hospital in Johannesburg with a Colorectal Unit (CRU) that hosts several trainees. While published studies demonstrate that the involvement of trainees in surgery does not adversely impact outcomes, private patients' perceptions of the role of trainees in their care have not been as widely researched
METHODS: This was a prospective, cross-sectional study using a self-administered questionnaire hosted on a REDCap database. Statistical analysis was performed using SPSS version 26
RESULTS: One hundred and seventy-four patients participated in the study, and 74.1% of respondents felt that training of doctors should occur in private hospitals in South Africa. Of the sample, 83.3% would allow a supervised trainee to perform a part of their operation, provided they had been made aware of trainee participation in advance (78%). Sixty per cent of patients felt that interaction with a trainee enhanced their care, and 52.3% of patients suggested that seeing more than one doctor a day improved their experience
CONCLUSION: Our results suggest that privately funded patients support the surgical training of medical doctors in private academic training hospitals, and they are willing to be participants in the training process. Moreover, training programmes in this setting appear to enhance the patient experience. We are optimistic that these findings could be used to advocate for expanded training opportunities across the private sector in South Africa
Keywords: patient perceptions, surgical training, fellow, South Africa
Introduction
Academic hospitals are responsible for the training of surgeons and the subsequent surgical sub-specialties. Most surgical training programmes function as an apprenticeship where the trainee (either a registrar or fellow) is given progressive responsibility as they demonstrate increased competence. Initially, trainees will observe or assist during the surgical procedure, progressing to the position where they operate as the primary surgeon, and perform complex and critical parts of the procedure, while supervised by the consultant surgeon.
Conceptually, surgical training presents a unique dichotomy.1 The only way in which doctors can become competent surgeons is to gradually perform increasingly complex aspects of operations. Fortunately, the implications of surgical trainee involvement in patient care, and the associated outcomes, have been extensively researched worldwide and most agree that it is safe for patients to undergo surgery when trainees are involved. Supervised trainees achieve surgical outcomes for operations equivalent to those performed entirely by specialists, suggesting that operative quality is not compromised in an appropriate training setting.2-5 Similarly, there is no demonstrable difference in surgical outcomes when supervised trainees perform an entire operation, as opposed to select parts of it.6 Moreover, studies have found that overall quality of care afforded to patients improves in surgical training settings, especially relating to more complex surgery.7,8 It is acknowledged that trainee involvement may lead to an increased rate of minor complications (such as wound sepsis) - however, these complications are not deemed to adversely impact on patient outcome.9,10
Apart from reservations about outcomes and competence, another concern is that involvement of trainees increases operative times, especially relevant in private healthcare settings, where theatre time is billed by the minute, and hence longer operative duration represents an escalated cost to healthcare funders. While some studies have demonstrated a relatively small difference of 15-20 minutes in operative times when a trainee performs part of the operation, others have shown that operative times increased by approximately 15% and that the private sector was able and willing to subsidise this difference.11-15,16
While a synthesis of international literature regarding surgical training suggests that it probably does not compromise patient care, outcomes, or operative times, it is also important to understand patient perceptions of accessing surgical care in a training environment. One study considering this phenomenon concluded that the majority (86%) of patients support the notion of having a trainee involved in their operation, provided that trainee is supervised and that the patient has been made aware of trainee involvement in advance of the procedure.17
Surgical training in South Africa
As the worldwide demand for specialist surgeons increases, and to complement the surgical training provided through academic and governmental institutions, private hospitals are increasingly hosting trainees.18 As with most other countries, South African medical students, specialists, and sub-specialists primarily access training opportunities in the government sector. However, the concept of training in the private sector is gaining traction across many sub-specialty disciplines. Published South African research has demonstrated that surgical trainees felt they did not receive enough formal academic teaching, supervision in theatre or training in minimally invasive surgery across six of the eight established academic training centres in the country.19 The study in question further emphasised that the state sector faces challenges such as "staff and other resource shortages, poor infrastructure, and high patient loads" which hamper training opportunities. Another South African study found that surgical training was particularly lacking in certain specialist and sub-specialist areas, including vascular, major rectum and anus, burns, oesophagus and liver.20 Opportunities to augment access to training platforms in these specialities may be available in the private sector in South Africa.
Wits Donald Gordon Medical Centre (WDGMC) was established as a private academic teaching hospital within the School of Clinical Medicine, Faculty of Health Sciences (FHS), University of the Witwatersrand, Johannesburg (Wits). It is a Health Professions Council of South Africa accredited teaching and training facility within the Wits Academic Teaching Hospital Complex (which comprises Charlotte Maxeke Johannesburg Academic Hospital, Chris Hani Baragwanath Hospital, The Helen Joseph and Rahima Moosa Mother and Child Hospital Complex and the Klerksdorp-Tshepong Hospital complex). The format of training provided at WDGMC is determined by the Wits FHS, based on the needs of the university.
The WDGMC teaching and training model is unique. As the first of its kind in South Africa, the hospital has offered post-graduate training opportunities since 2007. Through funding additional trainee posts, WDGMC increases the number of trainees in the Wits teaching circuit and after completion of their training. As such, the hospital is an ideal platform for answering research questions that are relevant to both private healthcare in South Africa, and the tertiary education setting.
WDGMC hosts a dedicated high-volume colorectal surgery unit (CRU), that actively participates in specialist and sub-specialist surgical training through a formal teaching programme. Registrars in general surgery spend two months of their five-year training programme in the CRU, and colorectal surgery fellows spend a proportion of their two-year fellowship at WDGMC. The trainees hosted at WDGMC are clinically capable of operating on patients in a supervised capacity, with most of them having operated independently at the state hospitals.
Objectives
Although trainees play a significant role in the care of CRU patients at WDGMC, we have not established patient perceptions of our training programme. This paper reports the findings of our study to ascertain patient perceptions of training in the CRU at WDGMC. We were particularly interested in exploring private patients' opinion regarding the provision of surgical training in the private sector, and how they feel about trainee involvement in their own care.
Methods
A prospective, cross-sectional study design making use of a self-administered questionnaire was used. Ethical approval was obtained from the University of the Witwatersrand Human Research Ethics Committee (M1811122). All patients who were admitted to the WDGMC CRU from 1 February 2019 to 30 November 2019 and met the following inclusion criteria were invited to participate:
1. Over 18 years of age
2. Able to speak and read English
3. > 1 night stay in hospital at the time of discharge
4. Clavien-Dindo (CD) score 0, 1 or 2
5. Had surgery involving an incision in theatre, including laparoscopic surgery
6. Valid email address or internet access
Eligible patients were invited to participate in the study at the time of discharge. They were approached by a clinical associate or clinical research intern who had no role in the surgical care of the patient. These research assistants provided information about the study and answered any questions that patients had. The survey was administered through a REDCap database and consent was presumed by the patient filling in the questionnaire. Questionnaires were completely anonymous and no identifying information was collected. Statistical analysis was performed using SPSS version 26.
The CD score is a score used to rate surgical complications.21 Patients with a score of 0-2 have no complications to minor complications. Patients with higher CD scores have more serious complications, which often require re-intervention or prolonged hospitalisation. Patients with higher CD scores have been excluded from this study as their hospital stay may have been more traumatic, and we aimed to avoid psychological harm to this vulnerable group. A total of 38 patients were excluded from the study on account of having CD scores falling outside of our range for eligibility. However, this exclusion does not represent a source of significant bias in sampling, as the rate of major complications in the WDGMC CRU for the study period was approximately 7.8%, which is consistent with international complication rates.22
Results
Population overview
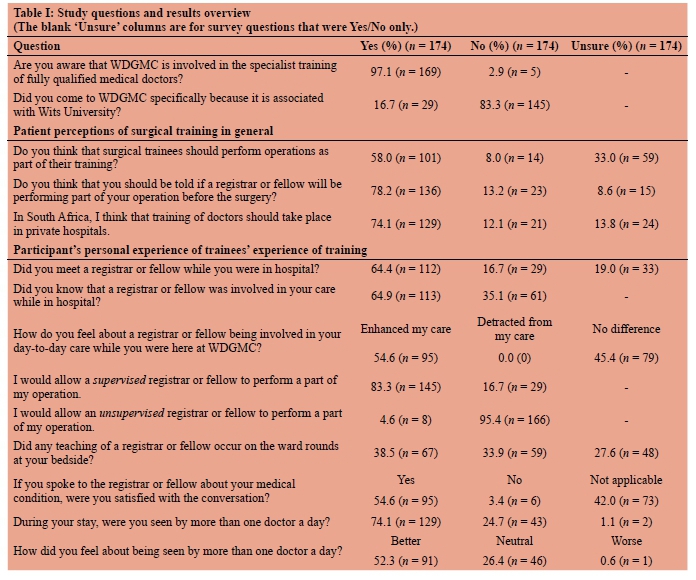
A total of 478 patients were suitable for inclusion in this study and the overall response rate was 36.4% (n = 174) over the study period. Because the survey was self-administered, we cannot elucidate reasons for non-participation. Of the respondents, 33.3% (n = 58) spent one night in hospital, 48.8% (n = 85) spent two to seven nights in hospital and 17.8% (n = 31) spent more than seven nights in hospital. Results are detailed in Table I.
Of the respondents, 74.1% (n = 129) felt that training of doctors should occur in private hospitals in South Africa. Additionally, 83.3% (n = 145) of the respondents would allow a supervised trainee to perform a part of their operation.
Of the 64.4% (n = 112) of respondents who met a trainee while in hospital, 88.4% (n = 99) stated that they would allow a trainee to operate on them under supervision. Of those who did not meet trainee, or were unsure whether they had met a trainee or not (62 respondents in total), 74.2% (n = 46) said that they would allow a trainee to operate on them under supervision. This suggests that the experience of meeting the trainee was a positive one and that the encounter with the trainee made it more likely that the patient would allow the trainee to perform a part of their operation (p = 0.02)
Seventy-eight per cent of our patients want to be told that a trainee is performing a part of their operation but only 58% of respondents felt that surgical trainees, in general, should perform operations as part of their training. There was, however, a clear positive correlation between those patients who felt that surgical trainees should operate as part of their training and their willingness to allow supervised trainees to operate on them (p = 0.002).
Patient perceptions of trainee involvement in their daily care
For the study period, the majority (64.4%) of patients met a registrar or fellow while they were in hospital. Sixteen-point-seven per cent (n = 29/174) of respondents said that they did not meet a registrar or fellow while they were in hospital and 19% (n = 33) of the patients were unsure of whether they had met a trainee or not. This was despite the fact that the registrars and fellows are substantially involved in the care of CRU patients at WDGMC, but logistics sometimes lead to patients not being seen by a trainee while they are in hospital.
If a patient had met a trainee, 60% of these patients felt that this interaction enhanced their care; and none felt that it detracted from their care. This finding links to a positive sentiment about being seen by more than one doctor a day, where 52.3% (91/174) of patients suggested that seeing more than one doctor a day improved their experience.
Additionally, 94% of patients who spoke to the trainee to get more information about their medical condition were satisfied with that conversation.
Discussion
This is the first study exploring patient perceptions of surgical training in the private sector in South Africa. Although a number of international studies have considered both trainee and trainer perceptions across both sectors, our findings are unique because of our private patient sample and the novelty of training in the private sector in South Africa. Our results suggest that the majority of privately insured patients support the surgical training of medical doctors in this context, and they are willing to be participants in the training process. These findings echo those in international studies among similar cohorts.
Notably, international studies of private settings have found that paying patients are firmly in favour of trainee involvement in surgery, and feel that surgical training should take place in the private sector worldwide.2326 Across these studies, up to 90-97% of respondents thought that training should occur in private hospitals and up to 85.7-88% of private patients were willing to allow a supervised trainee to perform part of their operation. These findings are highly relevant, as patients often seek care in the private sector hoping to access the expertise of a specific specialist or medical team, and there may be the assumption that said specialist will perform all requisite surgical procedures in their entirety.2326
Private sector training in South Africa
Our findings are important in the South African context because we have faced uncertainty about patient perceptions of trainees and training programmes in the private sector. There is a need for strong partnerships between the state and private sector to provide maximum and varied training opportunities in South Africa. However, the incorporation of trainees and the promotion of training programmes in private hospitals has been relatively slow. At present, WDGMC is the only South Africa private hospital with a formal training programme. While there may be numerous practical, financial and logistical barriers to implementation of similar hybrid training programmes in South Africa, it is heartening to see that training in the private sector was widely supported among our relatively small sample. This is the case even in the context of privately insured patients who are often seeking medical care at WDGMC in order to access the expertise of a particular specialist. While implementing surgical training programmes in the private sector may remain challenging, our findings tentatively suggest that patients would be supportive of such initiatives.
Implications for training in consulting disciplines in the South African private sector
Surgical procedures carry risks associated with complications, length of stay, the occasional need for re-operation, pain, and long recovery time. Decreasing these risks correlates with the skill and experience of the surgeon.27 Thus, it may be expected that patients do not feel comfortable about the involvement of trainee surgeons in their care.
Our results show that this is not the case at all, and that patients are generally supportive of trainee involvement in their operation provided it is supervised by the consultant specialist.
Private sector hospitals have the ability to create further training opportunities in consulting disciplines such as radiology and critical care.
We are interested as to whether our finding, that a remarkable proportion of private surgical patients support and encourage trainee involvement in their care, could be extrapolated to less invasive disciplines. The main apparent difference between surgical training and training in a consulting discipline is the risk to the patient.
In future, we hope to extend this research into consulting disciplines with a view to understanding whether private patients who are seeing a consulting specialist (where the risk profile is lower) are equally, or more, supportive of training in the private sector.
Doctor availability and access to information
An unexpected advantage of the training setting - seen in the results of our study - was that patients were often seen by more than one doctor a day. This can be explained by the presence of trainees, who are regularly in and out of the wards. The availability of additional doctors facilitated information sharing more readily, timely delivery of laboratory and radiological results, and answering of questions, all of which improved patient perceptions of care.
International studies have reported similar findings, where a majority of respondents stated that a conversation with a trainee improved their understanding of the proposed procedure or their medical condition.28,29 Access to medical expertise and information is an ongoing challenge in healthcare provision worldwide. A demonstrable trend in the academic literature suggests that ready access to information from one's doctor can help to allay uncertainty, promote autonomy and engender a sense of control.30 These are vital to patient wellbeing in a hospital environment where the patient necessarily cedes a large amount of control to health professionals.
Areas for improvement
There are some areas of our training programme which may be improved. For instance, some respondents stated that they did not meet a trainee. This could be accounted for by short length of stay. It may also be explained by our observation that our trainees are sometimes indistinguishable from other medical personnel, or that trainees do not adequately introduce themselves to patients when they engage at the bedside. We are considering ways in which we can make our trainees more visible, for instance by indicating this on their name tag. Given our finding that patients who had met a trainee were more willing to allow a trainee to perform a supervised part of their operation, implementing systems that promote trainee identification should be prioritised, as this may further entrench favourable perceptions of the training programme on offer.
A small number of this patient sample (6/174 respondents) were not satisfied with their conversation with the trainee about their medical condition. We need to ensure that our trainees communicate effectively with the patients and defer to the primary surgeon when they are unsure of how to respond to queries.
It was interesting to note that 8% of the respondents felt that surgical trainees should not perform operations as part of their surgical training. One possible interpretation of the answer to this question is that the public do not have an understanding of how surgical training occurs. Another interpretation may be that the respondents understood the question as implying that the trainees should operate independently while in training. This warrants further investigation.
Study limitations
This study may be limited by the relatively small sample size, and the fact that sampling took place across a single hospital department. Hence, the results of this study may not be readily generalisable. It is also possible that patients who experienced surgical complications may have differing perceptions of trainees in the private sector, and future research could consider mechanisms for exploring these in a sensitive manner.
Conclusion
Private sector medical training (and surgical training in particular) is a novel development in the South African healthcare environment. This study demonstrates that most of the patients seeking care at the WDGMC CRU who did not experience major complications see the value of training programmes in private sector hospitals and are themselves willing to be patients within such a system. Eighty-three per cent of the respondents would allow a supervised trainee to perform a part of their operation.
Moreover, training programmes in this setting appear to enhance the patient experience, particularly by facilitating a wider availability of doctors, and promoting access to information. We are cautiously optimistic that these findings could be used to advocate for expanded surgical and consulting training opportunities across the private sector in South Africa; however, more research is needed to formally establish this.
Acknowledgements
Thank you to the Wits Donald Gordon Medical Centre research office for their assistance with this project. Thank you to Drs Brendan Bebington, Nadine Harran and Daniel Surridge for allowing their patients to participate.
Conflict of interest
The authors declare no conflict of interest.
Funding source
Wits Donald Gordon Medical Centre.
Ethical approval
Ethical approval was obtained from the University of the Witwatersrand Human Research Ethics Committee (M1811122).
ORCID
D Lutrin https://orcid.org/0000-0002-0914-9464
H Etheredge https://orcid.org/0000-0002-2581-5754
J Fabian https://orcid.org/0000-0001-7130-9142
C Bouter https://orcid.org/0000-0001-8814-820X
S Tager https://orcid.org/0000-0002-2086-0345
REFERENCES
1. Sholl S. Balance or tension? Walking the tightrope between training and patient care. Med Educ. 2018;52(3):248-9. https://doi.org/10.1111/medu.13511. [ Links ]
2. Kiran RP, Ahmed Ali U, Coffey JC, et al. Impact of resident participation in surgical operations on postoperative outcomes: National Surgical Quality Improvement Program. Ann Surg. 2012;256(3):469-75. https://doi.org/10.1097/SLA.0b013e318265812a. [ Links ]
3. Jan A, Riggs DR, Orlando KL, Khan FJ. Surgical outcomes based on resident involvement: what is the impact on vascular surgery patients? J Surg Educ. 2012;69(5):638-42. https://doi.org/10.1016/j.jsurg.2012.06.012. [ Links ]
4. Renwick AA, Bokey EL, Chapuis PH, et al. Effect of supervised surgical training on outcomes after resection of colorectal cancer. Br J Surg. 2005;92(5):631-6. https://doi.org/10.1002/bjs.4935. [ Links ]
5. Acheampong DO, Paul P, Guerrier S, Boateng P, Leitman IM. Effect of resident involvement on morbidity and mortality following thoracic endovascular aortic repair. J Surg Educ. 2018;75(6):1575-82. https://doi.org/10.1016/j.jsurg.2018.04.012. [ Links ]
6. Saliba AN, Taher AT, Tamim H, et al. Impact of resident involvement in surgery (IRIS-NSQIP): looking at the bigger picture based on the American College of Surgeons-NSQIP Database. J Am Coll Surg. 2016;222(1):30-40. https://doi.org/10.1016/j.jamcollsurg.2015.10.011. [ Links ]
7. Ferraris VA, Harris JW, Martin JT, Saha SP, Endean ED. Impact of residents on surgical outcomes in high-complexity procedures. J Am Coll Surg. 2016;222(4):545-55. https://doi.org/10.1016/j.jamcollsurg.2015.12.056. [ Links ]
8. Hutter MM, Glasgow RE, Mulvihill SJ. Does the participation of a surgical trainee adversely impact patient outcomes? A study of major pancreatic resections in California. Surgery. 2000;128(2):286-92. https://doi.org/10.1067/msy.2000.107416. [ Links ]
9. Cobb AN, Eguia E, Janjua H, Kuo PC. Put me in the game coach! Resident participation in high-risk surgery in the era of big data. J Surg Res. 2018;232:308-17. https://doi.org/10.1016/j.jss.2018.06.041. [ Links ]
10. Doyon L, Moreno-Koehler A, Ricciardi R, Nepomnayshy D. Resident participation in laparoscopic Roux-en-Y gastric bypass: a comparison of outcomes from the ACS-NSQIP database. Surg Endosc. 2016;30(8):3216-24. https://doi.org/10.1007/s00464-015-4627-6. [ Links ]
11. Uecker J, Luftman K, Ali S, Brown C. Comparable operative times with and without surgery resident participation. J Surg Educ. 2013;70(6):696-9. https://doi.org/10.1016/j.jsurg.2013.06.011. [ Links ]
12. Ross SW, Oommen B, Kim M, et al. A little slower, but just as good: postgraduate year resident versus attending outcomes in laparoscopic ventral hernia repair. Surg Endosc. 2014;28(11):3092-100. https://doi.org/10.1007/s00464-014-3586-7. [ Links ]
13. Papandria D, Rhee D, Ortega G, et al. Assessing trainee impact on operative time for common general surgical procedures in ACS-NSQIP. J Surg Educ. 2012;69(2):149-155. https://doi.org/10.1016/j.jsurg.2011.08.003. [ Links ]
14. Whealon MD, Young MT, Phelan MJ, Nguyen NT. Effect of resident involvement on patient outcomes in complex laparoscopic gastrointestinal operations. J Am Coll Surg. 2016;223(1):186-92. https://doi.org/10.1016/j.jamcollsurg.2016.03.002. [ Links ]
15. Hernandez-Irizarry R, Zendejas B, Ali SM, Lohse CM, Farley DR. Impact of resident participation on laparoscopic inguinal hernia repairs: are residents slowing us down? J Surg Educ. 2012;69(6):746-52. https://doi.org/10.1016/j.jsurg.2012.08.013. [ Links ]
16. Watters DAK, D'Souza B, Guest G, et al. Training in the private sector: what works and how do we increase opportunities? ANZ J Surg. 2009;79(3):138-42. https://doi.org/10.1111/j.1445-2197.2008.04830.x. [ Links ]
17. Koirala R, Mattern O, Danne P, Murray S. Patients' perception of surgical training in private hospitals. ANZ J Surg. 2012;82(7-8):548-50. https://doi.org/104111/j4445-2197.2012.06112.x. [ Links ]
18. Yap R, Cullinan M. Private sector surgical training: feasibility through the lens of appendicectomy. ANZ J Surg. 2017;87(12):993-6. https://doi.org/10.1111/ans.13511. [ Links ]
19. Patel N, Leusink A, Singh N, Koto MZ, Luvhengo T. Registrar perceptions on general surgical training in South Africa: a report by the South African Society of Surgeons in Training (SASSiT). S Afr J Surg. 2018;56(2):10-4. https://doi.org/10.17159/2078-5151/2018/v56n2a2448. [ Links ]
20. Kruger D, Veller M. Exposure to key surgical procedures during specialist general surgical training in South Africa. S Afr J Surg. 2014;52(4):96-100. [ Links ]
21. Dindo D, Demartines N, Clavien P-A. Classification of surgical complications. Ann Surg. 2004;240(2):205-13. https://doi.org/10.1097/01.sla.0000133083.54934.ae. [ Links ]
22. Lutrin DL, Etheredge HR, Oettle GJ, et al. A one year audit of the Colorectal Unit at Wits Donald Gordon Medical Centre: 2016-2017. S Afr J Surg. 2019;57(3):50-4. https://doi.org/10.17159/2078-5151/2019/v57n3a2863. [ Links ]
23. Kempenich JW, Willis RE, Blue RJ, et al. The effect of patient education on the perceptions of resident participation in surgical care. J Surg Educ. 2016;73(6):e111-7. https://doi.org/10.1016/j.jsurg.2016.05.005. [ Links ]
24. Wong LM, Wun LP, Shaw J, Vellar D. The private hospital: a potential surgical training ground. Med J Aust. 2009;191(7):410. https://doi.org/10.5694/j4326-5377.2009.tb02856.x. [ Links ]
25. Cowles RA, Moyer CA, Sonnad SS, et al. Doctor-patient communication in surgery: attitudes and expectations of general surgery patients about the involvement and education of surgical residents. J Am Coll Surg. 2001;193(1):73-80. https://doi.org/10.1016/S1072-7515(01)00936-X. [ Links ]
26. Fiani B, Cathel A, Arshad M, et al. Patient perspectives on the participation of neurosurgery resident physicians in their care. Cureus. 2020. https://doi.org/10.7759/cureus.6880 [ Links ]
27. Birkmeyer JD, Finks JF, O'Reilly A, et al. Surgical skill and complication rates after bariatric surgery. N Engl J Med. 2013;369(15):1434-42. https://doi.org/10.1056/NEJMsa1300625. [ Links ]
28. Bryan AF, Bryan DS, Matthews JB, Roggin KK. Toward autonomy and conditional independence: a standardised script improves patient acceptance of surgical trainee roles. J Surg Educ. 2020;77(3):534-9. https://doi.org/10.1016/j.jsurg.2020.01.015. [ Links ]
29. Wojcik BM, Phitayakorn R, Lillemoe KD, Chang DC, Mullen JT. Preoperative disclosure of surgical trainee involvement: Pandora's box or an opportunity for enlightenment? Ann Surg. 2017;265(5):869-70. https://doi.org/10.1097/SLA.0000000000002136. [ Links ]
30. Bernat JL, Peterson LM. Patient-centered informed consent in surgical practice. Arch Surg. 2006;141(1):86. https://doi.org/10.1001/archsurg.141.1.86. [ Links ]
 Correspondence:
Correspondence:
C Bouter
Email: carolynbouter@outlook.com


{kind=link}