










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.59 n.2 Cape Town Jun. 2021
http://dx.doi.org/10.17159/2078-5151/2021/v59n2a3423
CASE SERIES
Magnetic resonance imaging features of dermatofibrosarcoma protuberans; what the surgeon should know: a case series
V Sitela; N Khan
Department of Radiology, Kalafong Hospital, University of Pretoria, South Africa
SUMMARY
Dermatofibrosarcoma protuberans (DFSP) is a rare, slow-growing, spindle cell neoplasm with low to intermediate grade malignant potential, commonly found in young and middle-aged adults, more in males than females. DFSP mostly originates in the dermis; rarely, it may be located in the deeper tissues without dermal involvement. Typically, DFSP appears as a multinodular mass, which then spreads into the subcutaneous tissues and muscle; it rarely dedifferentiates to high-grade fibrosarcoma, and more rarely, it may metastasise. We describe magnetic resonance imaging (MRI) features in three female patients with histologically proven DFSP and review the literature.
Introduction
DFSP is a rare tumour that grows with finger-like projections. Adequate and appropriate preoperative imaging is required to visualise these extensions and determine the extent of the tumour. Imaging features are not specific and may be confused with other pathologies such as benign peripheral nerve sheath tumour (BPNST). Characteristic location (extremities, chest, head and neck) and shape should prompt inclusion of this condition in the differential diagnosis of a soft tissue tumour. MRI is effective for determining the extent of tumour penetration and involvement of deeper structures prior to surgery and is also useful in the assessment of atypical lesions or recurrent disease. We describe the MRI features in three cases of histologically proven DFSP.
Materials and methods
Patients with features of DFSP, identified from the MRI registry between 2016 and 2018, were included. Clinical records were retrieved from the hospital medical filing system.
MRI was performed on 1.5Tesla Philips Multiva unit (Netherlands). Routine protocol in our department for soft tissue tumours includes T1- and T2-weighted sequence in axial, coronal and sagittal planes, and a short tau inversion recovery (STIR) sequence in the axial plane. Diffusion-weighted imaging (DWI) was not part of the protocol; postcontrast imaging was included for aggressive lesions and to exclude deeper invasion, perivascular and perineural spread. Contrast agent (Gadolinium DTPA; Magnevist; Schering AG) was administered at a dose of 0.1 mmol/kg. Signal characteristics of DFSP on MRI were compared with those of muscle and fat. Anatomical location, size and depth as well as definition of the lesions were assessed.
A staging computerised tomography (CT) was done to exclude regional and distant metastases.
Results
Four patients, three female and one male, were identified from the MRI registry. DFSP was confirmed histolog-ically in three patients. In the fourth patient, the histology demonstrated a BPNST. This patient was excluded from the series.
The study cohort, therefore, consisted of three patients whose age ranged from 27 to 82 years. All patients were female. Staging CT imaging did not demonstrate metastases in any of these patients.
Case no 1
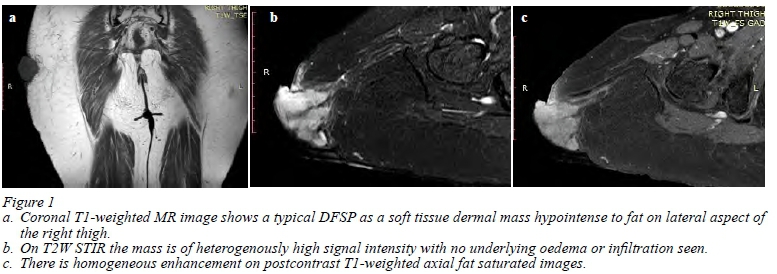
An 82-year-old female patient presented with four-month history of a right thigh mass and intermittent bleeding from the mass. Clinically there was a hard multilobulated reddish-brown mass, freely mobile over the underlying soft tissue structures. A clinical diagnosis of DFSP was made. MRI was requested to assess the extent and underlying local infiltration.
MRI findings
A well-defined multilobulated soft tissue mass arising from the dermal and subcutaneous tissues of the right superior lateral thigh was noted. There was a clear plane of separation from the underlying muscle. No bone or vascular infiltration was seen. This mass had MRI characteristics of a typical DFSP, i.e., isointense to skeletal muscle and hypointense to fat on coronal T1-weighted; hyperintense to skeletal muscle on T2-weighted (not shown) and on axial STIR; homogenous enhancement on postcontrast axial T1-weighted sequence (Figure 1a, b & c) respectively.
Case no 2
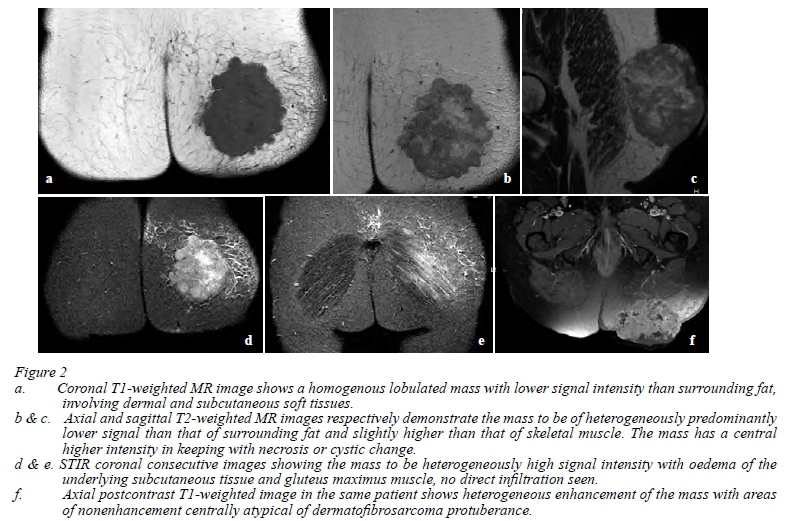
A 63-year-old immunocompromised female patient on anti-retroviral medication presented with an ill-defined left buttock mass involving the dermis. Superficial ulceration and bleeding were noted. The mass appeared fixed to the underlying soft tissues. Clinically an aggressive soft tissue tumour was suspected, and multiple tru-cut biopsies were taken. MRI was requested post-biopsy to assess the extent and infiltration of the underlying muscle and bone.
MRI findings
A well-defined lobulated soft tissue mass with mixed solid and cystic components and infiltration of the subcutaneous fat was noted in the dermis of the left buttock. There was a clear plane of separation with the gluteus maximus muscle which appeared oedematous. The underlying bone was intact. The mass was isointense to muscle and hypointense to surrounding fat on coronal T1-weighted images (Figure 2a), and heterogeneous with central higher signal than skeletal muscle on T2-weighted axial and sagittal images, respectively (Figure 2b & c). The mass was heterogeneous with areas of high intensity and a central higher signal intensity compared to subcutaneous fat in keeping with cystic change/necrosis noted on coronal STIR sequence (Figure 2d & e). There were areas of blooming on T2 Fast Field Echo (FFE - not shown) suggestive of haemorrhage secondary to biopsy. There was heterogeneous enhancement on postcontrast axial images (Figure 2f). Due to the heterogeneity of the tumour on T2-weighted and STIR, the differential diagnosis included a soft tissue sarcoma, lymphoma and atypical DFSP.
Case no 3
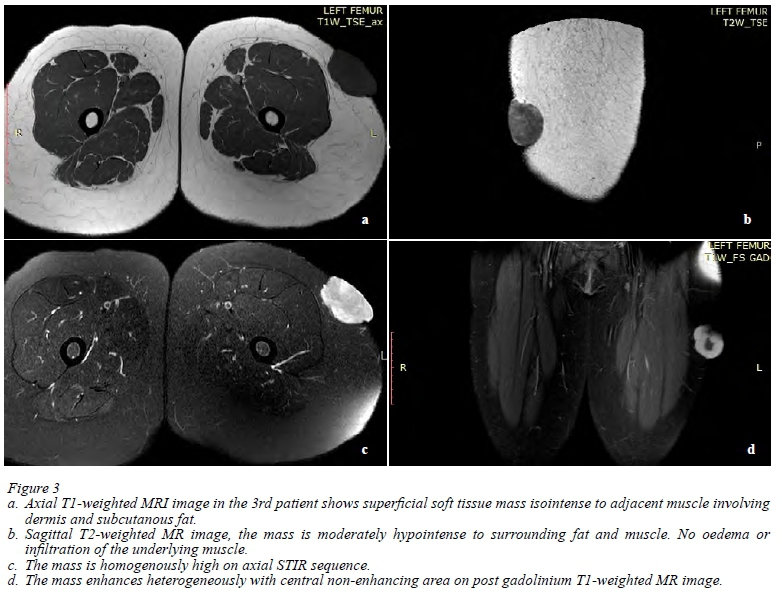
A 27-year-old female presented with an enlarging mul-tilobulated soft tissue mass involving the dermis of the left thigh. Clinical features were in keeping with a possible DFSP. This was confirmed on histology.
MRI findings
A superficial well defined exophytic mass was noted arising from the dermis on the anterolateral aspect of the left thigh. There were no signs of deeper extension. It was isointense to surrounding muscle and hypointense to fat on T1-weighted images (Figure 3a), moderately hypointense compared to fat on the T2-weighted sagittal image (Figure 3b), homogenously high on axial STIR (Figure 3c) and showed heterogeneous avid enhancement with a non-enhancing area anteriorly on post Gadolinium coronal T1-weighted images (Figure 3d). The findings of hypointensity on T2-weighted, and heterogeneous postcontrast enhancement were atypical of a DFSP. Histology confirmed the diagnosis of DFSP.
The fourth case was excluded based on MRI features typical of BPNST: a fusiform shape and the presence of a target sign. The diagnosis was confirmed on histology.
Discussion
DFSP is an uncommon spindle cell tumour originally described in 1924 by Darier and Ferrand. The term "dermatofibrosarcoma protuberans" was given by Hoffman in 1925 and remains in use.1,2 DFSP is described as a rare, infiltrative, locally aggressive, slow-growing neoplasm with low to intermediate grade malignant potential that has mostly been described in young and middle-aged adults with a male preponderance.1,3 It usually remains in the dermis as a plaque or a protuberant mass but in more aggressive lesions may extend into the subcutaneous tissue with involvement of the underlying fat and muscle.1 The cure rate after surgery is excellent.; DFSP rarely metastasises, but chances of local recurrence are high in cases of atypical and deep lesions.3,4 Fifty per cent of DFSP arise in the trunk; the rest in the extremities (20-30%) and head and neck region (10-15%). The size of the DFSP may vary from 1 cm to 25 cm.1,3,4 DFSP mostly arises in the normal skin but has been described to arise in the area of a scar, after repeated trauma, a vaccination site or following radiation.1,4 Clinical diagnosis of the lesion is not always possible and open biopsy, either excisional or incisional, is the diagnostic method of choice.
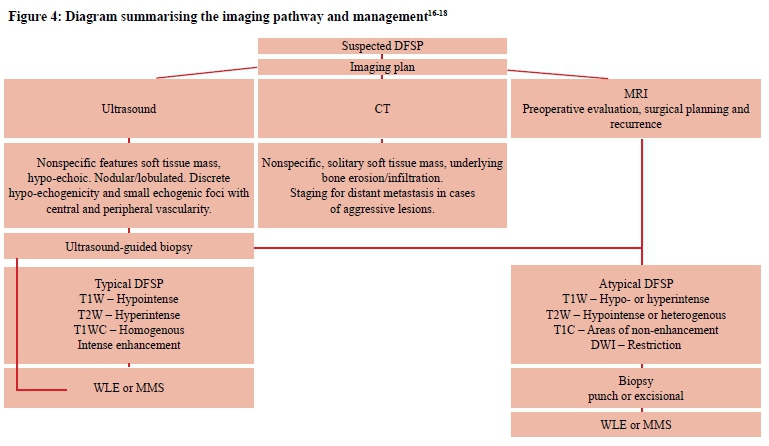
Ultrasound, CT imaging and MRI are the most commonly utilised imaging modalities for diagnosing and assessing DFSP.5-9 Ultrasound examination, although not specific, may also be useful, mainly for the detection of smaller lesions.5-9 Sonographically, DFSP typically presents as a well-defined subcutaneous lesion which may be mildly lobulated, hypoechoic with discrete areas of increased hypo-echogenicity together with small echogenic foci, central and peripheral vascularity as well as posterior enhancement.5,7,9,10 Ultrasound diagnosis is suspected on the strength of multiple ultrasound features in conjunction with the clinical presentation and not on the basis of one or two features only.
CT imaging is used for anatomical location, determination of underlying bone involvement or calcifications, and for staging purposes in suspected aggressive cases. These cases, particularly if the lesions are advanced or recurrent, may harbour pulmonary metastases.5,6 Chest radiography should be performed for all patients and CT imaging reserved for advanced stage tumours.
MRI is used to evaluate larger and atypical lesions, assess local extension and is essential for preoperative planning.3,5,11 It is considered more accurate than Doppler ultrasonography or CT imaging.5
Clinically, the history is that of a superficial, firm reddish-brown to bluish lesion that may remain small and stable or at times show a rapid aggressive growth pattern with ulceration and bleeding.1,6,8 DFSP accounts for ap-proximately 6% of soft tissue tumours. Large lesions can infiltrate subcutaneous tissue and involve the deep structures; rarely DFSP may arise de novo in the subcutaneous tissue without dermal involvement.6-8,10 Two primary groups have been described, namely "classic" protruding DFSP with elevation or protrusion, and "non-protuberans" DFSP with atrophy or depression. A case of pedunculated DFSP believed to be a neurofibroma or fibroepithelioma on clinical grounds has also been reported.7,9 According to a study by Ramakrishnan et al., as quoted by Shih et al., DFSP is considered deep, yet not involve the dermis, if it is 0.4-1 cm deep to the dermal surface;9,10 however, Torreggiani et al. identified a mean depth of 17 mm.3 The fourth case in our series was clinically challenging as it presented as a subcutaneous mass without dermal involvement similar to the lesion reported by Ramakrishnan et al., as quoted by Shih et al.9 Clinically, there was no neurological involvement. The differential diagnosis included a deep DFSP, BPNST or other benign mesenchymal tumour. MRI features were typical of a BPNST, which was confirmed on histology. The first patient in our series had typical MRI features of a DFSP while the second and third cases were considered atypical because of the presence of cystic changes, heterogeneous enhancement, central non-enhancement and low signal on T2-weighted sequence. Tumour was considered superficial in all cases, i.e., mainly involving dermal and subcutaneous tissues with associated bulging into the dermal surface.
DFSP can be multiple and coalesce to form an indurated plaque which is often violaceous clinically.3,7 It may grow asymmetrically in a horizontal or vertical frond-like growth pattern into subcutaneous tissues. It rarely infiltrates the investing fascia to extend into sub fascial tissues.7-9,11 DFSP rarely demonstrates perineural spread, or is associated with nodal or distant metastases; however, deeper lesions may erode the underlying bone.3
MRI is the preferred imaging modality of choice for soft tissue tumours due to the high soft tissue contrast resolution. It is frequently performed as part of the workup of DFSP to evaluate larger or atypical primary lesions or recurrent disease. MRI has greater sensitivity than palpation for detecting the depth of infiltration. MRI has been proposed for the delineation of DFSP, allowing accurate localisation before surgery.3,5,6,10-13 Galant et al. reported on the use of MRI to evaluate the location of soft tissue masses relative to the superficial fascia. Although their group of 64 patients did not include any cases of DFSP, they reported that subcutaneous lesions crossing the superficial fascia presented with a 6.88 times greater risk of malignancy than lesions that did not cross the fascia.14 A tumour that is close to investing fascia should be removed en bloc to reduce the chance of recurrence.7
MRI protocol includes three sequences: T1-weighted, T2-weighted and STIR sequence. Gadolinium is not routinely used but is employed if an alternate diagnosis is suspected, as in two of our cases. An intravenous dose of 0.1-0.2 mmol/ kg of contrast agent (Gadolinium DTPA) is administered to patients undergoing contrast-enhanced MRI. DFSP is usually intermediate to hypointense to fat and skeletal muscle on T1-weighted and hyperintense on T2-weighted sequence. It demonstrates marked enhancement on post-gadolinium T1-weighted images. STIR sequence with an inversion time of 150 msec provides fat suppression allowing clear definition of the tumour.3,5,6,8,10 Two of the cases in our series had atypical heterogeneous MRI appearance as described above. DWI is an MRI technique providing information on the mobility of water protons and for assessing tumour cellularity. It aids in the differentiation of tumour involvement from reactive oedema. Tumour infiltration within the fascia shows persistent hyperintensity on high b-value DWI and appears hypointense on apparent diffusion coefficient (ADC) maps due to diffusion restriction. This may help differentiate tumour infiltration from reactive oedema in cases of fascial involvement and recurrence after surgery.11 Kransdorf and Meis-Kindblom described four patients out of a total of 11 patients in their series who underwent MRI. The tumour in these four cases was described as a well-defined soft tissue neoplasm on MRI with low signal on T1-weighted images and higher than fat on T2-weighted sequences. The tumour in one case had areas of high signal on T1-weighted sequence compatible with that of haemorrhage.8
A study by Torreggiani et al. showed similar MRI characteristics of DFSP as described by Kransdorf and Meis-Kindblom, predominantly high signal on T2-weighted and STIR, low or intermediate signal on T1-weighted, and either uniform or patchy pattern of enhancement.3
While MRI is excellent in determining the anatomical extent of the lesion, its ability to characterise soft tissue lesions is limited and a differential diagnosis should be considered. Differential diagnoses that can be confused with DFSP include dermatofibroma, epidermal cyst, peripheral nerve sheath tumour, nodular fasciitis, cavernous haemangioma, liposarcoma, nodular type melanoma, and mycosis fungoides.3,4,6,9,10 Although dermatofibroma has similar imaging features as DFSP, it is seen most frequently on the extremities, whereas DFSP is most common on the trunk. Epidermal cyst does not enhance on postcontrast scans; peripheral nerve sheath tumours are closely associated with a nerve and have a classical split fat or fascicular or target sign, as was seen in our fourth case. Plexiform neurofibromas are diffuse and asymmetric, whereas DFSP is nodular. Nodular fasciitis favours the upper extremity and has an enhancing fascial tail sign. Cavernous haemangiomas have calcifications which is not a feature of DFSP, and liposarcomas contain fat which is also not a feature of DFSP. Nodular type melanoma is mostly blue to black on clinical examination, whereas DFSP is often violaceous. Mycosis fungoides is the cutaneous form of T-cell lymphoma and has other features of lymphoma not seen in DFSP.4,6,7,9
In the majority of cases, local recurrences of DFSP occur within the first three years of resection, with approximately half of these patients presenting within the first year of surgery, but recurrence has been reported up to five years later.4-610 It is therefore important to follow these patients up over a longer period. Distant metastases are rare and occur in less than 2-4% of cases. The 5-year disease-specific survival rate is over 95%.4513 The most important clinical feature of DFSP is its locally aggressive growth and a tendency for local recurrence (20-50%) after simple excision.4-6,8 Tumour recurrence is characterised by the presence of a discrete nodule or mass, with typically prolonged T1 and T2-weighted relaxation times.4-68 It has been hypothesised that if the tumour has specific findings such as high intensity in T2-weighted imaging or enhancement on Tl-weighted images (including invasion of fascia or muscle) and nodules in the capsule of the tumour, the potential for recurrence is higher. However, if the tumour displays well-defined borders the incidence of recurrence is lower after resection.3,4
It is sometimes difficult to assess the clinical extent of DFSP. Microscopic tumour has been detected 0.3-12 cm beyond the macroscopic tumour margins. Infiltration can extend to muscle and even tendons. Preoperative MRI has been shown to facilitate surgical planning and assess the extent of tumour invasion and degree of involvement of critical structures.13,15,16
Surgical techniques include wide local excision (WLE) with tumour free margins and Mohs micrographic surgery (MMS). Wide resection involves a three-dimensional excision including normal skin, subcutaneous tissue and underlying investing fascia with a 2-4 cm margin from the gross tumour boundary and is the standard treatment for DFSP. All patients in our series underwent wide excision of the lesions.16-18 Although WLE is a simple procedure, it does not permit intraoperative evaluation of surgical margins and is consequently associated with a higher rate of recurrence compared to MMS.17,18 MMS is a surgical technique where thin layers of tissue are removed and histologically analysed to ensure a negative margin.10,15,16 Some authors propose that MMS reduces the amount of tissue resected and lowers the recurrence rate to around 1%,1,4,6,9,16-18 as it allows entire margins of surgically removed tissue to be studied histologically. It is considered the treatment of choice for DFSP.15,16 Radiation and treatment with imatinib, a tyrosine kinase inhibitor, has been used to treat unresectable, recurrent or metastatic DFSP prior to surgery.4
Study limitations
Retrospective analysis with limited cases and restricted MR imaging, DWI was not utilised to assess fascial involvement.
Conclusion
DFSP is a rare soft tissue tumour characterised by asymmetrical and poorly defined growth. MRI is useful in determining the site of tumour origin, its extent, relation to adjacent anatomic structures, and for follow-up after therapy as well as in cases of disease recurrence. Knowledge of DFSP imaging characteristics may alert radiologists to include it in the differential diagnosis of lesions with similar imaging characteristics. Our cases were unique, as all were female, one was much older than the age stipulated in the literature and two had atypical MRI features.
Conflict of interest
The authors declare no conflict of interest.
Funding source
None.
Ethical approval
Ethical approval for publication of case series was received from University of Pretoria and Kalafong Hospital number: 284/2019.
ORCID
V Sitela https://orcid.org/0000-0002-8454-7075
N Khan https://orcid.org/0000-0002-5393-239
REFERENCES
1. Oswald G Costa. Progressive recurrent dermatofibroma (Darier-Ferrand) Anatomoclinical study. Arch Derm Syphilol.1946;54(4):432-54. [ Links ]
2. Hoffmann E, Ueber das knollentribende Fibrosarkom der Haut (dermatofibrosarcoma protuberans). Dermatol Z. 1925;43:1-28. (abstract only) [ Links ]
3. Torreggiani WC, Al-Ismail K, Nicolaou S, O'Connel JX, Knowling MA. Dermatofibrosarcoma protuberance: MR imaging features. AJR. Am J Roentgenol. 2002;178(4):989-93. [ Links ]
4. Millare GG, Guha-Thakurta N, Sturgis EM, El-Naggar AK, Debnam JM. Imaging findings of head and neck dermatofibrosarcoma protuberans. AJNR. 2014;35(2):373-8. [ Links ]
5. Goto H, Iwama Y, Kusinada M, et al. Imaging features of dermatofibrosarcoma protuberance with pathologic correlation and assessment for recurrence potential. ESR. 2013;C-2331. https://doi.org/10.1594/ecr2013/C-2231. [ Links ]
6. Zhang L, Liu QY, Cao Y, Zhong JS, Zhang WD. Dermatofibrosarcoma protuberans: computed tomography and magnetic resonance imaging findings. Medicine. 2015 Jun;94(24):e1001. https://doi.org/10.1097/MD.0000000000001001. [ Links ]
7. Lee RK, Griffith JF, Ng AW, Mac-Moune Lai F. Ultrasound appearances of dermatofibrosarcoma protuberans. J Med Ultrasound. 2013;21:21-8. [ Links ]
8. Kransdorf MJ., Meis-Kindblom JM. Dermatofibrosarcoma protuberans: radiologic appearance. AJR. 1994;163:391-4. [ Links ]
9. Shih P-Y, Chen C-H, Kuo T-T, et al. Deep dermatofibrosarcoma protuberans: a pitfall in the ultrasonographic diagnosis of lipoma-like subcutaneous lesions. Dermatologica Sinica. 2010;28:32-5. [ Links ]
10. Mujtaba B, Wang F, Taher A, et al. Dermatofibrosarcoma protuberans: pathological and imaging review. Curr Probl Diagn Radiol. 2020 Jun 1;50(2):236-40. [ Links ]
11. Yoon MA, Chee CG, Chung HW, et al. Added value of diffusion - weighted imaging to conventional MRI for predicting fascial involvement of soft tissue sarcomas. Eur Radiol. 2019:29;1863-73. [ Links ]
12. Martin L, Piette F, Blanc P, et al. Clinical variants of the preprotuberant stage of dermatofibrosarcoma protuberans. Br J Dermatol. 2005;153:932-6. [ Links ]
13. Riggs K, McGuigan KL, Morrison WB, et al. Role of magnetic resonance imaging in perioperative assessment of dermatofibrosarcoma protuberans. Dermatologic Surgery. 2009;35:2036-41. [ Links ]
14. Galant J, Marti-Bonmati L, Soler R, et al. Grading of subcutaneous soft-tissue tumours by means of their relationship with the superficial fascia on MR imaging. Skeletal Radiol. 1998;27:657-63. [ Links ]
15. Bergin P, Rezaei S, Lau Q, Coucher J. Dermatofibrosarcoma protuberance, magnetic resonance imaging and pathological correlation. Australas Radiol. 2007 Sept 14;51(S1):B64-6. https://doi.org/10.1111/j.1440-1673.2007.01762.x. [ Links ]
16. Serra-Guillen C, Sanmartin O, Llombart B, et al. Correlation between preoperative magnetic resonance imaging and surgical margins with modified Mohs for dermatofibrosarcoma protuberans. Dermatologic Surgery. 2011;37:1638-45. [ Links ]
17. Llombart B, Serra C, Requena C, et al. Guidelines for diagnosis and treatment of cutaneous sarcomas: dermatofibrosarcoma protuberans. Actas Dermosifilogr. 2018;109(10):868-77. [ Links ]
18. Hao X, Billings SD, Wu F, et al. Dermatofibrosarcoma protuberans: update on the diagnosis and treatment. J Clin Med. 2020;9:1752. [ Links ]
 Correspondence:
Correspondence:
N Khan
Email: nausheen.khan@up.ac.za


{kind=link}
{kind=link}
{kind=link}
{kind=link}