










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.59 n.2 Cape Town Jun. 2021
http://dx.doi.org/10.17159/2078-5151/2021/v59n2a3417
TRAUMA
Intensive care unit hospitalisation costs associated with road traffic crashes at a central hospital in KwaZulu-Natal for the 2017/18 financial year
RC PillayI; Y KistaI; TC HardcastleII, III; O MahomedI
IDepartment of Public Health Medicine, School of Nursing and Public Health, Howard College, South Africa
IITrauma Service, Inkosi Albert Luthuli Central Hospital, South Africa
IIIDepartment of Surgery, Nelson R Mandela School of Clinical Medicine, University of KwaZulu-Natal, South Africa
ABSTRACT
BACKGROUND: The financial and physical impacts of road traffic crashes are borne by the individual, the extended family, society, the health sector and the economy of the country. The main contributors to these costs are the loss of productivity and the accrual of ongoing healthcare costs over a long-term period. There is limited information available on the cost of admitting seriously injured patients post accidents to a central hospital intensive care unit
METHODS: Cost data was obtained from the electronic database for all patients admitted for more than 24 hours to the trauma intensive care unit at Inkosi Albert Luthuli Central Hospital. A mixed costing approach was used. Data was collected on surgical procedures, imaging, laboratory tests, trauma receiving fees, pharmaceuticals, goods and services and compensation of employees
RESULTS: The total cost of treating road traffic crash patients for the 2017/18 financial year equated to R21 140 475.49. The three main cost drivers comprised the compensation of employees (R12 135 848.41; 57.4%), goods and services (R5 083 182.12; 24%) and surgery costs (R1 429 321.00; 6.8%). The average cost per admission was R163 879.65, with the average cost per inpatient day equating to R12 727.56. Male patients admitted from motorcycle crashes had the highest cost per admission, followed by motor vehicle crashes and pedestrian vehicle crashes
CONCLUSION: The cost and burden associated with road traffic crashes is reflective of national and international trends and will require a comprehensive strategy to reduce accidents as well as better management at the scene and at lower levels of care
Keywords: road traffic crashes, cost per admission, cost per inpatient day, trauma intensive care
Introduction
Globally, road traffic fatalities and injuries are estimated to cost low- to middle-income countries (LMICs) approximately 3% of their gross domestic product (GDP). Data from the World Health Organization (WHO) suggests that road traffic fatalities and injuries account for approximately 5% of a country's GDP, however, road traffic crash (RTC) fatalities in SA accounted for 7.8% of GDP in 2013.1 The cumulative cost of RTCs in South Africa for 2015 was an estimated R142.95 billion, which was approximately 3.4% of South Africa's GDP.2
The cost per patient for fatal RTCs amounted to approximately R5.4 million in 2015.2 A publication by the Road Traffic Management Corporation in 2016 found the total cost of major and fatal RTCs to be R765 664 and R5 435 261, respectively, using the human capital approach. Medical costs were estimated at R110 656 and R147 143 for major and subsequently fatal RTCs, respectively.2 Serious injuries were estimated at approximately R760 000 per patient. These costs factored in the loss of future earnings, cost of pain and suffering, incident and vehicle repair costs.2
A review of injury and trauma costs in LMICs found that the median of direct medical, direct non-medical and indirect cost per injury was US$4 200 (US$355-10 300), with the median direct medical costs related to RTCs to be US$140 (US$99-720) per hospitalisation.3 A costing study was done at a regional hospital in KwaZulu Natal in 2013 on RTC patients where the researchers found the cost per patient to be US$6 988. This was noted to be an under-estimation of the total cost as fixed variables such as land, building and staff salaries were excluded.4
The financial and physical impacts of RTCs are borne by the individual, the extended family, society, the health sector as well as the economy of the country. From a macro-economic perspective, the biggest contributors to these costs are the loss of productivity of the individual as well as the accrual of ongoing healthcare costs over a long-term period.5 In addition, RTCs have a detrimental impact in many LMICs as it influences households by directly affecting breadwinners, causing additional cost of healthcare to the injured and may even require additional care for those permanently disabled by RTCs casting strain on the health, legal and insurance systems.2
There is limited information about the direct medical costs of RTCs on the public healthcare sector in SA, including emergency and health costs. The economic drain as well as the economic potential that is lost, which is estimated at 'billions of Rand per annum' is also unclear.6 From a health services perspective, there is very little consolidated information on the cost of major trauma associated with RTCs requiring intensive care admission. This study aims to fill this gap by determining the cost of treating RTC patients admitted at an intensive care unit at a quaternary hospital in KwaZulu-Natal for the 2017/18 financial year.
Methods
Study design
The study was a retrospective cost analysis using a mixed costing approach. Gross-costing or the top-down approach estimates the cost per patient by retrospectively obtaining the total cost of resources consumed. Micro-costing or the bottom-up approach, on the other hand, collects all resources utilised by the patient and adds all individual costs to achieve a total cost. The latter option is found to be the most accurate, however, it is more time-consuming than the former option.7 Micro-costing is noted to over-estimate the costs assessed, whereas gross-costing is noted to underestimate them.8 Top-down cost approaches are generally used in LMICs, however, a mixed costing methodology can be a suitable alternative due to the lack of availability of data. A mixed methodology approach allows the use of all available data sources and balances accurate micro-costing approaches with feasible gross-costing approaches.9
Study perspective
The study perspective was from a health provider perspective with the unit of analysis being the hospital cost of treating RTC patients in a trauma intensive care unit (TICU) at a quaternary hospital in KwaZulu-Natal.
Study location and site
The study was conducted at the TICU of Inkosi Albert Luthuli Central Hospital (IALCH), which is a central and tertiary care referral institution. The TICU, a 10-bed facility, is a level 1 trauma unit that manages immediate life-threatening injuries. The catchment area for IALCH is the whole of KwaZulu-Natal and approximately 50% of the Eastern Cape. IALCH is one of ten central hospitals in SA.
Study population
The study population included all RTC patients (adults and children) admitted to TICU at IALCH for more than 24 hours for the period from 1 April 2017 to 31 March 2018.
Information for the TICU inpatients was extracted from the electronic database. Patient clinical records were reviewed to identify patients admitted post RTCs. A data collection tool developed by the researcher was used to record the information. This data collection tool included a micro-costing section including costs such as imaging, laboratory tests, a trauma receiving cost as well as surgical procedures performed (including the facility fee, the anaesthetic costs and the surgeon's fee). A gross-costing section included costing of the compensation of employees, pharmaceutical costs and the cost of goods and services. Pharmaceuticals were noted as a gross-cost as this was sourced from the TICU cost centre along with the other gross-costing information.
The invoices for these patients were then obtained from the billing department to identify the micro-costing components with the unit prices noted. The finance department was contacted to obtain the TICU cost centre information noted as the gross-costing information. The information was transferred to a self-developed data collection tool.
Data analysis
All data was recorded on a Microsoft Excel® (Microsoft Corp, Redmund WA) spreadsheet and analysed. Costs were calculated as components, i.e., imaging, laboratory tests, trauma receiving fee and surgery costs using the bottom-up method. These costs totalled the micro-costing component. Compensation of employees, pharmaceuticals as well as goods and services were calculated using the gross-costing method, which once accumulated, was divided by the total number of inpatient days in the TICU and multiplied by each RTC patient's length of stay (LOS) in the unit and this equated to the total gross-costing fee per patient. Together the micro-costing and gross-costing totals added to the total amount utilised by RTC patients in the TICU. The cost per admission was the summation of each component cost per RTC patient. The average cost per inpatient day for RTC patients was the total cost of all the RTC patients divided by the total LOS of RTC patients. No discounting was applied to any of the costs as actual 2017 prices were used. A sensitivity analysis was conducted to test the robustness of the costs.
Results
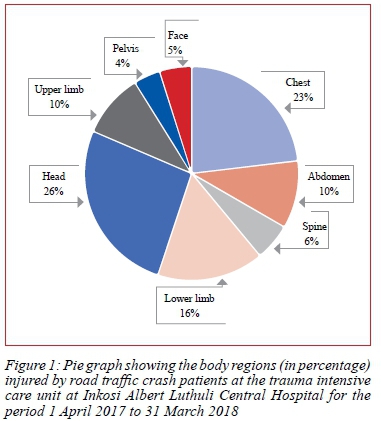
During the period of 1 April 2017 to 31 March 2018, there were 129 RTC patients admitted to TICU, who met the inclusion criteria and represented approximately 48% (129/269) of the total admissions to the unit. The study population comprised of 96 males (74%), with a median age of 30 years (interquartile range [IQR] 19-39 years). There were 372 injuries sustained by 129 RTC patients with the most commonly injured areas being the head 26% (98/372) and chest 23% (86/372) (Figure 1). The mean LOS was 12.9 days (standard deviation [SD] 13.2 days) with the injury severity score (ISS) ranging from 4-68, with a median score of 34 (IQR 26-43) noted, indicative of a severe injury cohort (ISS > 25).
Cost analysis
Total and component costs
The total cost of treating RTC patients at TICU IALCH for the 2017/18 financial year was R21 140 475.49. Gross costs represented 86% (18 173 393.92/21 140 475.49) of the total RTC cost (Table I). The biggest cost driver was the compensation of employees R12 135 848.41 (57.4%). This cost of staff comprised of permanently employed TICU doctors (i.e., medical officers and consultants), nurses and administration clerks. Goods and services totalled R5 083 182.12 (24%) including items such as gloves, catheters, wound dressings, syringes, stationery, telephonic billing, crutches, etc. Pharmacy costs which amounted to R954 363.39 (4.5%) included medication, intravenous fluids, intravenous feeds and blood vaccines.
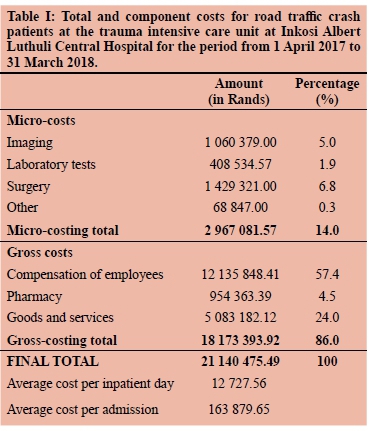
Patient activity related costs in this study represented 14% (2 967 081.57/21 140 475.49) of the total RTC cost (Table I). Surgery was the highest micro-costing component, R1 429 321.00 (6.8%) and included the surgeon, anaesthetist, and facility fees. This was followed by imaging, R1 060 379.00 (5%) and laboratory investigations R408 534.57 (1.9%). Trauma receiving costs contributed a mere R68 847.00 (0.3%) of the overall total. This was the cost on presenting to the TICU for admission and resuscitation as the TICU has its own receiving area. The average cost of treating a RTC patient per day was R12 727.56. The average cost per admission was calculated as R163 879.65.
Comparison between motor vehicle crashes, pedestrian vehicle crashes and 'other'
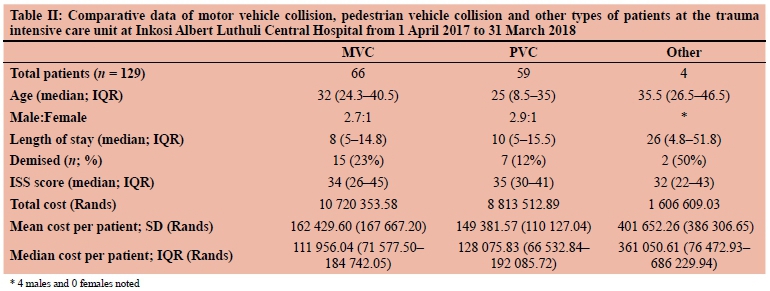
The most common type of RTC were motor vehicle crashes (MVCs) (51.1%), with an age range from 5-65 years. Males represented 73% of these patients with a median LOS of 8 days (IQR 5-14.8 days). This cadre of patients had a median ISS of 34 (IQR 26-45) and a 23% (15/66) mortality rate. The mean and median costs of MVC patients were R162 429.60 (SD R162 667.20) and R111 956.04 (IQR R71 577.50-R184 742.05), respectively.
The study population comprised of 59 pedestrian vehicle crash (PVC) patients, with a median age of 25 years (IQR 8.5-35 years). Seventy-five per cent of PVC patients were male with a median LOS of 10 days (IQR 5-15.5 days). The median ISS for PVC subjects was 35 (IQR 30-41), with a mortality rate of 12%. The mean and median costs of treating a PVC patient was R149 381.57 (SD R110 127.04) and R128 075.83 (IQR R66 532.84-R192 085.72), respectively (Table II).
The 'other' category was all male, motorcycle users, totalling four patients. The median age was 35.5 years (IQR 26.5-46.5 years) with a median LOS of 26.4 days (iQR 4.8-51.8 days). The median ISS was 32 (IQR 22-43), with a 50% mortality rate. The mean and median costs of treating these patients were R401 652.26 (SD R386 306.65) and R361 050.61 (IQR R76 472.93-R686 229.94), respectively (Table II).
Sensitivity analysis
Cost estimates are subject to a degree of uncertainty. Two scenarios were identified to eliminate uncertainty in this costing study. The sensitivity analysis in scenario 1 shows the low IQR cost of the micro-costing components whilst the gross-costing components were unchanged. In scenario 1 the cost per RTC patient per inpatient day was R10 944.80 (Figure 2).

The sensitivity analysis in scenario 2 shows the high IQR cost of the micro-costing components whilst the gross-costing components were unchanged. The cost per RTC patient per inpatient day was R10 961.40 (Figure 2).
Discussion
The total cost of treating RTC patients at TICU IALCH for the study period represented 0.87% of the total IALCH budget, in contrast to a 2016 Iranian study which found the cost of RTCs to be 7.4% of the total hospital expenditure. Notably, the sample size in the latter study was approximately nine times higher than the IALCH study population and the authors noted the average cost of RTC patients to be approximately 11 times higher than that of other categories of patients in their facility, however, they examined "all comers" and not only the ICU subset.10 Further costing disparity was noted in a 2018 study in a SA tertiary hospital in Mpumalanga with the cost of RTC patients representing 2.4% of their hospital's expenditure, once again including all patients and not only the "severely injured" cohort.11 This percentage was higher than the current study and is most likely representative of the different hospital expenditures based on the type of health facility (i.e., a tertiary hospital versus a central quaternary hospital) or the patient cohort under review. IALCH's expenditure was approximately fives times higher than the hospital expenditure at the Mpumalanga facility.
Comparing these costs to other studies proved not to be a straightforward task due to the different variables noted. A systematic review of costing injury and trauma in several LMICs found that it was difficult to compare prices globally as current data is "country and context-specific".3
Imaging (5%), laboratory tests (1.9%), surgery (6.8%) and a trauma receiving cost (0.3%) accounted for 14% of the total cost of treating RTC patients for the 2017/18 financial year. A study conducted at a tertiary hospital in Mpumalanga in 2018 found, in contrast, that the direct costs of treating RTC patients accounted for 54% of the total RTC cost. Imaging in the current study was approximately four times higher, and laboratory tests almost five times greater than the Mpumalanga study. The higher cost variables of imaging and laboratory tests in our study are most likely because of the specialised nature of the facility with more expensive and/or more frequently used imaging and laboratory tests performed.
Gross-costing components (i.e., the compensation of employees, goods and services and pharmacy costs) equated to 86% of the total RTC cost in contrast to a cost analysis of RTCs in Mpumalanga over the 2015/16 financial year, which found that 46% of the cost of their study conducted at a tertiary hospital to be indirect costs.11 Similarities are noted between these studies pertaining to the major cost drivers. The compensation of employees in the 2018 study was 61%, with a similar calculation of 67% in the current study. Similarly, goods and services were calculated at 31% in the Mpumalanga study compared to 28% in this study. Despite pharmacy costs approximating 5% in the indirect cost section of the Mpumalanga study as well as the current study and appearing comparable, the study in Mpumalanga also calculated medication as a direct cost (29%), thus deeming pharmaceuticals as a significantly higher cost compared to this study, which only included pharmacy costs under the indirect cost component.
The average cost for treating RTC patients within the TICU IALCH unit was R12 727.56 (US$848.50) per inpatient day. The costs were approximately five times higher than the findings in the Mpumalanga study (R2 563; US$189.85), based on an exchange rate of R15 to US$1, and approximately twice as high as the Edendale study (approximately US$394).8,15 The possible explanations for these discrepancies are probably due to the type of facility the study was conducted at, i.e., regional versus central hospital, the severity of RTC patients treated (all comers versus an ICU cohort) as well as the peak RTC season noted in the Edendale study. Furthermore, the LOS period in the Mpumalanga study was more than double the LOS period in the current study, most likely because this was a hospital study versus our single-unit ICU study, thereby directly affecting the cost per inpatient day.
The average cost per RTC admission within TICU IALCH for the 2017/18 financial year was R163 879.65 (US$10 925.31). This cost was approximately 19 times higher than that of a study conducted at a hospital in Iran in 2016 (US$577.20), approximately 2.8 times higher than a local study in Mpumalanga in 2018 (R59 952.82, US$3 922.43) and roughly 1.6 times higher than the average cost per patient at a regional hospital in Pietermaritzburg in 2013 (US$ 6 988).4,10,11 However, the Cost of Crashes Report in 2016 found similar findings to our study, with the cost of medical treatment to be R110 656 and R147 143 for major and fatal RTCs, respectively.2
The possible reasons for the vast difference in the Iranian study were that the sample size was approximately nine times higher than that at our study facility. This would have directly impacted as this had an inversely proportional relationship to the cost per admission. The Cost of Crashes Report 2016 supported our study findings as well as noted the cost of medical treatment as a fraction of the total 'human casualty' cost including sub-components of lost productivity, pain, grief and suffering, funeral costs and workplace re-occupation. These medical costs amounted to an even smaller fraction of the total cost of RTCs noted, including human casualty, vehicle repair and incident costs.2
Moreover, the current study site is a central hospital with specialised care based on referrals, inferring that the patients ranged from moderate to severe and fatal injuries. The above results reflect costs related to different types of facilities with all severity levels of RTC patients, confirmed by the Pietermaritzburg study, which had 61% of patients with single area injuries compared to 13% of patients in the current study.4 The Mpumalanga study also suggested that the caseload was reduced due to no regulations enforced to commit the institution to collect data and record information related to RTCs leading to a low patient day equivalent which apportioned a lower human resource cost to their study.11
Study limitations
IALCH is a quaternary hospital. This facility has modern medical technology, a specialised staff complement and is based mainly on referrals from other facilities. This suggests that the patients to whom they render their services are those of a more complicated nature compared to patients treated at local district and regional hospitals. The patients at this facility, therefore, cannot be viewed as the 'average' RTC patient noted within KZN. The inherent nature of the facility and type of patients selected as the study population predispose the study to selection bias, with the majority of RTC patients being moderately to severely or fatally injured. Minor injuries would have been rare as this is a specialist trauma unit which is based predominantly on referrals. The costs noted with treating RTC patients at this facility are an under-estimation, since the direct non-medical and indirect costs were not included in this study. Rehabilitation costs were also not included under direct medical costs.
Conclusion
RTCs may, on the surface, appear to only affect the individual; however, they have a significant impact on the healthcare system and society at large. These costs highlight the importance of reducing the number of RTC injuries and fatalities by implementing prevention strategies. Greater emphasis should be placed on reducing the burden of RTCs by enhancing road user behaviours. Interventions should include primary prevention measures, such as road safety education, road traffic management measures and enhancing legislation and enforcement. Secondary prevention measures like improving post-crash care and tertiary prevention measures such as early rehabilitation are necessary to prevent complications and facilitate a better prognosis.
Acknowledgements
The authors wish to acknowledge the assistance provided by the Finance Department, Billing Department and the Business Intelligence Unit at IALCH.
Conflict of interest
The authors declare no conflict of interest.
Funding source
This research was self-funded.
Ethical approval
Ethical clearance was obtained from the Biomedical Research Ethics Committee of the University of KwaZulu-Natal, reference: BE310/18 and the Department of Health.
ORCID
RC Pillay https://orcid.org/0000-0002-2277-6470
Y Kista https://orcid.org/0000-0002-2140-3904
TC Hardcastle https://orcid.org/0000-0002-3967-0234
O Mahomed https://orcid.org/0000-0001-8076-0453
REFERENCES
1. World Health Organisation. Global status report on road safety. Geneva; 2015. [ Links ]
2. Labuschagne F. Cost of crashes in South Africa: Research and developement report 2016. South Africa: Road Traffic Management Corporation. [ Links ]
3. Wesson HK, Boikhutso N, Bachani AM, Hofman KJ, Hyder AA. The cost of injury and trauma care in low-and middle-income countries: a review of economic evidence. Health Policy Plan. 2014;29:795-808. [ Links ]
4. Parkinson F, Kent S, Aldous C, et al. The hospital cost of road traffic accidents at a South African regional trauma centre: a micro-costing study. Injury. 2014;45:342-5. [ Links ]
5. Marquez PV, Farrington JL. The Challenge of non-communicable disease and road traffic injuries in Sub-Saharan Africa: an overview. Washington, DC: The World Bank; 2013. [ Links ]
6. Arrive Alive. Decade of action for road safety in SA : Midterm report. 2017. Available from: https://www.arrivealive.co.za/United-Nations-Decade-of-Action-for-Road-Safety-2011-2020 . [ Links ]
7. Razzouk D. Methods for measuring and estimating costs. Mental Health Economics. Springer; 2017. p. 19-33. [ Links ]
8. Hrifach A, Brault C, Couray-Targe S, et al. Mixed method versus full top-down microcosting for organ recovery cost assessment in a French hospital group. Health Econ Rev. 2016;6:53. [ Links ]
9. Hendriks ME, Kundu P, Boers AC, et al. Step-by-step guideline for disease-specific costing studies in low-and middle-income countries: a mixed methodology. Glob Health Action. 2014;7:23573. [ Links ]
10. Sargazi A, Sargazi A, Jim PKN, et al. Economic burden of road traffic accidents; report from a single center from south Eastern Iran. Bull Emerg Trauma. 2016;4:43. [ Links ]
11. Matiwane BP, Mahomed O. Cost analysis of road traffic crashes in a tertiary hospital in Mpumalanga Province, South Africa. Cogent Medicine. 2018;5:1-13. [ Links ]
 Correspondence:
Correspondence:
O Mahomed
Email: mahomedo@ukzn.ac.za


{kind=link}