










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.58 no.4 Cape Town Dez. 2020
http://dx.doi.org/10.17159/2078-5151/2020/v58n4a3256
UROLOGY
Beware the bolus size: understanding intrarenal pressure during ureteroscopic fluid administration
J Lazarus PI; WisniewskiII; L KaestnerI
IDivision of Urology, Groote Schuur Hospital, University of Cape Town, South Africa
IIParklands Hospital, South Africa
ABSTRACT
BACKGROUND: Flexible ureteroscopy (FURS) and laser lithotripsy for ureteric and renal calculi requires adequate irrigation for visualisation. This study aimed to evaluate how bolus administration of irrigant fluid impacts intrarenal pressure (IRP) during FURS. We also investigated how ureteral access sheaths (UAS) of varying sizes mitigate elevated IRP
METHODS: Using a porcine cadaveric model, IRP was evaluated using an arterial invasive pressure measurement system. Given a fluid column height (driving force) of 80 cm H2O, and varying bolus administration (1, 2, 3, 5, 10 ml), IRP was studied with and without a UAS. An IRP of < 40 mmHg was considered the cut off for "safe" FURS. The flow (drainage capacity) of UAS was also evaluated. At varying fluid column heights, three sizes of UAS were used, 10/12 French size (Fr), 11/13 Fr and 12/14 Fr, all 36 cm long
RESULTS: Bolus administration with a UAS of < 5 ml with a starting fluid column height of 80 cm H2O was "safe" (< 40 mmHg). In contrast, where no UAS was used, bolus sizes as small as 2 ml produced "unsafe" peak pressures. The flow through a 10/12 Fr UAS was poor but improved greatly with larger UAS diameters
CONCLUSION: This study suggests that 10/12 Fr UAS may be inadequate to maintain drainage from the kidney at acceptable pressures. Bolus fluid administration produces "unsafe" (> 40 mmHg) elevated IRP in the absence of a UAS. When a UAS is used, a fluid bolus of < 5 ml is likely "safe"
Keywords: renal stones, ureteroscopy, complications, basic science, access sheaths, intrarenal pressure
Introduction
Nephrolithiasis (kidney stones) is one of the most common diseases in modern times, affecting one in ten people in the United States in their lifetime. Recurrence rates are high, and prevalence worldwide is increasing due to diet and lifestyle changes.1
Flexible ureteroscopy (FURS) and laser lithotripsy is a commonly performed urological procedure for ureteric and renal calculi. The interest in collateral damage during such endourological interventions is increasing. One aspect that has recently received more attention is the risk of complications associated with elevated intrarenal pressure (IRP).
Visibility is key to successful FURS. Given the small size of flexible ureterorenoscopes (typically in the range of 8-10 Fr diameter), obtaining adequate irrigation fluid flow is not always easy, especially when vision is hampered by bleeding, pus and debris in the collecting system. In order to improve visualisation, irrigant flow must be increased. Various devices such as syringes or foot pedals have been proposed to improve irrigant flow. These devices, while increasing flow, may contribute to elevated IRP.
Normal IRP is 0-15 mmHg.2 Hinman and Redewill showed that reflux of urine via pyelovenous reflux occurs above IRP of 40 mmHg.3 Elevated IRP has been linked to postoperative infectious complications.2
Ureteral access sheaths (UAS) are commonly employed during FURS. UAS and low flow rate irrigation has been demonstrated by Wilson and Preminger to reduce IRP.4
The aim of the study was to evaluate IRP during varying irrigant flow from typical clinical driving pressures of fluid, to investigate the impact of varying bolus size administration on IRP and in a parallel set of experiments to investigate the ability of a UAS to mitigate IRP and provide effective drainage.
Methods
IRP measurements were taken in response to varying fluid irrigation heights and bolus volumes. Fresh porcine cadaveric kidneys were used. The animals were not sacrificed for the purpose of the study. The porcine kidneys with preserved ureter were less than six hours post-mortem. Three porcine kidneys were used. For each experiment, the average IRP from the two kidneys was calculated.
IRP measurements were taken directly by means of 20-gauge cannula inserted to the renal pelvis (Figure 1) and transduced using a Deltran Invasive Blood Pressure Transducer (Utah Medical Incorporation, USA). To measure the IRP, an arterial invasive pressure measurement system, GE Datex - Ohmeda Cardiocap 5 was used and was zeroed to atmospheric pressure.

Water for irrigation boluses of 1, 2, 3, 5 and 10 ml were administered into the cadaveric ureter through a FURS (Pusen Uscope digital ureteroscope, Zhuhai Pusen Medical Technology Co., Ltd.) with a diameter of 3.1 mm (as measured by Mitutoyo Dial Callipers # 505-681, Mitutoyo, Japan) and a tip to Luer Lock length of 72 cm.
An irrigation set (standard Cysto-irrigation set - total length 220 cm) was attached to the irrigation port at a fluid column height of 0 and 80 cm. This was done with and without a UAS. The UAS was 36 cm long with a diameter of 12/14 Fr (inner diameter 12 Fr, outer diameter 14 Fr, Proxis, BARD/BD). The tip of the UAS was placed in the pelvis of the kidney.
The artificial choice of a column height 0 cm was motivated by wanting to assess the effect of fluid bolus administration in isolation, while a fluid column of 80 cm of H20 was used as 60-80 cm H20 is considered as the conventional height in clinical practice.
In the first experiment, starting pressure was measured before the bolus administration and the highest (peak pressure) following the bolus administration was recorded. The bolus was administered with a syringe by hand using a chronometer at a rate of 1 ml per second.
Gravitational hydrostatic pressure was recorded at a fluid column height of 0 cm and 80 cm of H2O (58 mmHg) with and without a UAS and with increasing volumes of bolus fluid administered (1, 2, 3, 5, 10 ml) (Figure 2).

Based on the work of Hinman and Redewill,3 an IRP of > 40 mmHg was considered the cut off for pyelovenous reflux and potentially "unsafe".
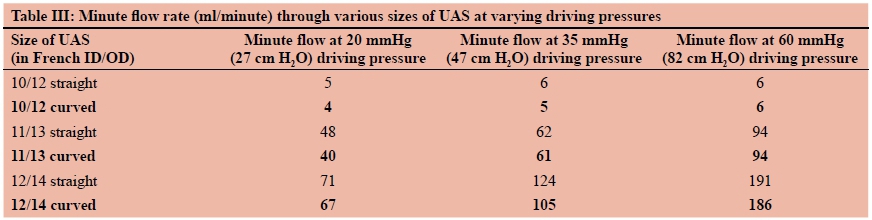
In the second experiment, assessment was made of drainage capacity of UAS at varying fluid column height (driving pressure) while the UAS was in a straight position and bent/curved. Three sizes of UAS were used 10/12 Fr, 11/13 Fr and 12/14 Fr, all 36 cm long. Partial obstruction
was caused by the 3.1 mm diameter Pusen FURS (Figure 3). The minute flow was measured, and the hourly flow was calculated.

Lastly, the second experiment was repeated, but this time measurements were taken through straight UAS and then through curved UAS (Figure 4).

Results
At a driving force of 0 cm H2O, only a bolus greater than 3 ml produced pressures above the predetermined "safe range" of < 40 mmHg. By comparison with the more typical clinical scenario, with a driving pressure of 80 cm H2O, any bolus of > 1 ml produced "unsafe" pressures (Table I).

In comparison, when a UAS was used, at a driving pressure of 0 cm H2O only a bolus of 10 ml resulted in pressures above 40 mmHg. However, if the driving pressure was 80 cm H2O, a bolus of 5 ml and above caused "unsafe" pressures (Table II).

In terms of drainage flow rate through various sizes of UAS at varying driving pressures, we found no appreciable difference between curved and straight UAS (Table III).
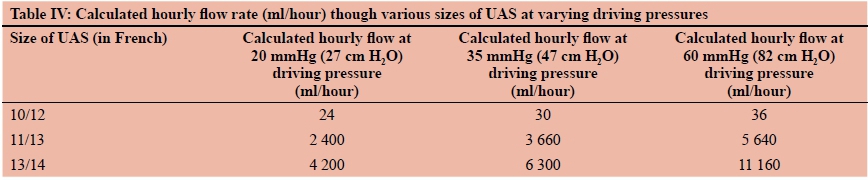
Flow through the 10/12 UAS was very poor (24 ml/hour) compared to 12/14 UAS (4 200 ml/hour) (Table IV).
Discussion
The normal IRP is in the range of 0-15 mmHg (0-20 cm H2O).5 Pyelovenous reflux has historically been quoted to occur above 40 mmHg (54 cm H2O),3 while more recent studies suggest it can occur at lower level of 20 mmHg (27 cm H2O).6 FURS is known to increase IRP to 60-100 mmHg in the absence of a UAS. If irrigation is forced, pressure rises above 300 mmHg are not unusual.2 In a recent study, Jung and Osther demonstrated in vivo that during routine FURS in 12 patients for stones, the IRP averaged 54 mmHg and pelvic pressure peaks up to 328 mmHg occurred. In a 5-minute standardised period of simple FURS, 83 pressure peaks > 50 mmHg were measured.7
These elevated IRPs have been linked most importantly to infection, but also to haemorrhage, renal impairment and postoperative pain.2 Pyelotubular reflux occurs at 20-30 mmHg and pyelovenous reflux occurs at 30-50 mmHg.23
Zhong et al. studied these infective complications demonstrating in a series of 260 patients undergoing FURS that a systemic inflammatory response (SIRS) was seen in 8.1%. Independent risk factors included: stone size, small-calibre UAS, irrigation flow rate and struvite calculi.8 The large multicentre Endourology Society (CROES) FURS study reported infection postoperatively in 2.97% with severe sepsis seen in 0.3%.9
The use of UAS has been shown by Traxer et al. to decrease postoperative sepsis rates by 50%.10 Other than UAS, the factors confirmed to impact IRP include: the access sheath size, the ureteroscope diameter and the irrigation rate.2
Strategies which reduce IRP and promote drainage should impact the incidence of infective complications and promote patient safety, particularly in those patients with infected struvite stones. Rehman et al. suggested that larger sized UAS lead to improved irrigation flow and lower IRPs in a human cadaveric model.11 Similarly, Wright et al. concluded statistically that a 12/14 Fr access sheath offered significantly improved irrigation whilst maintaining significantly lower IRP, when compared to a 10/12 Fr access sheath in a cadaveric porcine model.12
Another strategy proposed by Ng et al. noted substantially poorer flow with the irrigation channel occupied by a guidewire or basket. The proposed placing of the guidewire "inside or alongside the UAS provides by far the highest flow rates without a rise in IRP".13 Likewise, Wright et al. counterintuitively have shown that different laser fibres of apparently the same diameter reduce the flow to quite varying degrees.14
More recently, Fang et al. highlighted the importance of the ratio of endoscope-sheath diameter (RESD). They showed that to maintain a low intrapelvic pressure (IPP) and acceptable flow rate during FURS laser lithotripsy, RESD should be kept below 0.75. UAS length had less effect on the IPP and flow rate.15 This study goes on to note that certain manufacturers' ureteroscopes may be better suited to certain commercially available UAS in terms of IRP and flow characteristics. This work builds on an earlier paper by Monga et al.16
Our study presents three major findings. Firstly, we have demonstrated that UAS not only reduces IRP in the setting of continuous irrigation but also with bolus fluid administration. Bolus administration of< 5 ml with a starting fluid height (driving force) of 80 cm H2O is "safe". This contrasts with the situations where no UAS is used -here bolus volumes as little as 2 ml produced "unsafe" (> 40 mmHg) peak pressures. Secondly, flow through different sized UAS varies dramatically. The flow through a 10/12 Fr UAS is far poorer than through a larger UAS. This dramatic difference in flow in a larger UAS is a demonstration of Hagen-Poiseuille's law.17 The law shows that as tube radius halves, flow reduces by 16-fold (i.e. flow is proportional to radius of the tube to the power of 4). This finding would appear to contradict Sener et al. whose findings showed in vitro that FURS via a 10/12 Fr UAS provided pressures below 30 mmHg.18 Thirdly, despite good minute drainage capacity of the two larger UAS (Fr 11/13 and Fr 12/14), this ability of good flow is in sharp contrast to its limited ability to reduce IRP during bolus administration. The relationship between flow and IRP reduction requires further elucidation
Despite the increased flow of larger calibre UASs, it should be mentioned that their use is not without its own set of complications. Traxer and Thomas showed that marked ureteral wall injury is common after the insertion of a 12/14 Fr UAS and that this risk benefit should be born in mind when using large UASs.19
Our study has limitations. The work was done in vitro in porcine cadaveric kidneys. This limits its applicability to live human subjects. The lack of peristalsis from a living animal and the pressure from the surrounding tissues may make the results less useful in a clinical setting. It would be useful to attempt to reproduce these findings in vivo. We limited the study to a single set of devices which limits it applicability to other manufactured products.
Conclusion
Visibility is key to successful FURS. Infective and other complications are under-recognised problems with FURS. Keeping IRP low while promoting flow appears to be critical in reducing these complications. This study suggests that 10/12 UAS may be inadequate to maintain drainage from the kidney. Bolus fluid administration produces "unsafe" (> 40 mmHg) elevated IRP in the absence of a UAS. When a UAS is used, fluid bolus < 5 ml is likely "safe". Further work is warranted to investigate how elevated IRP can better be mitigated.
Conflict of interest
The authors declare no conflict of interest.
Funding source None.
Ethical approval
The research did not involve human participants and/or animals and therefore did not require ethical approval.
ORCID
J Lazarus https://orcid.org/0000-0003-2417-8332
L Kaestner https://orcid.org/0000-0001 -7417-735X
REFERENCES
1. Turner BW, Reynard JM, Noble JG, et al. Trends in urological stone disease. BJU Int. 2012;109:1082-7 [ Links ]
2. Osther PJS. Risks of flexible ureterorenoscopy: pathophysiology and prevention. Urolithiasis. 2018;46:59-67. [ Links ]
3. Hinman F, Redewill FH. Pyelovenous back flow. J Am Med Assoc. 1926:87(16):1287-93. [ Links ]
4. Wilson WT, Preminger GM. Intrarenal pressures generated during flexible deflectable ureterorenoscopy. J Endourol. 1990;4(2):135-41. [ Links ]
5. Oratis AT, Subasic JJ, Hernandez N, et al. A simple fluid dynamic model of renal pelvis pressures during ureteroscopic kidney stone treatment. PLoS ONE. 2018;13(11):e020820. [ Links ]
6. Tokas T, Herrmann TR, Skolarikos A, et al. Pressure matters: intrarenal pressures during normal and pathological conditions, and impact of increased values to renal physiology. World J Urol. 2019;37(1):125-31. https://doi.org/10.1007/s00345-018-2378. [ Links ]
7. Jung H, Osther PJS. Intraluminal pressure profiles during flexible ureterorenoscopy. SpringerPlus. 2015;4:373. [ Links ]
8. Zhong W, Leto G, Wang L, Zeng G. Systemic inflammatory response syndrome after flexible ureteroscopic lithotripsy: a study of risk factors. J Endourol. 2015;29(1):25-8. [ Links ]
9. Somani BK, Giusti, Sun Y, et al. Complications associated with ureterorenoscopy (URS) related to treatment of urolithiasis: The Clinical Research Office of Endourological Society URS Global study. World J Urol. 2017;35:675-81. [ Links ]
10. Traxer O, Wendt-Nordahl G, Sodha H, et al. Differences in renal stone treatment and outcomes for patients treated either with or without the support of a ureteral access sheath: The Clinical Research Office of the Endourological Society Ureteroscopy Global Study. World J Urol. 2015;33(12):2137-44 [ Links ]
11. Rehman J, Monga M, Landman J, et al. Characterization of intrapelvic pressure during ureteropyeloscopy with ureteral access sheaths. Urology. 2003;61:713-8. [ Links ]
12. Wright A, Williams K, Somani B, Rukin N. Intrarenal pressure and irrigation flow with commonly used ureteric access sheaths and instruments. Cent European J Urol. 2015;68(4):434-8. [ Links ]
13. Ng YH, Somani BK, Dennison A, et al. Irrigant flow and intrarenal pressure during flexible ureteroscopy: the effect of different access sheaths, working channel instruments, and hydrostatic pressure. J Endourol. 2010;24(12):1915-20. [ Links ]
14. Wright AE, Williams K, Rukin NJ. What effect do different 200 μπι laser fibres have on deflection and irrigation flow rates in a flexible ureterorenoscope? Lasers Med Sci. 2015;30(5):1565-8. [ Links ]
15. Fang L, Xie G, Zheng Z, et al. The effect of ratio of endoscope-sheath diameter on intrapelvic pressure during flexible ureteroscopic lasertripsy. J Endourol. 2019;33:132-9. [ Links ]
16. Monga M, Bodie J, Ercole B. Is there a role for small-diameter ureteral access sheaths? Impact on irrigant flow and intrapelvic pressures. Urology. 2004;64(3):439-41; discussion 441-2. [ Links ]
17. Open Anesthesia [Internet]. Poiseuille's law: IV fluids. c2020. Available from: https://www.openanesthesia.org/poiseuilles_law_iv_fluids/. Accessed 10 January 2019. [ Links ]
18. Sener E, Cloutier J, Villa L, et al. Can we provide low intrarenal pressures with good irrigation flow by decreasing the size of ureteral access sheaths? J Endourol. 2016;30(1):49-55. [ Links ]
19. Traxer O, Thomas A. Prospective evaluation and classification of ureteral wall injuries resulting from insertion of a ureteral access sheath during retrograde intrarenal surgery. J Urol. 2013;189:580-4. [ Links ]
 Correspondence:
Correspondence:
email: j.lazarus@uct.ac.za


{kind=link}
{kind=link}