










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.58 no.4 Cape Town Dez. 2020
http://dx.doi.org/10.17159/2078-5151/2020/v58n4a3128
ORIGINAL ARTICLE
Alarm features as predictors of major findings in a rural South African upper endoscopic service
S CheddieI; CG MannehI; Y MoodleyII
IClinical Surgery Unit, Madadeni Hospital, University of KwaZulu-Natal, South Africa
IIFaculty of Health and Environmental Sciences, Central University of Technology, South Africa
ABSTRACT
BACKGROUND: Alarm features are commonly used to identify patients who require an endoscopy to rule out significant upper-gastrointestinal (GI) pathology. Validation of these features in a rural South African (SA) setting has implications for the provision of endoscopy services and was the aim of this study.
METHODS: This was a retrospective chart review of 1 000 consecutive endoscopies performed at a rural SA regional/ referral hospital over three years. Demographic data, indication for endoscopy (upper GI bleed, dyspepsia, dysphagia, anaemia, weight loss, age) and major endoscopic findings (defined any tumour, ulcer, or stricture) were recorded. A multivariate logistic regression analysis was done to identify risk factors for major endoscopic findings.
RESULTS: The median age of the study sample was 51.0 (range14.0-88.0) years. Males (306/1 000) accounted for 30.6% of the study population. The prevalence of alarm features in the study sample was as follows: upper GI bleed - 16.6%; dyspepsia - 58.4%; dysphagia - 10.3%; anaemia - 3.5%; weight loss - 0.3%. The following alarm features were statistically significant in detecting a major endoscopic finding: age > 60 (OR: 2.67, CI: 1.82-3.96), male gender (OR: 1.52, CI: 1.03-2.24), dysphagia (OR: 12.16, CI: 4.33-34.19) and upper GI bleed (OR: 2.77, CI: 1.03-7.47), p < 0.05.
CONCLUSION: Dysphagia, age > 60, male gender, and upper GI bleed are identifiable risk factors for major endoscopic findings. Not all the alarm features for major endoscopic findings that are established elsewhere can be applied in our rural SA setting.
Keywords: endoscopy, oesophageal cancer, gastric cancer, alarm features, South Africa
Introduction
South Africa (SA) is currently experiencing an epidemiolog-ical transition, whereby the burden of non-communicable diseases will soon exceed the traditionally higher burden of communicable disease in the country. This epidemiological profile is very different from that in countries such as the United States or the United Kingdom, which have long since completed their epidemiological transition. The incidence of non-communicable upper-gastrointestinal (GI) disorders has grown substantially amongst the rural SA populace, possibly a reflection of urbanisation, adoption of westernised lifestyles and an increase in risk factors in this group. Diagnosis of upper GI disorders through clinical examination alone is challenging, with foregut cancer being a possible diagnosis. Understandably, physicians and general surgeons decide to err on the side of caution and refer a large proportion of patients with upper GI symptoms for endoscopy, even when the probability of cancer is very low. The high proportion of patients with upper GI clinical symptoms unnecessarily referred for endoscopy can have a significant impact on the delivery of endoscopy services, particularly in rural SA hospitals where there is a shortage of appropriate skills and equipment.1 In other countries, several "alarm features" have been proposed in order to reduce unnecessary endoscopy and improve the triage of patients through endoscopy units.210 These features include patient demographics, clinical symptoms, and comorbidity. While the predictive value of these alarm features differs between settings, in most instances they demonstrate the ability to improve clinical decision-making related to endoscopy services. Validation of these features in a rural SA hospital service has not yet been performed. This would have important implications related to resource utilisation for endoscopy services in this setting. Therefore, the objective of this study was to confirm alarm features for major upper GI endoscopic findings, which have been established elsewhere, in a rural SA setting.
Methods
The study was conducted at the public-sector Madadeni Provincial Hospital. This 800-bed regional/referral hospital is located in rural northern KwaZulu-Natal Province, SA. The population served by the hospital is predominantly of black African ethnicity. The hospital has an endoscopy unit service by two general surgeons, with an estimated weekly procedure rate of ten endoscopies.
A retrospective chart review of 1 000 consecutive pa-tients (hereafter referred to as "the study sample") who had upper GI endoscopies at the hospital's endoscopy unit between 1 January 2014 and 31 December 2016 was performed. Patients in this study were aged > 13 years old and were identified from the hospital endoscopy lists. Data was collected from each patient's medical chart using an electronic spreadsheet. Data collected for alarm features included patient demographics (age and gender) and indication for endoscopy (dyspepsia, upper GI bleeding, reflux, anaemia, weight loss, dysphagia, and corrosive ingestion). Post-endoscopic findings (gastritis, normal, candidiasis, oesophagitis, stricture, gastric tumour, oesophageal tumour, hiatus hernia, peptic ulcer disease, oesophageal varices) were extracted from the procedural notes in the patient's medical chart and the post-procedural findings book maintained in the endoscopy unit. The study outcome was major endoscopic findings. This composite outcome was defined as the presence of any one of the following conditions during an endoscopy: stricture, ulcer or histologically confirmed malignancy.2
The electronic spreadsheet was analysed with the Statistical Package for the Social Sciences (SPSS) version 25.0 (IBM Corporation, New York). Descriptive statistics were used to present the characteristics of the study sample, with results presented as frequencies and percentages or means with standard deviation. The χ2 test was used to investigate potential statistical associations between various alarm features and the study outcome, with results presented as frequencies and percentages along with a p-value. Alarm features withp < 0.200 in the χ2 analysis were selected for inclusion in the multivariate logistic regression analysis as independent variables, with major endoscopic findings being entered into the analysis as the dependent variable. This process of purposeful selection of variables for inclusion in a regression analysis ensures that a parsimonious regression model is obtained. Results of the multivariate logistic regression analysis are presented as odds ratios (OR) with 95% confidence intervals (CI) and a p-value. A value < 0.05 in the multivariate logistic regression analysis was considered a statistically significant result. The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated for alarm features which had a significant result in the logistic regression analysis.
Results
A description of the study sample is provided in Table I. One hundred and ninety-four (194) patients (19.4%) in the study sample had major endoscopic findings.

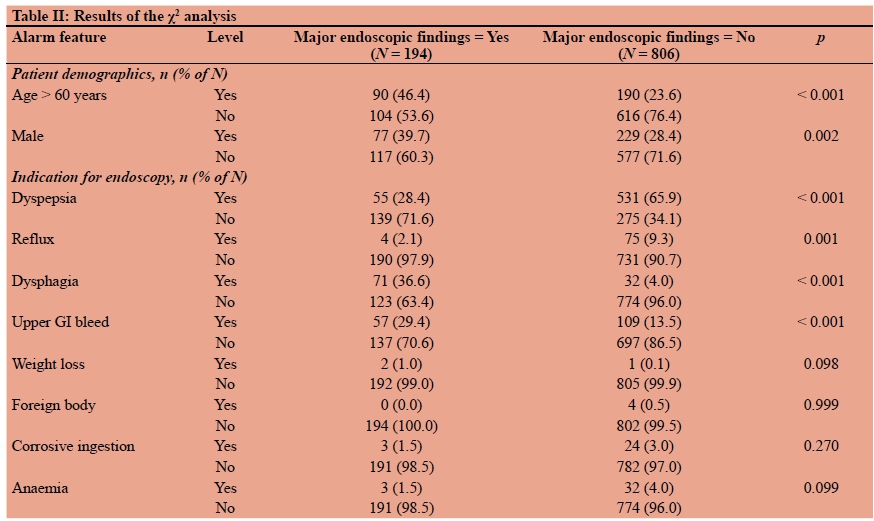
The results of the χ2 analysis are shown in Table II. Only corrosive ingestion and the presence of a foreign body did not meet the criteria of p < 0.200 in the χ2 analysis for subsequent inclusion in the multivariate logistic regression analysis.
Statistically significant results were observed for four of the eight alarm features entered into each multivariate logistic regression analysis (Table III). The following alarm features, age > 60 years, male gender, dysphagia, and upper GI bleed, were associated with a major endoscopic finding. The ORs for all significant variables were > 1.00, suggesting that all significant alarm features identified through this model were associated with an increased risk of major endoscopic findings.
Discussion
This study has shown that age > 60 years and certain alarm features, namely dysphagia, male gender and upper GI bleed are predictors of major endoscopic findings in rural South African patients. Some alarm features like anaemia and unintentional weight loss were not identified as predictors of major endoscopic findings. These findings are important because it demonstrates that the relative importance of alarm features can differ between South Africa and other settings.
The South African guidelines have stipulated that the age > 45 years cut-off be used to screen patients with dyspepsia.3 Recent American College of Gastroenterology (ACG) guidelines have increased the age threshold for screening dyspepsia patients to > 60 years.4 A recent study by the author has shown that an age cut-off > 60 years has a high NPV (93%) for screening endoscopy for patients with dyspepsia in the South African context. There was no significant difference in detecting major endoscopic findings between age cut-offs of > 45 years versus age > 60 years.5 The rationale for screening dyspepsia patients aged > 60 is based on the perceived risk of gastric malignancy being higher in this age group. Endoscopy can detect gastric malignancy at an early stage.6 In the age group < 60, the risk of gastric malignancy is < 1%. Wallace et al. have shown that age was a poor predictor of major endoscopic findings (ulcer, stricture and tumour), and recommended that better clinical protocols be established.2 In their study, major endoscopic findings increased in a linear fashion from age 45 to 65, however the sensitivity was 85% and the specificity was only 26%. In our study the age cut-off > 60 years had a high NPV of 85.6% which implies that the large majority of patients < 60 years will not have a major endoscopic finding. A recent study by Abdeljawad et al. has shown that dyspeptic patients have a low prevalence of major endoscopic findings and age > 55 is associated with higher risk of major endoscopic findings.7 The predictive value of alarm features in detecting major endoscopic findings is controversial. In our study, patients with dysphagia had a 12-fold greater probability of having a significant underlying pathology and the highest PPV (68%) when compared with other alarm features. This is most likely explained by the observation that patients presenting with dysphagia had a high rate of oesophageal malignancy (56%) with an overall malignancy rate of 8.6% in our study population. A large North American study by Wallace et al. had shown that dysphagia was not a predictor of major endoscopic findings.2 Other studies from countries like Iran where there is a high prevalence of oesophageal cancer has shown dysphagia to be a strong predictor in detecting upper GI malignancy with similar odds ratios to our study.8 Lee et al. have shown that alarm features are poor predictors of upper GI malignancy in an Asian population with a low malignancy rate of 2.1%. In their study, dysphagia was found to have a PPV of 67% and a NPV of 98%. The high NPV and high specificity correlates with the low percentage of malignancy in their study population.9
A meta-analysis by Chen et al. had shown that alarm features were moderate predictors of upper GI malignancy in uninvestigated dyspepsia patients (AUC 0.74). The overall malignancy rate was low (1.3%).10 Wallace et al. had concluded that both age and alarm features did not predict significant pathological findings at endoscopy, however, the absence of alarm features had a high NPV in excluding upper GI malignancy.2 Our study has shown similar results with high NPVs shown for the alarm features investigated. Kapoor et al. evaluated the diagnostic accuracy of alarm features in a clinical prediction model for cancer and showed that dysphagia (OR = 6.87) and weight loss (OR = 12.2) were significant predictive factors for cancer, but the diagnostic value of other alarm features was limited.11 The use of individual alarm features is less likely to have an excellent predictive accuracy than using a combination of alarm features. Our study has shown a high diagnostic yield for upper GI malignancy of 8.6% thus necessitating a low threshold to perform an upper GI endoscopy to exclude malignancy despite the low PPVs seen in the alarm features investigated.
Our study has shown that male gender was a risk factor for detecting major endoscopic findings. Other studies have shown that male gender is a validated risk factor.89 Male gender is an established risk factor for gastric cancer, oesophageal cancer and in peptic ulcer disease, and would thus increase the likelihood of detecting significant pathology at endoscopy in this high-risk group. Overall, the majority of patients who underwent endoscopy were female with the commonest indication being dyspepsia. A large meta-analysis by Ford et al. showed a higher pooled prevalence of dyspepsia in women compared with men (25.3 vs 21.9%), which still remains much lower than the prevalence seen in our study.12 Gender-based prevalence studies have shown that the prevalence of dyspepsia in men and women is inconsistent.13 We postulate that women are more likely to seek healthcare for dyspepsia symptoms than men - resulting in a higher number of endoscopies being performed.14
There are several limitations to this study. As it is retrospective in design, we had to rely on patients' records from an endoscopy report book, which is subject to clinician and observer error. Patients whose records were analysed may not be representative of the general population, as this was a regional, hospital-based study in a rural area. Data regarding medical comorbidities, H. pylori infection, duration of symptoms and HIV status were not collected.
Conclusion
Alarm features, namely dysphagia, age > 60 years, upper GI bleed and male gender are important risk factors for detecting major endoscopic findings in rural patients in the South African setting. The high prevalence of malignancy in this study, especially oesophageal cancer, necessitates a low threshold to perform a diagnostic upper GI endoscopy in the presence of identifiable alarm features, despite the low PPVs. The association between alarm features and their predictive accuracy for major endoscopic findings differs between countries. As such, caution should be exercised in our South African setting when applying alarm features for disease prediction which have been identified in other countries. Further prospective studies are required in South Africa to evaluate the predictive value of a combination of alarm features in predicting major endoscopic findings.
Conflict of interest
The authors declare no conflict of interest.
Funding source
None.
Ethical approval
Ethical approval to conduct the study was granted by the Biomedical Research Ethics Committee of the University of KwaZulu-Natal (Protocol reference 620/17).
ORCID
S Cheddie © https://orcid.org/0000-0002-1844-5759
CG Mannen © https://orcid.org/0000-0001-9761-0603
Y Moodley © https://orcid.org/0000-0002-4119-1734
REFERENCES
1. Loots E, Clarke DL, Newton K, et al. Endoscopy services in KwaZulu-Natal Province, South Africa, are insufficient for the burden of disease: is patient care compromised? S Afr Med J. 2017;107(11):1022-5. https://doi.org/10.7196/SAMJ.2017.v107i11.1248. [ Links ]
2. Wallace MB, Durkalski VL, Vaughan J, et al. Age and alarm symptoms do not predict endoscopic findings among patients with dyspepsia: A multicentre database study. Gut. 2001;49:29-34. https://doi.org/10.1136/gut.49.L29. [ Links ]
3. Louw JA, Pinkney-Atkinson V. Diagnosis and management of dyspepsia - clinical guideline, 1999. Dyspepsia Working Group, South African Medical Association, South African Gastroenterology Society Working Group. SAMJ. 1999 Aug;89(8 Pt 2):897-903. [ Links ]
4. Moayyedi PM, Lacy BE, Andrews CN, et al. ACG and CAG clinical guideline: management of dyspepsia. Am J Gastroenterol. 2017 Jul;112(7):988-1013. https://doi.org/10.1038/ajg.2017.154. [ Links ]
5. Cheddie S, Manneh CG, Owczarek BM, Moodley Y. Age is a predictor of significant endoscopic findings in dyspepsia patients in South Africa. S Afr J Surg. 2020;58(1):14-8. https://doi.org/10.17159/2078-5151/2020/v58n1a2814. [ Links ]
6. Spahos T, Hindermarsh A, Cameron E, et al. Endoscopy waiting times and impact of the two week wait scheme on diagnosis and outcome of upper gastrointestinal cancer. Postgrad Med J. 2005;81:728-30. https://doi.org/10.1136/pgmj.2004.031104. [ Links ]
7. Abdeljawad K, Wehbeh A, Quayed E. Low prevalence of clinically significant endoscopic findings in outpatients with dyspepsia. Gastroenterol Res Pract. 2017;35436817p. Epub 2017 Jan 22. https://doi.org/10.1155/2017/3543681. [ Links ]
8. Lee SW, Chang CS, Yeh HJ, et al. Diagnostic value of alarm features for identifying types and stages of upper gastrointestinal malignancies. Gastroenterol Res. 2017;10(2):120-5. https://doi.org/10.14740/gr826w. [ Links ]
9. Ataie-Korasgani M, Emami MH, Javari-Posve N. Diagnostic value of alarm symptoms for upper GI malignancy in patients referred to GI clinic: A 7-years cross-sectional study. J Res Med Sci. 2017;22:76 https://doi.org/10.4103/jrms.jrms_450_15. [ Links ]
10. Chen SL, Gwee KA, Lee JS, et al. Systematic review with meta-analysis: prompt endoscopy as the initial management strategy for uninvestigated dyspepsia in Asia. Aliment Pharmacol Ther. 2015;41:239-52. https://doi.org/10.1111/apt.13028. [ Links ]
11. Kapoor N, Bassi A, Sturgess R, Bodger K. Predictive value of alarm features in a rapid access upper gastrointestinal cancer service. Gut. 2005;54:40-5. https://doi.org/10.1016/s0016-5085(03)80901-0. [ Links ]
12. Ford AC, Marwaha A, Sood R, et al. Global prevalence of, and risk factors for, uninvestigated dyspepsia: a metaanalysis. Gut. 2015;64(7):1049-57. https://doi.org/10.1136/gutjnl-2014-307843. [ Links ]
13. Ahlawat SK, Cuddihy MT, Locke GR 3rd. Gender-related differences in dyspepsia: a qualitative systematic review. Gend Med. 2006/3(1):31-42. https://doi.org/10.1016/s1550-8579(06)80192-0. [ Links ]
14. Koloski NA, Talley NJ, Boyce PM. Epidemiology and health care seeking in the functional GI disorders: a population-based study. Am J Gastroenterol. 2002/97(9):2290-9. https://doi.org/10.1016/s0002-9270(02)04139-4. [ Links ]
 Correspondence:
Correspondence:
email: scheddie@gmail.com


{kind=link}
{kind=link}
{kind=link}