










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Surgery
versión On-line ISSN 2078-5151
versión impresa ISSN 0038-2361
S. Afr. j. surg. vol.57 no.4 Cape Town dic. 2019
http://dx.doi.org/10.17159/2078-5151/2019/v57n4a2916
CASE REPORTS
Tuberculous prostatitis: a condition not confined to the immunocompromised
JC HeiligI; Y ReddyII; M KeyterII; M du ToitIII; A AdamI
IDepartment of Urology, Helen Joseph Hospital, University of Witwatersrand, Johannesburg, South Africa
IIDepartment of Anatomical Pathology, Charlotte Maxeke Johannesburg Academic Hospital, University of Witwatersrand, Johannesburg, South Africa
IIIDepartment of Radiology, Helen Joseph Hospital, University of Witwatersrand, Johannesburg, South Africa
SUMMARY
Tuberculous (TB) prostatitis is rare; usually occurring in immunocompromised men. It can mimic benign prostatic hyperplasia (BPH), chronic prostatitis or prostate cancer. This report in an immunocompetent 72-year-old man adds to the clinical spectrum of the five prior reported cases. A low threshold for prostatic biopsy led to a histological evaluation and subsequent microbiological confirmation of TB. This attests to the value of such an approach in arriving at the correct diagnosis and the institution of appropriate anti-tuberculous therapy even amongst immune-competent men.
Case report
A 72-year-old man from rural South Africa presented with a one-year history of lower urinary tract symptoms (LUTS) and intermittent right scrotal pain. His International Prostate Symptom Score (IPSS) (a questionnaire-based screening tool to quantify, track and manage the symptoms of BPH/LUTS) was 19, indicating moderately severe symptoms.1 He denied any constitutional symptoms and there was no significant medical or surgical history. He had no known TB contacts nor any occupational risk factors to develop TB. He was not on corticosteroids.
The general and systemic examination was unremarkable. The patient had mild right hemi-scrotal swelling with no skin changes or sinuses and no clearly definable mass on urogenital examination, and digital rectal examination (DRE) findings revealed a hard, nodular prostate. His prostate specific antigen (PSA) was 37.99 ug/L and urinalysis showed a sterile pyuria. A clinical suspicion of underlying 'prostate cancer' was formulated in light of the DRE and PSA, so a trans-rectal ultrasound guided (TRUS) prostate biopsy was performed.
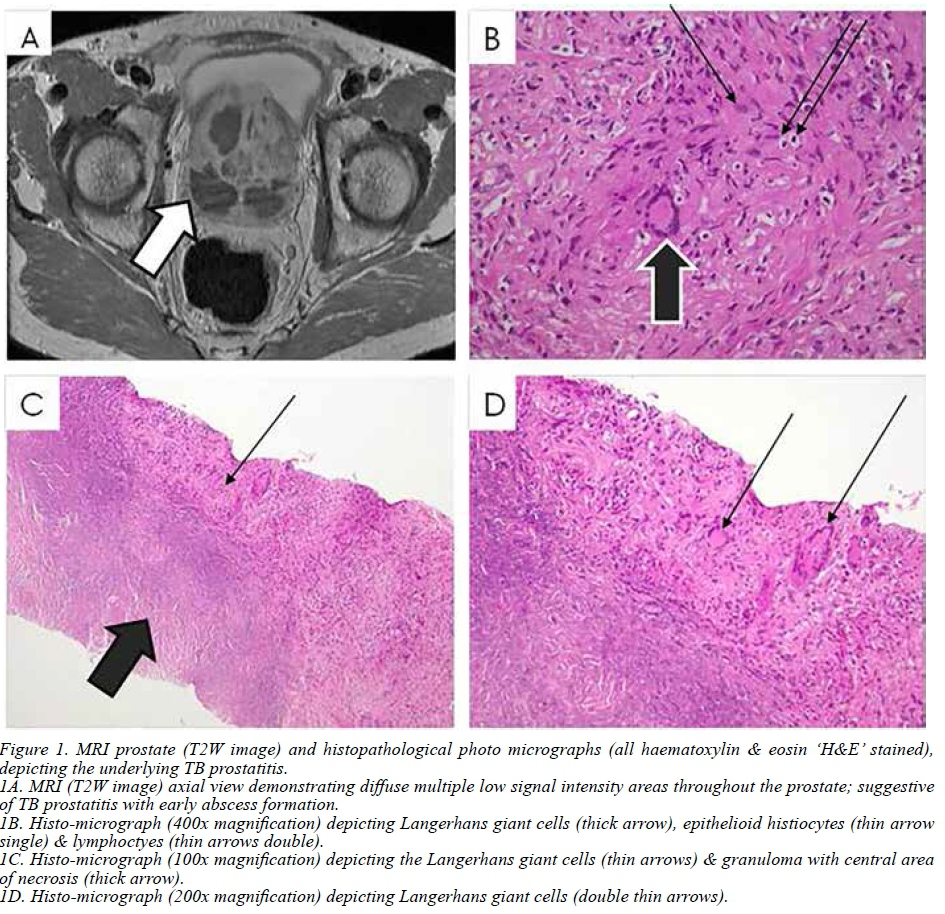
Histology showed extensive necrotising granulomatous inflammation suggestive of an active mycobacterial infection, although acid-fast bacilli (AFB) were not detected and PAS staining showed no fungal infection. (Figure 1 B-D). There were no pre-neoplastic or neoplastic features.
Despite the absence of AFB on the slides assessed, the associated features and regional residence led to a working diagnosis of TB prostatitis and the patient was investigated accordingly. An HIV ELISA test was non-reactive. His chest radiograph was unremarkable. A urine lipoarabinomannan (LAM) test was positive and his urine auramine-O was positive and cultured TB after 14 days. Urine gene expert was not done due to laboratory protocol. Serum ACE (angiotensin converting enzyme) and ANCA (anti-neutrophil cytoplasmic antibodies) were negative and therefore other granulomatous disease, such as sarcoidosis, was excluded from the differential diagnosis.
Further imaging of the upper tracts showed no abnormalities. Magnetic resonance imaging (MRI) of the prostate revealed a prostatic volume of 151 ml and infective changes of the prostate and seminal vesicles (PI-RADS 1 - 'most probably benign') (Figure 1 A). The acronym PI-RADS stands for Prostate Imaging-Reporting and Data System. It is a scoring system to risk stratify MRI findings of the prostate for suspected malignancy (1 - very low risk of cancer; 2 - low; 3 - intermediate; 4 - high; 5 - very high).2
In light of the above findings and after consultation with the local Infectious Diseases department, he was initiated on anti-tuberculous medication, and will complete nine months of treatment as per institutional protocol. As TB can coexist with prostate cancer symptomatic evaluation, clinical examination, DRE and PSA trend will determine the need for re-biopsy at follow up.
Discussion
Genitourinary tuberculosis (GUTB) accounts for about 30-40% of all extra-pulmonary TB cases.3 The organs usually affected are the kidneys, ureters, bladder and genital organs.4 Primary prostatic TB is rare, especially in immune-competent patients,3,4 with only five prior reports from high prevalence TB areas.5 Routes of transmission include descending infection from the upper urinary tract, haematogenous and lymphatic spread, direct extension from neighbouring structures, post intra-vesical injection of Bacille Calmette-Guerin (BCG) for bladder carcinoma and very rarely, from sexual transmission.3,5
The clinical presentation of TB prostatitis is often nonspecific and patients most commonly present with LUTS, a suspicious DRE and elevated PSA; therefore mimicking benign prostatic hyperplasia (BPH), chronic prostatitis and prostate cancer clinically, biochemically and radiologically.4,6
Furthermore, one needs to remain cognisant that TB prostatitis may co-exist with prostate cancer.7 Most cases of TB prostatitis are diagnosed incidentally on histology following prostate biopsy for suspected carcinoma, transurethral resection of the prostate (TURP) or prostatectomy.5 Prostatic specimens may be examined by histopathology, polymerase chain reaction (PCR) for mycobacterial detection, culture and stains for AFBs.7,8 The characteristic lesion is confluent foci of caseous necrosis surrounded by epithelioid histiocytes. However, as in our case, the absence of caseation on biopsy does not necessarily exclude TB prostatitis.6
We performed a urine LAM test on our patient, which was positive and suggestive of disseminated TB. Suwanpimolkul et al. suggested the possible use of the urine LAM test with
AFB smear and culture in resource limited countries for the diagnosis of TB in patients with advanced HIV and in HIV negative patients with disseminated TB.6,9
Imaging studies are useful in the diagnostic workup.4 TRUS may reveal enlargement and hypoechoic lesions and should be used for guided biopsy of suspicious lesions. Contrast CT usually demonstrates multiple bilateral low density prostatic lesions with irregular borders and can identify upper tract or abdominal signs of TB. MRI has some advantages over CT, including better resolution and multi-planar imaging options.5 Voiding cystourethrogram with retrograde urethrogram may reveal filling defects suggestive of TB cavities.8
Important benign mimickers of prostate cancer which give rise to false-positive malignant cells are prostatic atrophy, post-atrophic hyperplasia, atypical adenomatous hyperplasia and seminal vesicle tissue. Inflammatory processes such as granulomatous prostatitis, xanthogranulomatous prostatitis and malakoplakia may simulate high grade adenocarcinoma.10
The primary treatment of TB prostatitis is medical with anti-tuberculous medication. Surgery, such as endoscopic resection, may be considered when medical therapy is unsuccessful3 as determined by persistence or non-resolution of symptoms and complications such as prostatic abscesses.
Our patient was initiated on anti-TB medication according to the standard national policy and will be followed up regularly as an outpatient.
Conclusion
TB prostatitis is a rare clinical entity that is usually diagnosed incidentally. The urologist and his/her pathologist should maintain a high index of suspicion in patients who present with LUTS, a suspicious DRE and an elevated PSA. Biopsy is key to establishing the correct diagnosis and treatment.
Conflict of interest
The authors declare none.
Ethics clearance
Local institutional ethics clearance was attained with Human Research Ethics Committee (Medical) Certificate M.180892 (2018).
Funding
None.
Orcid
J Heilig http://orcid.org0000-0002-5560-9396
REFERENCES
1. Barry MJ, Fowler FJ, O'Leary MP. The American Urological Association Symptom Index for Benign Prostatic Hyperplasia. J Urol. 1992;148:1549-57. doi: 10.1016/s0022-5347(17)36966-5 [ Links ]
2. Padhani AR, Weinreb J, Rosenkrantz AB, Villeirs G, Turkbey B, Barentsz J. Prostate imaging-reporting and data system steering committee: PI-RADS v2 status update and future directions. Eur Urol. 2019;1;75(3):385-96. doi: 10.1016/j.eururo.2018.05.035 [ Links ]
3. Gupta S, Khumukcham S, Lodh B, Singh AK. Primary prostatic tuberculosis: A rare clinical entity. J Med Soc. 2013;:84-6. doi: 10.4103/0972-4958.116658 [ Links ]
4. Esa NY, Hanafiah M, Koshy M, Abdullah H, Izuanuddin I, Rani MFAR. A rare case of tuberculous prostatitis. JCHS. 2016;1(2):33-6. doi: 10.25141/2476-2504-2017-3.0030 [ Links ]
5. Rafique M, Rauf A, Rafique T, Bhutta RA. Tuberculosis of Prostate. JPMA. 2001;51:408-10. doi: 10.1016/j.idcr.2016.06.002 [ Links ]
6. Zhang H, Xu Y, Liu R. A rare case of prostatic tuberculosis accompanied by prostate cancer. BJU Int. 2010. doi: 10.1002/BJUIw-2010-038-web [ Links ]
7. Shukla P, Gulwani H, Kaur S. Granulomatous prostatitis: clinical and histomorphologic survey of the disease in a tertiary care hospital. Prostate Int. 2017;5:29-34. doi: 10.1016/j.prnil.2017.01.003 [ Links ]
8. Kulchavenya E, Brizhatyuk E, Khomyakov V. Diagnosis and therapy for prostate tuberculosis. Ther Adv Urol. 2014;6(4):129-34. doi: 10.1177/1756287214529005 [ Links ]
9. Suwanpimolkul G, Kawkitinarong K, Manosuthi W, et al. Utility of urine lipoarabinomannan (LAM) in diagnosing tuberculosis and predicting mortality with and without HIV. Prospective TB cohort from the Thailand Big City TB Research Network. Int J Infect Dis. 2017;59:96-102. doi: 10.1016/j.ijid.2017.04.017 [ Links ]
10. Srigley J. Benign mimickers of prostatic adenocarcinoma. Mod Pathol 2004;17:328-48. doi: 10.1038/modpathol.3800055 [ Links ]
 Correspondence:
Correspondence:
Dr Julian Hellig
julianhellig@icloud.com


{kind=link}