










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.57 n.3 Cape Town Sep. 2019
http://dx.doi.org/10.17159/2078-5151/2019/v57n3a2934
TRAUMA
Surgical site infection after penetrating abdominal trauma with bowel involvement: a comparison between HIV-seropositive and seronegative patients
M MauserI; Christos BartsokasII; Frank PlaniI
IChris Hani Baragwanath Academic Hospital, Johannesburg
IIHippokration General Hospital of Athens, Greece
ABSTRACT
BACKGROUND: The influence of HIV-infection on surgical site infection (SSI) after surgery for penetrating abdominal trauma is not investigated and therefore not as yet elucidated. This prospective study was performed with the aim to compare the SSI rate in human immunodeficiency virus (HIV)-seropositive and HIV-negative patients and to identify other risk factors for this abdominal wound complication
METHODS: 98 patients who underwent small or large bowel resection and subsequent anastomosis due to penetrating abdominal trauma were included in the study. Injury related factors as well as demographical and physiological parameters, including HIV-status were analysed and superficial and deep SSI incidence rates were evaluated
RESULTS: Of the 98 patients, 23 patients (23%) were HIV-seropositive. The overall superficial SSI rate was 45% and the deep SSI rate was 15%. No significant difference in SSI (superficial or deep) in the HIV-seropositive and -negative group was demonstrated (superficial SSI HIV-pos vs HIV-neg: 61% vs 40%; p=0.172, deep SSI 22% vs 13%, p=0.276). Multivariate analysis identified five independent risk factors for SSI: postoperative CD4 count < 250 cells/μ!, postoperative albumin < 30 g/L, relook operation, anastomotic leak and colonic anastomosis
CONCLUSION: HIV-infection is not an independent risk factor for developing SSI after penetrating abdominal trauma. Low postoperative CD4 count, irrespective of HIV status, low postoperative albumin, relook operation, anastomotic leak and colonic anastomosis are predictors for SSI irrespective of the HIV-serostatus. These factors should be considered in unison during the decision-making process of abdominal wound closure; planned secondary wound treatment or immediate application of negative pressure dressings in patients with a high-risk profile may decrease the hospital stay and the financial burden on the health care system
Introduction
Surgical site infection (SSI) is one of the most common complications after abdominal surgery.1 Abdominal wound complications have severe socioeconomic consequences due to a prolonged hospital stay that places financial strain on the health care system and negatively impacts on the employment of patients due to a prolonged absence.2 Deep SSI, in particular, may require further surgical procedures which are associated with additional costs and increased morbidity.
Emergency abdominal surgery is associated with a higher risk of developing wound infections compared to elective surgery.3 During surgery for abdominal trauma, fecal contamination especially from colonic injuries is an established risk factor for wound infections.4,5
The role of HIV-infection in the development of SSI after abdominal trauma is not yet fully elucidated. It has been demonstrated that in the context of trauma, the percentage of HIV-positive patients is higher compared to the seroprevalence in the general population.6 However, there is a paucity of research that focuses on the impact of HIV on trauma patients. This context is limited further by the heterogeneity of trauma patterns that have been investigated.78 It is still debated as to whether the impaired immune status of these patients leads to a higher rate of surgical site infections after surgery.9
The principal aim of this study is to investigate whether SSI occurs more frequently in HIV-infected patients and furthermore to identify other risk factors that influence abdominal wound complications after surgery for penetrating abdominal trauma with bowel involvement.
Patients and methods
Data was collected prospectively from patients who were treated in the Trauma Unit at Chris Hani Baragwanath Academic Hospital from January 2017 to January 2018. Ethical approval was obtained from the Human Research Ethics Committee of the University of Witwatersrand (certificate number M 170143) and all the participants provided informed consent.
Subsequently admitted patients with penetrating abdominal trauma were included in this study if injury occurred to the lower gastrointestinal tract, as confirmed intraoperatively, thus requiring resection and small bowel anastomosis or colonic primary repair/anastomosis. Patients were excluded if they were younger than 18 years of age, if they presented with penetrating abdominal trauma without bowel injury, if they refused to be tested for HIV and thereby could not be classified, if they suffered from uncontrolled diabetes mellitus or active tuberculous infection, if there was history of prolonged steroid use, pelvic irradiation, pre-existing organ failure or demised within the first three days of the trauma.
Preoperative resuscitation was as per advanced trauma life support (ATLS) guidelines and all patients received preoperative antibiotic prophylaxis with amoxicillin/ clavulanic acid. A consultant trauma surgeon was present during all operations, the fascia of the abdomen was closed in all cases of definitive surgery continuously with polydioxanone (loop), the skin with metallic skin staples. Prolonged preoperative hypotension (systolic blood pressure < 90 mmHg, requirement of inotropes, metabolic acidosis (pH < 7.2, Lactat > 5), hypothermia (< 34°C) and presence of coagulopathy were indications for damage control surgery (DCS). After DCS, a vacuum dressing was applied and closure was attempted as soon as the abdominal situs allowed. If closure of the abdomen was not possible due to abdominal sheath retraction, the patient was discharged after skin grafting of the granulated situs (open abdomen).
Mechanism of injury, basic demographic information, presenting vital signs, arterial blood gas and results of routine blood tests were collected during admission to the trauma unit. The HIV-status was assessed in all the patients and the viral load was measured in the HIV-positive patients. CD4 counts and albumin levels were confirmed in all patients, 24 hours after surgery. The postoperative CD4 count in HIV-infected and non-infected patients was subdivided as per the Centre for Disease Control and Prevention (CDC) CD4-lymphocyte classification system for HIV infection.
Intraoperatively the severity of the intra-abdominal injury was graded using the penetrating abdominal trauma index (PATI)10 and the American Association for the Surgery of Trauma (AAST)-score.11 The anastomotic technique, whether or not a damage control approach was followed, inotrope use and blood transfusions were documented. All complications were recorded.
The primary endpoint of the study was to determine the rate of postoperative superficial and deep SSI as well as closure rate of the abdomen in HIV-infected patients compared to HIV-negative patients. SSI were divided into superficial and deep; superficial SSI was defined as an infection of the skin incision site with purulent drainage within 30 days of surgery involving the skin and subcutaneous tissue while the deep SSI involved muscle and fascial layers with purulent drainage and spontaneous dehiscence of the fascia.12
Statistical methods
All patients with complete data included in the prospectively collected database were evaluated in the analyses. No sample size calculation was performed.
Descriptive statistics were presented in the tables for all the above mentioned characteristics. Univariate logistic regression analyses were performed to determine the significant factors associated with superficial and deep SSI. Subsequently, the statistically significant factors were included in multivariate logistic regression analysis model. All multivariate analyses were adjusted by age. Cases with missing data were excluded from the analyses. All statistical analyses were conducted using SPSS computer program version 24.0.
Results
One hundred patients were recruited for the study, 2 of them were excluded because they did not agree to be tested for HIV so that finally 98 patients were analysed. At admission 6.3% of the patients were hypotensive (SBP < 90 mmHg) and 25.6% had a base excess less than -7.5 mmol/l.
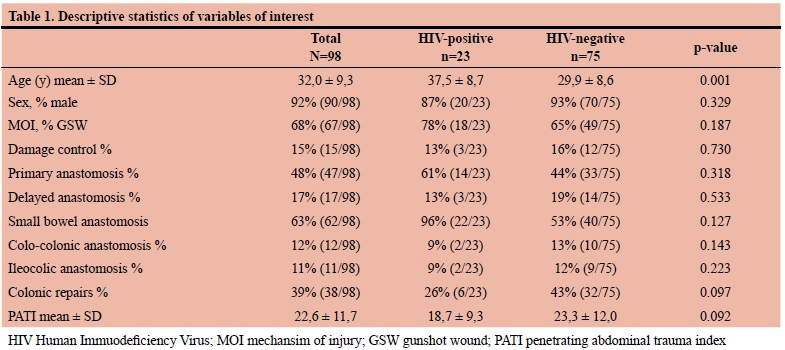
Of the 98 patients, 18 required more than one anastomosis; of the colonic injuries 37% were located in the right hemi-colon and 63% in the left hemi-colon. No significant differences were demonstrated in the HIV-seropositive and -negative groups regarding the number of small bowel and large bowel repairs, severity and mechanism of the sustained injuries and the number of cases of DCS (Table 1).
The analysis of the whole study group revealed significantly more SSI in patients who sustained GSW compared to stab wounds (superficial SSI: GSW vs. stab: 60% vs 13%, p < 0.001; deep SSI: GSW vs. stab: 21% vs 3%, p=0.024). Patients who were hypotensive at admission had significantly more dehiscence of the fascia postoperatively compared to normotensive patients (deep SSI: hypotensive vs. normotensive: 67% vs 12%, p=0.004).
Characteristics of HIV-infected patients, total postoperative CD4 count and albumin analysis
Among the HIV-seropositive patients, 8 (34.8%) were newly diagnosed on admission, 15 (65.2%) were aware of their retroviral status and received antiretroviral treatment (ART). In newly diagnosed patients, the mean viral load was 332.000+228.000 copies/ml. Of the patients who received ART, the mean viral load was 24.000+17.000 copies/ml and the mean ART duration was 20+7.2 (mean + SD) months.
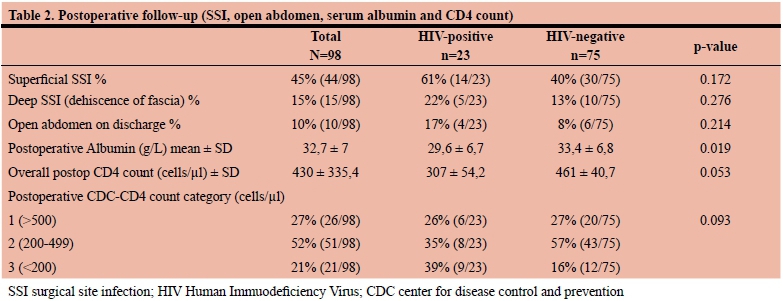
Postoperatively, 73% of the HIV-negative patients had CD4 counts in keeping with category 2 and 3 of the CDC-CD4 count classification; 33 patients (33.3%) had a CD4-count less than 250 cells/μ! which we used as the cut-off value for our risk calculations. The serum albumin was significantly lower in the HIV-positive patients 24 hours after surgery (Table 2).
The overall mortality rate in the study group was 7%. The patients were followed up in our outpatient clinic and the mortality was documented for the first 30 days after surgery. HIV-seropositive patients had a higher mortality rate than
HIV-negative patients (17% vs 4% in HIV-negative patients, p=0.086) but those results did not reach statistical significance.
SSI (surgical site infection and open abdomen)
There was no significant difference in superficial or deep SSI with regards to the HIV-status.
Among the HIV-seropositive patients, 5 of the 8 newly diagnosed patients and 8 of the 15 patients who were on antiretroviral treatment had a superficial SSI.
10% of the patients were discharged with an open abdomen because an abdominal closure could not be achieved (Table 2).
The patients who had damage control surgery had a significantly higher percentage of open abdomen at discharge (DC vs non-DC: 31.3% vs 3.6%, p-value < 0.001).
The difference in the hospital length of stay between the patients who had SSI and the patients without septic complications of the abdominal wound is shown in Table 3.
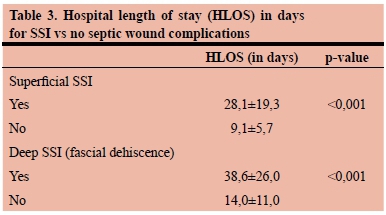
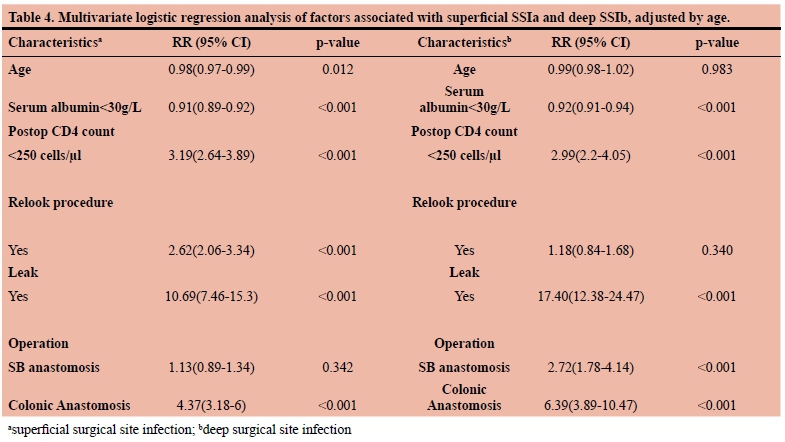
Table 4 shows the profile of patients who are at higher risk for developing a SSI. Patients with lower serum albumin levels, a CD4 count less than 250 cells/uL, with colonic repairs, relook laparotomies and anastomotic complications were more likely to have a SSI. Superficial and deep SSI have more or less identical risk factors. Relook procedures did not have a significant impact on dehiscence of the fascia. All data were adjusted by age.
Discussion
Reviewing the data from general surgery, there is controversy as to whether HIV-infected patients have an increased rate of surgical site infections and compromised wound healing.13,14 In our study we demonstrate that HIV-seropositive patients do not have a significantly higher incidence of superficial site infections or fascial dehiscence than HIV-negative patients after surgery for penetrating abdominal trauma. This research contributes perspective from a busy trauma unit at the largest hospital in Africa. The findings of this study are supporting the results of another trauma centre in South Africa that also compared the outcome of HIV-seropositive and -negative patients after penetrating abdominal trauma and did not identify a significant difference with regards to in-hospital mortality, intensive care unit admission rate, relaparotomy numbers, and hospital length of stay.15
The logistic regression analysis identified a CD4 count < 250 cells/μl as predictor for SSI independent of HIVserostatus.
In this study cohort 73% of the HIV-negative patients had a CD4 count below 500 cells/μl while 16% had a CD4 count less than 200 cells/μl, 24 hours after trauma and subsequent surgery.
These findings highlight the strong trauma- and surgical stress-induced influence on the adaptive immune system as evidenced by the finding of a decreased CD4 cell count in the group of healthy young HIV-negative males who lacked comorbidities. The extent to which each of these two factors, i.e. trauma and surgery, contributed to the fall of the T helper cells is not known, but the findings suggest that in trauma patients the stress-induced immunosuppression plays as an important role as the HIV-infection itself. HIV-infected patients with reconstitution of their CD4 count by ART seem to have a similar risk profile as HIV-negative trauma patients.
There is still uncertainty as to whether the T helper cell plays a role in the wound healing or if the T helper cell count is only an indicator of the potential of wound healing. Davis et al. showed in an animal experiment that animals with lower CD4 count had a significant decrease of strength and stability of the wound.16
Our findings reflect those of Tran et al. who followed up HIV-infected patients after general surgical procedures and demonstrated that the postoperative percent CD4 lymphocyte count and the decrement of percent CD4 lymphocyte count (preoperative to day one) were independent predictors for postoperative complications and infections.17 Chichom-Mefire et al. compared two groups of HIV-infected patients who underwent major abdominal surgery, both groups on ART with different preoperative CD4 counts, and noted a significantly higher rate of sepsis and a longer hospital stay in the patients with the lower CD4 count.18
Studies from orthopedic trauma revealed a trend towards higher rate of surgical site infection in HIV-infected patients. Guild et al. associated a low CD4 count (< 300 cell^l) in HIVpositive patients with an increased rate of septic complications after orthopedic surgery.19 With regards to the CD4 count, this observation is consistent with our finding where a CD4 count < 250 cell^l leads to a three-fold higher risk of developing a superficial SSI and having a postoperative fascial dehiscence.
Albumin, usually used to assess the nutritional status of patients, is an acute negative phase protein which decreases due to trauma and surgical stress.20 Low albumin levels are known to lead to a reduced collagen synthesis and impaired wound healing.21 In this study, patients with a low postoperative albumin level had significantly more superficial and deep SSI which aligns with previous studies that identified the albumin level as an independent predictor for SSI.22
Anastomotic leaks and colonic injuries
SSI may be an early sign for intraabdominal complications. Patients with anastomotic leaks had an almost 10-fold increased risk of having a surgical site infection. The risk for fascial dehiscence was increased nearly 20-fold which emphasizes the importance of investigating aggressively for an anastomotic leak in patients with deep surgical site infection.
According to previous trauma studies4,5 colonic injury was found to be another independent risk factor of developing SSI in this study population; increased bacterial loading of colonic stool exposes the patient to a higher risk of wound infection suggesting that patients with severe colonic fecal contamination may benefit from a secondary wound closure or an immediate negative pressure dressing postoperatively. The combination injury of colon and small bowel did not increase the risk profile compared to colonic injury alone.
Patients undergoing relook operations had a significantly higher risk of developing superficial SSI, which may be explained by the prolonged exposure and possible contamination of the subcutaneous tissue during the temporary closure of the abdomen.
It is noteworthy that in all cases, emergency surgery was performed and the procedures were classified as contaminated surgery.12 as there is spillage from the gastrointestinal tract into the abdomen subsequent to penetrating bowel injury contrasting to clean, elective surgery. The comparison with regards to the HIV-serostatus was not biased by trauma severity or mechanism as HIV-infected and -negative patients had no significant difference in the PATI, mechanism of injury nor in the number of damage control approaches.
Socioeconomic impact of open abdomen and SSI
When a patient who has an open abdomen is discharged from hospital, there is associated extensive morbidity and burden as this entails having a non-functional abdominal wall. Damage control surgery, more often performed in trauma than in general surgery, and postoperative complications lead to multiple relook procedures with the consequence of fascial retraction and finally the inability to close the abdomen. In almost one third of the patients who underwent damage control surgery the abdomen could not be closed before discharge and needed to be skin grafted after granulating. Loss of income for six to nine months especially for patients who are menial laborers engaged in physical work is the consequence of this morbidity followed by another hospital stay with complicated abdominal wall reconstruction. HIV-infected patients did not have a higher rate of open abdomen compared to HIV-negative patients (HIV-pos vs HIV-neg: 17% vs 8%, p=0.214), suggesting that trauma related factors exert a stronger influence on this complication than HIV-infection itself.
Prolonged hospital stay of patients with SSI is an enormous burden on the health care system.1 In this study, patients who suffered from a superficial SSI experienced a 3-fold longer hospital stay than the patients without septic wound complications. This problem is of even greater importance in areas of the world where clinics neither have the experience nor equipment to do complex wound dressings and where the medical network in the community cannot provide an appropriate follow-up of wound complications. Hence, the patients have to remain in hospital until their wounds are nearly healed.
Conclusion
This prospective study demonstrated that HIV-seropositive patients do not have significantly more frequent surgical site infections than HIV-negative patients after penetrating abdominal trauma with bowel involvement. Trauma-and surgical stress-induced decreased postoperative CD count, albumin level as well as colonic injury, anastomotic complications and relook operations are independent risk factors for postoperative wound complications. Patients with these risk factors may benefit from secondary wound closure or early application of negative pressure dressings to avoid prolonged hospital stay.
Conflict of interest
The authors declare that they have no conflict of interest.
REFERENCES
1. Badia JM, Casey AL, Petrosillo N, et al. Impact of surgical site infection on healthcare costs and patient outcomes: a systematic review in six European countries. J Hosp Infect. 2017;96(1):1-15. [PMID 28410761] Available at: http://dx.doi.org/10.1016/j.jhin.2017.03.004 [ Links ]
2. Weber WP, Zwahlen M, Reck S, et al. Economic Burden of Surgical Site Infections at a European University Hospital. Infect Control Hosp Epidemiol. 2008;29(7):623-9. [PMID 18564917] Available at: http://dx.doi.org/10.1086/589331 [ Links ]
3. Watanabe N, Suzuki M, Nomura H, et al. Risk factors for surgical site infection in emergency colorectal surgery: a retrospective analysis. Surg Infect. 2014;15(3):256-61. [PMID 24810804] Available at: http://dx.doi.org/10.1089/sur.2012.154 [ Links ]
4. Fabian TC, Croce MA. Management of penetrating colon injuries. Perspect Col Rect Surg. 1990; 5:24-49. [ Links ]
5. Bozorgzadeh A, Pizzi WF, Barie PS, et al. The duration of antibiotic administration in penetrating abdominal trauma. Am J Surg. 1999;177:125-31. [PMID 10204554] Available at: http://dx.doi.org/10.1016/S0002-9610(98)00317-1 [ Links ]
6. Sloan EP, McGill BA, Zalenski R, et al. Human immunodeficiency virus and Hepatitis B seroprevalence in an urban trauma population. J Trauma. 1995;38:736-41.[PMID 7760401] Available at: http://dx.doi.org/10.1097/00005373-199505000-00010 [ Links ]
7. Duane TM, Sekel S, Wolfe LG, et al. Does HIV Infection Influence Outcomes After Trauma? J Trauma. 2008;65(1):63-5. [PMID 18580533] Available at: http://dx.doi.org/10.1097/TA.0b013e318065c02a [ Links ]
8. Guth A, Hofstetter S, Pachter H, et al. Human immunodeficiency virus and the trauma patient: factors influencing postoperative infectious complications. J Trauma. 1996;41(2):251-6. [PMID 8760532] Available at: http://dx.doi.org/10.1097/00005373-199608000-00009 [ Links ]
9. Kigera JWM, Straetemans M, Vuhaka SK, et al. Is There an Increased Risk of Post-Operative Surgical Site Infection after Orthopaedic Surgery in HIV Patients ? A Systematic Review and Meta-Analysis. PLoS ONE. 2012;8(8):e42254. [PMID 22905120] [ Links ]
10. Moore EE, Dunn EL, Moore JB, Thompson JS. Penetrating abdominal trauma index. J Trauma. 1981;21:439-45. [PMID 7230296] [ Links ]
11. Moore EE, Cogbill TH, Malangoni MH, et al. Organ injury scaling, ll: pancreas, duodenum, small bowel, colon, and rectum. J Trauma. 1990;30(11):1427-9. [PMID 2231822] [ Links ]
12. Center for Disease Control and Prevention. Procedure-associated module SSI. Available at: https://www.cdc.gov>9pscssicurrent [ Links ]
13. Consten HJ, Slors EC, Noten FJ, et al. Anorectal surgery in human immunodeficiency virus-infected patients: clinical outcome in relation to immune status. Dis Colon Rectum. 1995;38:1169-75. [PMID 7587759] Available at: http://dx.doi.org/10.1007/BF02048332 [ Links ]
14. Davis BG, Corless PA, Gazzard DJ, et al. Increased risks of wound complications and poor wound healing following laparotomy in HIV-seropositive and AIDS patients. Dig Surg. 1999;16:60-7. [PMID 9949269] Available at: http://dx.doi.org/10.1159/000018695 [ Links ]
15. McPherson D, Neuhaus V, Dhar R, et al. The effect of Human-Immunodeficiency Virus status on outcomes in penetrating abdominal trauma: an interim analysis. World J Surg. 2018;42(8):2412-2420. [PMID 29387958] Available at: http://dx.doi.org/10.1007/s00268-018-4502-4 [ Links ]
16. Davis PA, Corless DJ, Aspinall R, et all. Effect of CD4(+) and CD8(+) cell depletion on wound healing. Br J Surg. 2001;88(2):298-30. [PMID 11167885] Available at: http://dx.doi.org/10.1046/j.1365-2168.2001.01665.x [ Links ]
17. Tran HS, Moncure M, Tarnoff M, et al. Predictors of operative outcome in patients with human immunodeficiency virus infection and acquired immunodeficiency syndrome. Am J Surg. 2000;180(3):228-33. [PMID 11084136] Available at: http://dx.doi.org/10.1016/S0002-9610(00)00450-5 [ Links ]
18. Chichom-Mefire A, Azabji-Kenfack M, Atashili J. CD4 count is still a valid indicator of outcome in HIV-infected patients undergoing major abdominal surgery in the era of highly active antiretroviral therapy. World J Surg. 2015;39(7):1692-9. [PMID 25663010] Available at: http://dx.doi.org/10.1007/s00268-015-2994-8 [ Links ]
19. Guild GN, Moore TJ, Barnes W, et al. CD4 count is associated with postoperative infection in patients with orthopaedic trauma who are HIV positive. Clin Orthop Relat Res. 2012;470(5):1507-12. [PMID 22207561] Available at: http://dx.doi.org/10.1007/s11999-011-2223-1 [ Links ]
20. Sung M, Bochicchio J, Joshi GV. Admission serum albumin is predictive of outcome in critically ill trauma patients. Am J Surg. 2004;70:1099-102. [PMID 15663053] [ Links ]
21. Ward MR, Danzi MW, Lewin M, et al. The effects of subclinical malnutrition and refeeding on the healing of experimental colonic anastomosis. Br J Surg. 1982;69:308-10. [PMID 6805546] [ Links ]
22. Hennessey DB, Burke JP, Ni-Dhonochu T, et al. Preoperative hypoalbuminemia is an independent risk factor for the development of surgical site infection following gastrointestinal surgery: A multi-institutional study. Ann Surg. 2010;252(2):325-9. [PMID 20647925] Available at: http://dx.doi.org/10.1097/SLA.0b013e3181e9819a [ Links ]
 Correspondence:
Correspondence:
Dr Martin Mauser
mtmauser@gmx.de


{kind=link}
{kind=link}
{kind=link}