










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.57 n.3 Cape Town Sep. 2019
http://dx.doi.org/10.17159/2078-5151/2019/v57n3a3000
TRAUMA
The consequences of major visceral vascular injuries on outcome in patients with pancreatic injuries: a case-matched analysis
JEJ KrigeI, III; EG JonasI, III; UK KotzeI, III; M SetshediII; PH NavsariaI, IV; AJ NicolI, IV
IDepartment of Surgery, Faculty of Health Sciences, University of Cape Town, South Africa
IIDepartment of Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
IIISurgical Gastroenterology and HPB Unit, Faculty of Health Sciences, University of Cape Town, South Africa
IVTrauma Centre, Groote Schuur Hospital, Cape Town, South Africa
ABSTRACT
BACKGROUND: Major pancreatic injuries are complex to treat, especially when combined with vascular and other critical organ injuries. This case-matched analysis assessed the influence of associated visceral vascular injuries on outcome in pancreatic injuries
METHOD: A registered prospective database of 461 consecutive patients with pancreatic injuries was used to identify 68 patients with a Pancreatic Injury combined with a major visceral Vascular Injury (PIVI group) and were matched one-to-one by an independent blinded reviewer using a validated individual matching method to 68 similar Pancreatic Injury patients without a vascular injury (PI group). The two groups were compared using univariate and multivariate logistic regression analysis and outcome including complication rates, length of hospital stay and 90-day mortality rate was measured
RESULTS: The two groups were well matched according to surgical intervention. Mortality in the PIVI group was 41% (n = 28) compared to 13% (n = 9) in the PI alone group (p = 0.000, OR 4.5, CI 1.00-10.5). On univariate analysis the PIVI group was significantly more likely to (i) be shocked on admission, (ii) have a RTS < 7.8, (iii) require damage control laparotomy, (iv) require a blood transfusion, both in frequency and volume, (v) develop a major postoperative complication and (vi) die. On multivariate analysis, the need for damage control laparotomy was a significant variable (p = 0.015, OR 7.95, CI 1.50-42.0) for mortality. Mortality of AAST grade 1 and 2 pancreatic injuries combined with a vascular injury was 18.5% (5/27) compared to an increased mortality of 56.1% (23/41) of AAST grade 3, 4 and 5 pancreatic injuries with vascular injuries (p = 0.0026
CONCLUSION: This study confirms that pancreatic injuries associated with major visceral vascular injuries have a significantly higher complication and mortality rate than pancreatic injuries without vascular injuries and that the addition of a vascular injury with an increasing AAST grade of pancreatic injury exponentially compounds the mortality rate
Keywords: pancreas, vascular, injury
Introduction
Major pancreatic injuries are among the most complex intraabdominal solid organ injuries to treat, especially when combined with adjacent organ and/or major vascular injuries.1 The close anatomic proximity of the inferior vena cava, portal vein, superior mesenteric vein and artery and aorta to the head and neck of the pancreas make these critical vessels vulnerable to injuries involving the proximal pancreas. Outcome is influenced by the cause and complexity of the pancreatic injury, the amount of blood lost, duration of shock, speed of resuscitation, number and type of associated injuries and the quality and magnitude of the surgical intervention.2 Mortality ultimately correlates with the cumulative impact of all injured organs and the total Injury Severity Score.3 In particular, gunshot wounds have the propensity to inflict substantial damage to both the pancreas and the peripancreatic vasculature with potentially dire consequences. The overall mortality rate of abdominal vascular injuries is 30% but may be as high as 68% for large capacitance visceral veins which is further compounded by the addition of a major pancreatic injury.4 Most early deaths are due to exsanguination after visceral vascular injuries rather than due to the pancreatic injury itself,3 while late mortality is generally a consequence of pancreas and adjacent organ damage resulting in intraabdominal and systemic septic complications or multi-organ failure.1,2
No other studies have assessed in detail the outcome in patients with pancreatic injuries when associated with specific visceral vascular injuries. Our group has previously evaluated multiple aspects of pancreatic trauma and has sufficient mature prospective granular data available in the high volume academic trauma centre to investigate organ-specific research questions.57 In view of the current lack of high quality clinical evidence the purpose of this data-driven analysis was to test the hypothesis that patients with combined pancreatic and major visceral vascular injuries have a worse outcome than pancreatic injuries without associated vascular injuries. In addition, the deleterious compounding consequences of specific and multiple associated vascular injuries were analysed. To accomplish this objective we performed a matched control study in a large cohort of consecutive patients using robust and reliable methodology and objective and reproducible clinical end-points.
Patients and methods
Study design
Following the STROBE guidelines for observational studies,8 a comparative case-matched analysis was done of consecutive patients who had a pancreatic injury combined with a major visceral vascular injury (PIVI) between January 1995 and December 2015 with pancreatic injury patients without a vascular injury (PI). Patient data were retrieved from a faculty approved and registered prospective database of all patients with pancreatic injuries treated in the Level 1 Trauma Centre and the Hepatopancreatobiliary and Surgical Gastroenterology units in Groote Schuur Hospital, Cape Town. Patients were manually matched one-to-one before outcome measures were reviewed in terms of type of intervention -pancreatoduodenectomy (PD), distal pancreatectomy (DP) or non-resection - by an independent reviewer according to a validated individual matching procedure.9 To reduce bias, investigators were blinded throughout the selection process to the primary and secondary end points in both groups during manual matching. Peri- and postoperative outcomes were compared between the PIVI group and the matched-pair PI group. The study design and analysis were approved by the appropriately convened Departmental and Institutional Ethics and Research Committees (HREC 293/2011). Data validation and quality-control procedures followed accepted international Good Clinical Practice guidelines and the study was conducted in accordance with the Declaration of Helsinki.
Data collection
Patient data collection, transcription and entry were performed by a trained surgical clinical reviewer and validated by a senior staff surgeon. Reliability audits were conducted on a regular basis to ensure data quality. Comprehensive details of the database have been documented previously.5-710 In short, data recorded for each patient used a specifically designed binary and narrative form comprising 60 items with 54 data fields. Variables recorded included demographic data, mechanism of injury, revised trauma score (RTS), associated visceral and non-visceral intra- as well as extra-abdominal vascular injuries, anatomic site and grade of pancreatic injury, operative findings and surgical management of the pancreatic and vascular injuries, the presence and type of pancreas-related and other complications, duration of hospital stay and mortality. Duration of hospital and ICU stay were expressed in calendar days.
Definitions
For the purpose of this study a major intra-abdominal visceral vascular injury was defined as an injury to either the aorta, inferior vena cava (IVC), portal vein (PV) or the superior mesenteric, renal and splenic vein or artery. Standardised definitions for events and outcome were used. Shock was defined as a systolic blood pressure less than 90 mm Hg. Pancreatic injury grade,11 pancreatic fistula,12 organ dysfunction,13 infectious complications and septic shock14 were defined and graded according to international consensus guidelines. Damage control laparotomy (DCL) was defined as an abbreviated emergency trauma laparotomy that required temporary abdominal closure and secondary definitive surgery.15 Morbidity was documented as systemic, intra-abdominal or specifically related to the pancreatic injury. Mortality was defined as in-hospital death due to any cause.
Initial management
Our general approach to complex pancreatic injuries has been described previously.5-7,10,15 Initial resuscitation was according to Advanced Trauma Life Support (ATLS) guidelines. Rapid preoperative evaluation included relevant physical examination, endotracheal intubation when necessary, insertion of resuscitation lines, selected trauma abdominal and cardiac sonography and chest radiographs. Urgent laparotomy was performed in patients who had clinical signs of peritonitis or evidence of major intra-abdominal bleeding. From 1995 onwards, haemodynamically unstable patients who had associated organ and visceral vascular injuries had an initial DCL before later definitive intervention.
Operative management of pancreatic injuries
Operative management of pancreatic injuries was based on the haemodynamic stability of the patient, the magnitude and extent of associated injuries and the location and severity grades of both pancreatic and duodenal injuries, details of which have been published.5-7 Minor lacerations of the pancreas without visible duct damage (AAST grade 1 and 2) were managed by suction drainage. Grade 3 injuries of the body and tail of the pancreas were treated by DP. Splenic preservation was used in haemodynamically stable patients. PD was restricted to patients who had non-reconstructable injuries due to destruction of the head of the pancreas, duodenum or ampulla (AAST grade 4 and 5) and was done as a primary procedure during the initial operation if the patient was stable or as a secondary staged procedure after the DCL.7,15 After resection suction drains were routinely placed.
Operative management of vascular injuries
The repair methodology, either direct primary repair, end-to-end anastomosis, interposition grafting or ligation, was determined by the patient's intraoperative physiologic status and the complexity of the vascular injury.16 The extent of operative exposure necessary was dictated by the site of the injured vessel. Urgent control of PV bleeding was achieved by the Pringle manoeuvre. Primary venorrhaphy was the preferred intervention in stable patients with PV injuries, but other operative strategies included ligation, end-to-end anastomosis and interposition grafting using harvested vein or Goretex were used when necessary and technically feasible. Access to the retro-pancreatic PV and superior mesenteric vein (SMV) necessitated division of the pancreatic neck for exposure in order to control the venous confluence. Lateral defects in the SMV were repaired with interrupted 5-0 polypropylene sutures. Extensive SMV and infrahepatic IVC injuries in hypotensive patients with profound shock were ligated.16
Damage control laparotomy
The decision to use DCL in critically injured patients was based on injury pattern, clinical status and the presence of severe metabolic acidosis (pH < 7.2), lactate > 5 mmol/L hypothermia (core temperature < 35°C), coagulopathy or > 10 units RBC transfusion.17
Management of postoperative intra-abdominal, pancreatic and duodenal complications
Postoperative intra-abdominal collections were drained with ultrasound or CT guided percutaneous catheters.
Endoscopically placed pancreatic duct stents were used for persistent pancreatic fistulas and covered self-expanding metal duodenal stents were used for complex duodenal leaks or fistulas.18
Study endpoints
The primary end points were overall in-hospital morbidity and mortality. Total operative time, intraoperative blood loss and length of hospital stay were secondary endpoints. Postoperative complications were recorded prospectively and graded according to the Clavien-Dindo complication score.19 When more than one complication occurred in a patient, only the most severe was taken into account for calculation of the complication grade in that patient.
Data analysis
Descriptive statistics reporting medians with ranges, and frequency distributions, were used to characterise the cohort. Between-group comparisons were made using the Student t-test or Wilcoxon sum rank test for normal and non-normally distributed data respectively. The Pearson's χ2 or Fisher's exact tests were used for analysis of categorical variables, and odds ratios (ORs) with 95 per cent confidence intervals (CI) were calculated. Univariate and then forward stepwise multivariate logistic regression analyses were performed to identify factors associated with the occurrence of complications. A p-value of < 0.05 was considered statistically significant. The data were analysed using Stata software version 11 (StataCorp LP, College Station, Texas, USA).
Results
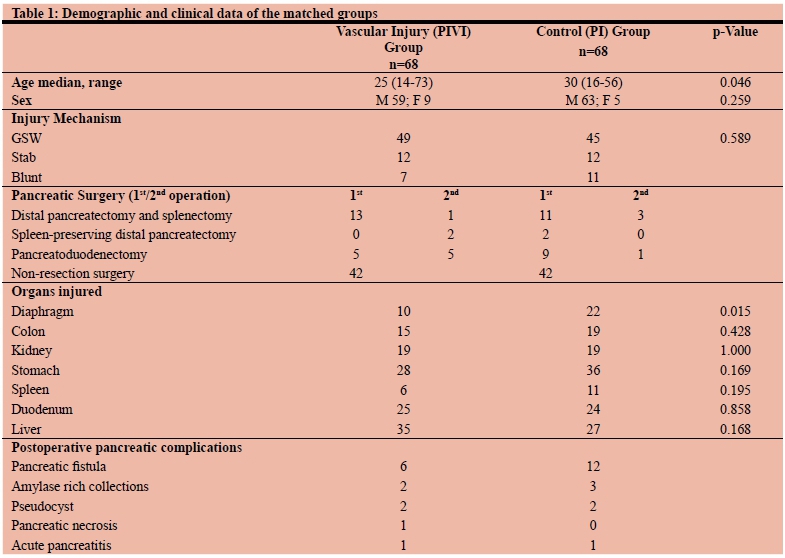
Of 461 consecutive patients with pancreatic injuries in the database 68 with a PIVI who required urgent surgery were matched to 68 with a PI without a vascular injury (Table 1). The groups were comparable with regard to mechanism of injury, AAST grade and associated injuries (Table 1). Although the control group was older by a median of 5 years (p = 0.0462), there was no statistical gender difference between the two groups (59/68 men in the PIVI group vs 63/68 in the control group, (p = 0.259).
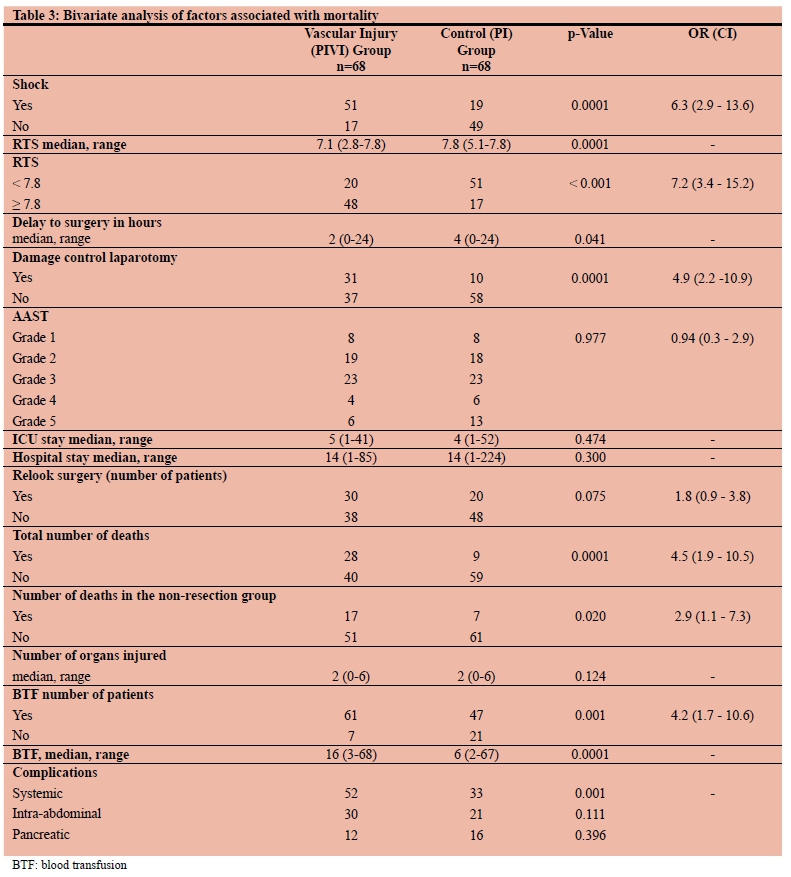
Patients in the PIVI group were more likely to be shocked and had a lower RTS than the PI group (Table 3). In the PIVI group 31/68 (45.6%) required a DCL compared to 10/68 (14.7%) in the PI only group (p = 0.0001). Mortality rates after DCL were similar, 65% (21/31) in the PIVI group compared to 60% (6/10) in the PI group (p = 0.653). Sixteen of the 21 deaths in the PIVI group after DCL were due to exsanguination in < 24 hours postoperatively compared to 2 deaths < 24 hours in the PI group due to head injuries. Three of ten patients who had a Whipple resection in the PIVI group died compared to one of ten in the PI group (0.263).
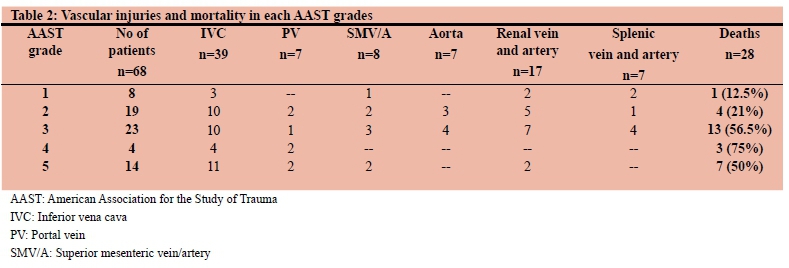
The PIVI group sustained injuries as shown in Table 2. Of patients with venous injuries 39 patients had IVC injuries and 17 (43.6%) died. Twenty-seven of the IVC injuries had a primary repair of whom 11 (40.8%) died. Twelve patients with profound shock and extensive loss of the caval wall as well as deteriorating physiological status with persistent hypotension, hypothermia, coagulopathy and worsening base deficit had ligation of the infrarenal IVC of whom 6 (50%) died. Eleven patients had an IVC injury combined with another visceral vascular injury of whom 8 (72.7%) died. Seven patients had PV injuries. Three patients had a PV injury only and all 3 survived after repair. Eight patients had either SMV only (n = 4) injured or combined with SMA or IVC or PV injuries (n = 4). All were repaired, and 2 (25%) survived. Four patients had triple vascular injuries with combined PV, IVC and SMV injuries and all four died despite repairs. Seven patients had aortic injuries repaired of whom 3 (42.9%) survived. Six of 17 patients (35.3%) with renal artery and/or vein injuries died, all of whom had other associated vascular injuries. Nine patients in the control group died, 5 of whom had associated liver and head injuries with DIC, while four died due to MOF and sepsis.
Overall mortality in the PIVI group was 41% (n = 28) compared to 13% (n = 9) in the PI only group (p = 0.0001). On bivariate analysis, the PIVI group were significantly more likely to (i) be shocked on admission, (ii) have a RTS < 7.8, (iii) require DCL, (iv) require a blood transfusion, both in frequency and volume, (v) develop a major postoperative complication and (vi) die (Table 3). On multivariate logistic regression analysis, only the need for DCL remained a significant variable (p = 0.015, OR 7.95, CI 1.50-42.0) for mortality. When combined with a vascular injury, mortality of AAST grade 1 and 2 pancreatic injuries was 18.5% (5/27) compared to an increased mortality of 56.1% (23/41) for AAST grade 3, 4 and 5 pancreatic injuries (p = 0.0026) (Table 4).
Discussion
This study provides strong evidence that pancreatic injuries, when combined with a major vascular injury, have a substantially worse outcome both in terms of morbidity and mortality. The case-matched controlled comparison demonstrated on univariate analysis that the addition of a vascular component to a pancreatic injury resulted in the greater likelihood of shock on admission, a lower RTS score, the need for damage control surgery, more frequent and larger volume blood transfusions and increased severe postoperative complications and death. While this observation intuitively may seem obvious, no previous papers have provided a detailed analysis of concomitant vascular injuries as a major risk factor for either disability or death in patients who have pancreatic injuries. We have previously shown in a stepwise multivariate logistic regression analysis model that 5 variables, age, shock, median number of units transfused and the presence of associated complications, were significant factors associated with mortality.6 In a study from our unit of 219 civilian pancreatic gunshot injuries, age, shock on admission, the need for damage control surgery, a high-grade AAST pancreatic injury and associated vascular injuries were associated with mortality on multivariate analysis.5 This study also confirms that pancreatic injuries associated with major visceral vascular injuries have a significantly higher complication and mortality rate than pancreatic injuries without vascular injuries and that the addition of a vascular injury with an increasing stage of pancreatic injury exponentially compounds mortality rate.
Several other studies which sought to detect predictors of mortality in patients with pancreatic trauma identified surrogate markers for blood loss but have not included vascular injuries as a major risk factor for death. An analysis from the Scottish Trauma Audit Group (STAG) database identified overall number of injuries, age, male sex, blunt trauma and shock as independent risk factors for death20 while increasing age, ISS and shock were variables predicting mortality after pancreatic trauma in an analysis from the Trauma Audit and Research Network (TARN) database in the UK.21 In a study from Louisville, Kentucky, Heitsch et al. reported a 34% mortality rate in patients with pancreatic trauma and found that death was more common in the presence of a pancreatic duct injury and gram-negative sepsis (p < 0.0001).22 Bradley et al. reported that mortality and morbidity increased when there was a delay in the detection of a pancreatic ductal injury.23 In a retrospective review from Bologna, Italy, Antonacci found that age, AAST grade, number of organs involved, hemodynamic status, intraoperative cardiac arrest and operative time were strongly predictive of mortality on multivariate analysis.24 Hwang and Choi from Korea reported that a greater than 12 unit blood transfusion and an initial base deficit of greater than -11 mM/L were significant predictors of mortality.25 In a retrospective review of 193 patients with a pancreatic injury admitted to their Level I trauma center in Seattle, Kao et al. reported that the grade of pancreatic injury was an independent predictor of mortality (odds ratio, 2.6; 95% CI 1.2-5.8).26
Visceral vascular injuries combined with pancreatic injuries are uncommon. Multiple associated injuries are typical, and act as important contributors to patient outcome.27 In a review of pancreatic injuries due to abdominal gunshot wounds treated at our institution, 27% of patients had an injury to a named abdominal vessel, most commonly the IVC.5 The mortality in the PIVI group in this study was 41% compared to 13% in the PI alone group. The reported mortality rate of intra-abdominal vascular injuries ranges from 32-54%.4 Shock, coagulopathy, multiple vessels injured and acidosis increase the mortality rate4 which exceeds 80% when the initial SBP is < 60 mm Hg and the base deficit is -15. IVC injuries accounted for 57% of the abdominal vascular injuries in this study of whom 43.6% died. Sixty-nine per cent had a primary repair while 31% with significant physiological derangement and extensive local caval injury had ligation as part of a damage control procedure. In this study, 28% of those with a caval injury had a second, major vascular injury, most commonly involving the aorta or portal vein. Clinical factors predicting poor outcome include shock on admission, persistent hypotension, anatomic level of the caval injury, associated visceral and vascular injuries, timing of diagnosis to definitive management, blood loss, requirements for blood transfusions, associated injuries, ED thoracotomy, preoperative lactate and base deficits, ISS, and GCS.28 Hypotension on admission occurs in two-thirds of patients and is the most important determinant of mortality. A sharp transition in mortality occurs with an increase in the number of associated injuries.29 Graham et al. reported that mortality increases to 50% with two vascular injuries and to 75% with more than two injuries.30
Similarly, superior mesenteric vein injuries are complex and are often associated with portal venous and SMA injuries with a high mortality for combined injuries.28 In this study, we found a similar mortality following ligation (33%) and repair (43%). In this study, all patients who had only a portal vein injury and a primary repair survived. Those with a second vascular injury had a mortality of 46.7% and those with triple vascular injuries involving PV, IVC and SMV all died despite repairs. In this group, surgical repair is technically difficult due to uncontrolled bleeding, difficult access and exposure and associated injuries. Mortality rates range from 50-70% and the most common cause of death is irreversible shock secondary to massive bleeding. The anatomical proximity of both the PV and the SMV to other vascular structures and organs explains the high incidence of associated injuries, and consequently a higher ISS, as observed in our series.
Several factors must be taken into account when interpreting the findings of this study. There are several limitations and caveats which may influence the interpretation of these data. Previous retrospective studies have focussed on the results of intra-abdominal vascular injuries alone and are hampered by discrepancies and weaknesses in their study design with limited numbers and selection bias. To the best of our knowledge this study is the first to investigate the detailed outcome of patients with combined pancreatic and vascular injuries. Unmeasurable biases may have had an influence on outcome and the results must be interpreted in this context. Despite extensive matching, our study is limited by its retrospective nature and relatively small sample size. Nonetheless, this study is the only comparative study using matched pair controls from a large prospective database which, in addition, minimised patient selection bias by using a blinded matching analysis. The strength of this study is that the data are sourced from a high volume academic trauma centre based on protocol driven intervention and collected by audited trained surgical clinical nurse reviewers to minimise measurement bias.
In conclusion, this study provides strong evidence that pancreatic injuries in combination with visceral vascular injuries have a significantly higher complication and mortality rate than pancreatic injuries without vascular injuries. Overall mortality in the combined pancreatic and vascular injury cohort was more than three times greater than the pancreatic sans vascular injury group. The PIVI group were significantly more likely to be shocked on admission, have a RTS < 7.8, require damage control surgery, require a blood transfusion, both in frequency and volume, develop a major postoperative complication and die. This study also showed that the addition of a vascular injury exponentially compounds mortality rate with each increasing stage of the pancreatic injury because mortality of AAST grade 1 and 2 pancreatic injuries combined with a vascular injury was 18.5% compared to a mortality of 56.1% for AAST grade 3, 4 and 5 pancreatic injuries.
Ethics approval
The study was approved by the University of Cape Town Human Research Ethics Committee and the study protocol conformed to the ethical guidelines of the "World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects" adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964, as revised in Tokyo 2004.
REFERENCES
1. Chrysos E, Athanasakis E, Xynos E. Pancreatic trauma in the adult: current knowledge in diagnosis and management. Pancreatology. 2002;2:365-78. Available from: http://dx.doi.org/10.1159/000065084 [ Links ]
2. Antonacci N, Di Saverio S, Ciaroni V, Biscardi A, Giugni A, Cancellieri F, et al. Prognosis and treatment of pancreaticoduodenal traumatic injuries: which factors are predictors of outcome? J Hepatobiliary Pancreat Sci. 2011;18:195-201. Available from: http://dx.doi.org/10.1007/s00534-010-0329-6 [ Links ]
3. Sorrentino TA, Moore EE, Wohlauer MV, Biffl WL, Pieracci FM, Johnson JL, et al. Effect of damage control surgery on major abdominal vascular trauma. J Surg Res. 2012;177:320-325. Available from: http://dx.doi.org/10.1016/jjss.2012.05.020 [ Links ]
4. Paul JS, Webb TP, Aprahamian C, Weigelt JA. Intraabdominal vascular injury: are we getting any better? J Trauma. 2010;69:1393-7. Available from: http://dx.doi.org/10.1097/TA.0b013e3181e49045 [ Links ]
5. Chinnery GE, Krige JE, Kotze UK, Navsaria P, Nicol A. Surgical management and outcome of civilian gunshot injuries to the pancreas. Br J Surg. 2012;99 Suppl 1:140-8. Available from: http://dx.doi.org/10.1002/bjs.7761 [ Links ]
6. Krige JE, Kotze UK, Setshedi M, Nicol AJ, Navsaria PH. Prognostic factors, morbidity and mortality in pancreatic trauma: a critical appraisal of 432 consecutive patients treated at a Level 1 Trauma Centre. Injury. 2015;46:830-6. Available from: http://dx.doi.org/10.1016/jinjury.2015.0L032 [ Links ]
7. Krige JE, Kotze UK, Setshedi M, Nicol AJ, Navsaria PH. Surgical Management and Outcomes of Combined Pancreaticoduodenal Injuries: Analysis of 75 Consecutive Cases. J Am Coll Surg. 2016;222:737-49. Available from: http://dx.doi.org/10.1016/jjamcollsurg.2016.02.005 [ Links ]
8. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370:1453-7. Available from: http://dx.doi.org/10.1016/S0140-6736(07)61602-X [ Links ]
9. Miettinen OS. Individual matching with multiple controls in the case of all-or-none responses. Biometrics. 1969;25:339-55. Available from: http://dx.doi.org/10.2307/2528794 [ Links ]
10. Thomson DA, Krige JE, Thomson SR, Bornman PC. The role of endoscopic retrograde pancreatography in pancreatic trauma: a critical appraisal of 48 patients treated at a tertiary institution. J Trauma Acute Care Surg. 2014;76:1362-6. Available from: http://dx.doi.org/10.1097/TA.0000000000000227 [ Links ]
11. Moore EE, Cogbill TH, Malangoni MA, Jurkovich GJ, Champion HR, Gennarelli TA, et al. Organ injury scaling, II: Pancreas, duodenum, small bowel, colon, and rectum. J Trauma. 1990;30:1427-9. [ Links ]
12. Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al; International Study Group on Pancreatic Fistula Definition. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery. 2005;138:8-13. Available from: http://dx.doi.org/10.1016/j.surg.2005.05.001 [ Links ]
13. Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101:1644-55. Available from: http://dx.doi.org/10.1378/chest.101.6.1644 [ Links ]
14. Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, et al; for the International Surviving Sepsis Campaign Guidelines Committee. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008;36:296-327. Available from: http://dx.doi.org/10.1097/01.CCM.0000298158.12101.41 [ Links ]
15. Krige JE, Navsaria PH, Nicol AJ. Damage control laparotomy and delayed pancreatoduodenectomy for complex combined pancreatoduodenal and venous injuries. Eur J Trauma Emerg Surg. 2016;42:225-30. Available from: http://dx.doi.org/10.1007/s00068-015-0525-9 [ Links ]
16. Navsaria PH, de Bruyn P, Nicol AJ. Penetrating abdominal vena cava injuries. Eur J Vasc Endovasc Surg. 2005;30:499-503. Available from: http://dx.doi.org/10.1016/j.ejvs.2005.08.004 [ Links ]
17. Timmermans J, Nicol A, Kairinos N, Teijink J, Prins M, Navsaria P. Predicting mortality in damage control surgery for major abdominal trauma. S Afr J Surg. 2010;48:6-9. [ Links ]
18. Chinnery GE, Bernon M, Krige JE, Grotte A. Endoscopic stenting of high-output traumatic duodenal fistula. S Afr J Surg. 2011;49:88-9. [ Links ]
19. Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250:187-196. Available from: http://dx.doi.org/10.1097/SLA.0b013e3181b13ca2 [ Links ]
20. Scollay JM, Yip VS, Garden OJ, Parks RW. A population-based study of pancreatic trauma in Scotland. World J Surg. 2006;30:2136-41. Available from: http://dx.doi.org/10.1007/s00268-006-0039-z [ Links ]
21. O'Reilly DA, Bouamra O, Kausar A, Malde DJ, Dickson EJ, Lecky F. The epidemiology of and outcome from pancreatoduodenal trauma in the UK, 1989-2013. Ann R Coll Surg Engl. 2015;97:125-30. Available from: http://dx.doi.org/10.1308/003588414X14055925060712 [ Links ]
22. Heitsch RC, Knutson CO, Fulton RL, Jones CE. Delineation of critical factors in the treatment of pancreatic trauma. Surgery. 1976;80:523-9. [ Links ]
23. Bradley EL 3rd, Young PR Jr, Chang MC, Allen JE, Baker CC, Meredith W, et al. Diagnosis and initial management of blunt pancreatic trauma: guidelines from a multiinstitutional review. Ann Surg. 1998;227:861-9. Available from: http://dx.doi.org/10.1097/00000658-199806000-00009 [ Links ]
24. Antonacci N, Di Saverio S, Ciaroni V, Biscardi A, Giugni A, Cancellieri F, et al. Prognosis and treatment of pancreaticoduodenal traumatic injuries: which factors are predictors of outcome? J Hepatobiliary Pancreat Sci. 2011;18:195-201. Available from: http://dx.doi.org/10.1007/s00534-010-0329-6 [ Links ]
25. Hwang SY, Choi YC. Prognostic determinants in patients with traumatic pancreatic injuries. J Korean Med Sci. 2008;23:126-30. Available from: http://dx.doi.org/10.3346/jkms.2008.23.1.126 [ Links ]
26. Kao LS, Bulger EM, Parks DL, Byrd GF, Jurkovich GJ.Predictors of morbidity after traumatic pancreatic injury. J Trauma. 2003;55:898-905. Available from: http://dx.doi.org/10.1097/01.TA.0000090755.07769.4C [ Links ]
27. Sullivan PS, Dente CJ, Patel S, Carmichael M, Srinivasan JK, Wyrzykowski AD, et al. Outcome of ligation of the inferior vena cava in the modern era. Am J Surg. 2010;199:500-6. Available from: http://dx.doi.org/10.1016/j.amjsurg.2009.05.013 [ Links ]
28. Asensio JA, Britt LD, Borzotta A, Peitzman A, Miller FB, Mackersie RC, et al. Multiinstitutional experience with the management of superior mesenteric artery injuries. J Am Coll Surg. 2001;193:354-66. Available from: http://dx.doi.org/10.1016/S1072-7515(01)01044-4 [ Links ]
29. Rosengart MR, Smith DR, Melton SM, May AK, Rue LW 3rd. Prognostic factors in patients with inferior vena cava injuries. Am Surg. 1999;65:849-56. [ Links ]
30. Graham JM, Mattox KL, Beall AC Jr. Portal venous system injuries. J Trauma. 1978;18:419-422. Available from: http://dx.doi.org/10.1097/00005373-197806000-00006 [ Links ]
 Correspondence:
Correspondence:
Prof JEJKrige
jej.krige@uct.ac.za


{kind=link}
{kind=link}
{kind=link}
{kind=link}