










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.57 no.2 Cape Town Jun. 2019
ABSTRACTS
47th Meeting of The Surgical Research Society of Southern Africa
University of Pretoria
ABSTRACT 1
MUTATIONAL PROFILING OF GALLBLADDER TUMOURS OBTAINED FROM SOUTH AFRICAN PATIENTS REVEAL NOVEL MUTATIONS
Devar J, Nweke E, Candy G, and Smith M
Department of Surgery, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand.
Background: Gall bladder cancer (GBC) is the sixth most prevalent digestive malignancy and the most common biliary-tract carcinoma. GBC is characterized with delayed diagnosis, ineffective treatment and poor prognosis. Consequently, GBC has a 5-year survival rate varying from 0-12%. Studies have shown that the incidence of GBC varies by both location and ethnicity. Information about the genetic changes occurring during GBC is limited especially in Africa.
Aim: This study aims to highlight genetic mutations in African GBC patients and observe differential expression of genes.
Methods: Ethics clearance was obtained from the Human Ethics Research Committee of the University of Witwatersrand (M160640). A pilot cohort of eight (8) Tru-cut biopsy tumors were collected from consenting patients in Chris Hani Baragwanath Hospital. Total RNA was extracted, and RNA sequencing performed. Differential gene expression and variant analysis were performed using the CLC-Bio Genomics workbench and the Ingenuity Variant Analysis tool. Functional analysis of gene variants was investigated using tools such as Polyphen-2 and WANNOVAR.
Results: Our results showed the mutational profile of gallbladder tumors in our patient cohort. We found 153 mutations including in pro-apoptotic genes leading to loss of function and in proto-oncogenes resulting in gain of function. RGPD6, a transcription factor, was the most mutated gene in tumours. The mutated genes were mostly enriched in cellular and metabolic processes. Interestingly, most of these identified mutations have not been previously described.
Conclusions: This study has uniquely identified the mutational profile of Gallbladder tumors in a South African cohort helping to elucidate the mechanism of progression of the disease. A more comprehensive study with larger sample size is required to validate these findings.
ABSTRACT 2
NOVEL TARGETS IN DYSREGULATED SIGNALLING PATHWAYS TO INHIBIT METASTASIS IN PANCREATIC DUCTAL ADENOCARCINOMA
Mhlambi NHM, Candy G, and Nweke EE
Department of Surgery, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand.
Introduction: Pancreatic cancer (PDAC) has a poor prognosis despite several treatment strategies. Hence, the discovery of potential new therapeutic targets is essential to improve outcomes. Dysregulation of several key pathways occur during pancreatic cancer. These pathways have been identified to be involved in cellular proliferation, invasion and migration. Aberrancy of these biological processes induced by dysregulated pathways can result to metastasis, a major cause of mortality in pancreatic cancer.
Aim: This study intends on utilizing pathway-based approach to identify potential therapeutic targets that impede metastasis.
Methods: Following ethics clearance, tissues were obtained from 15 consented PDAC patients. Subsequently, total RNA was extracted, and pathway focused PCR arrays used to identify expression of key signalling genes at different stages of PDAC progression. These targets were further validated using Real-time PCR.
Results: We observed the dysregulation of certain components of the Epithelial-to -Mesenchymal transition (EMT) pathway in resect able PDAC tumours. Genes such as ERCC3, POLB, and OCLN were upregulated, while GSC, KRT14, and SNAI3 downregulated. Additionally, genes involved in cell cycle (MCM2 and WEE1) and cellular senescence (ETS2, IGFBP3, IGFBP5, 1GFBP7, and SOD1) were upregulated with an average fold change of 3.
Conclusion: The upregulation of genes involved in cell cycle and senescence is indicative of increased cellular proliferation. Furthermore, increased expression of targets within the EMT pathway, may indicate aberrant cell migration and subsequently, metastasis. Targeting the components of these pathways may lead to inhibition of biological processes that induce metastasis.
ABSTRACT 3
ANGIOGENIC PATHWAYS ARE OVEREXPRESSED IN EARLY PANCREATIC DUCTAL ADENOCARCINOMA IN A COHORT OF SOUTH AFRICAN PATIENTS AFFECTING IMMUNE RESPONSE.
Nsingwane Z1, Candy GP1, Nweke EE1
1Department of Surgery, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand
Introduction: Pancreatic ductal adenocarcinoma (PDAC) is the most common type of pancreatic cancer with a poor prognosis and survival rate of 5 years for only 5% of patients. PDAC is asymptomatic at its early stages and characteristically aggressive in nature as it progresses. The immune system has been observed to be activated during PDAC, however, cancer cells develop mechanisms to evade detection. Avoiding immune recognition and destruction has been identified as an emerging hallmark of cancer. Angiogenic pathways are crucial in cellular development and growth, however their dysregulation would result in uncontrolled proliferation of cells affecting immune response. Understanding how immune system acts is essential to developing effective therapeutic options. This study aims to describe the expression profile of immune-related genes in pancreatic cancer progression.
Methods: In this study, 30 tissues (15 tumour and 15 corresponding normal tissues) were obtained from early PDAC African patients at Chris Hani Baragwanath academic hospital in Johannesburg after ethics approval. Furthermore, we performed secondary analysis of previously obtained RNA sequencing data obtained from four tissue samples (2 tumours and 2 corresponding normal samples) targeted to immune pathways to identify those that may be involved in PDAC disease progression.
Results: Our analysis showed the upregulation of angiogenic pathways such as the fibroblast growth factor (FGF) and vascular endothelial growth factor (VEGF). Also, we observed that immune response pathways (including those of innate and adaptive response) were simultaneously activated.
Conclusions: This study corroborates others that have identified the overexpression of angiogenic factors in PDAC progression. Tumour cells avoid recognition and subsequent elimination by secreting these angiogenic factors. Thus, the overexpression of these factors induces tumour growth and migration and provide a mechanism of immune system evasion. Thus, targeting these mechanisms might prove beneficial for the development of immune-based therapeutic strategies for PDAC treatment.
ABSTRACT 4
POLYMER CONJUGATION IMPROVES THE ANTICANCER ACTIVITY OF BETULINIC ACID AND DIHYDROARTEMISININ AGAINST PANCREATIC CANCER CELLS
Mthimkhulu N1, Mvango S2, Balogun M2, Jones-Omoshoro J1, Devar J1, Fonteh P1
1Department of Surgery, WITS University, Johannesburg, South Africa
2Biopolymer Modification & Therapeutics Lab, CSIR, Pretoria, South Africa
Introduction: Pancreatic cancer is the fourth leading cause of cancer deaths worldwide and one of the most drug-resistant cancer. Conventional treatment for pancreatic cancer has shortcomings including lack of specificity and multi-drug resistance. Drug delivery systems like polymer therapeutics have reportedly improved the potency and pharmacokinetics of cancer drugs.
Aim(s): The aim of the project was to synthesize, characterize, and screen betulic acid (BA) and dihydroartemisinin (DHA) polymer conjugates against a pancreatic cancer cell line Mia PaCa-2, normal cell line (Vero) and PBMCs.
Methods: The parent drugs BA and DHA were conjugated to PEG and Chitosan polymers using carbodiimide chemistry. The cytotoxicity of the conjugates was tested using tetrazolium salts on MIA-PaCa-2, Vero, and peripheral lymphocytes at concentrations ranging from 0.4-100μM. (37°C, 72 hours). Selected concentrations were further used to determine the mode of cell death using flow cytometry. The antioxidant potential of the conjugates was tested using a free radical scavenging assay. Ethics approval was obtained from the HREC Medical of the University of the Witwatersrand.
Results: The conjugates had lower IC50 values than the parent drugs, suggesting an increased potency. Conjugate cytotoxicity was higher on MIA PaCa-2 cells compared to Vero and PBMCs. The precursor compounds showed no toxicity suggesting that most of the cytotoxicity observed was as a result of conjugation. Selective cytotoxicity was observed for BA-PEG (SI =3.7 μM) with more apoptosis on MIA-PaCa-2 cells compare to Vero cells and PBMCs confirming the observed selectivity. The conjugates further showed antioxidant potential with IC50s of 11.22 ±0.10, 12.02±0.09 and 15.48±1.00 for BA-PEG, DHA-PEG and DHA-Chitosan, respectively.
Conclusion/Recommendations: The conjugation of natural compounds such as BA to polymers holds potential for increasing the anticancer activity. This could provide a platform for the development of more potent and specific natural-based anticancer drugs
ABSTRACT 5
LAPAROSCOPIC APPENDECTOMY FOR COMPLICATED APPENDICITIS, DOES THE DRAIN MAKE ANY DIFFERENCE? RANDOMISED PROSPECTIVE STUDY
Anyisha AP
Department of General Surgery, Dr George Mukhari Academic Hospital, Sefako Makgatho Health Sciences University
Introduction/Background: Laparoscopic appendectomy (LA) has been increasing in last decades. Its role in complicated appendicitis (CA) is debatable. Concerns persist about post-operative collection rates after LA for CA.
Aim: To compare the outcome of the patients following LA for CA with use of a drain vs those without drain.
Methods: A prospective randomised controlled study was conducted. Patients >13 years with acute appendicitis were recruited. Consented qualifying patients were randomised to two arms: Drain Group (DG) and No Drain Group (NDG). Qualifying patients were offered standard LA with pus suction only. Surgeons were senior residents. The two groups were subjected to the same standard post-operative care. The primary end point was the rate of postoperative intraabdominal collection (POIAC). Patients with suspected POIAC were confirmed by imaging or a relook surgery. The rate of POIAC was statistically compared between the two groups.
Results: In total 168 patients were diagnosed with acute appendicitis and operated. Eighty-two patients had simple appendicitis and 86 had CA. Twenty were excluded: 15 were done via laparotomy and five were converted to laparotomy. Sixty-six patients qualified and were randomised to two arms: 33 in each group. Rate of POIAC was compared between the two groups. In the DG 6 (18.18%) patients had POIAC vs 20 (60.61%) in NDG (p<0.001). One patient in the DG had major resection and one in the NDG died. The mean and median for hospital stay and for duration of antibiotics did not differ between the two groups. The power of the Fisher Exact test, performed at the two-sided 0.05 significance level, to detect a difference between 18.2% and 60.6% (42.4%) with 33 patients per group, was 93.6%.
Conclusion: POIAC was higher in the NDG. The difference between the two groups was statistically significant; p-value<0.001. The use of drain reduced the rate of POIAC by 42.4%.
ABSTRACT 6
DEVELOPING A TRAUMA REGISTRY IN A MIDDLE INCOME COUNTRY - BOTSWANA
Motsumi MJ1, Mashalla Y2, Sebego M3, Ho-Foster A4, Motshome P5, Mokokwe L4, Mmalane M6, Montshiwa T1
1Department of Surgery, Faculty of Medicine, University of Botswana
2Faculty of Health Sciences, University of Botswana
3School of Nursing, University of Botswana;
4Botswana-UPenn Partnership, University of Pennsylvania Perelman School of Medicine;
5Health and Wellness Centre, University of Botswana; 6Botswana Harvard AIDS Institute
Background: Injury is a major public health problem globally causing almost 6 million deaths per year.
Aims: To develop and pilot a road traffic accident trauma registry prototype and assess the completeness of data collected using the registry prototype and existing collecting data collection tools.
Methods: A cross sectional study was piloted at a tertiary hospital and a secondary level hospital in Botswana. The study consisted of two parts: Part One mainly involved stakeholder consultations on existing data collection tools. Part Two consisted of two phases: Phase I involved retrospective collection of existing data from existing data collection tools and Phase II collected data prospectively using the proposed trauma registry prototype.
Results: The pre-hospital road traffic accident data is collected using hard copy forms and some of this data is transferred to a stand-alone electronic registry. The hospital phase of road traffic accident data all goes into hard copy files then stored in institutional registry departments. The post-hospital data is also partially stored as hard copies and some data is stored in a stand-alone electronic registry. The demographics, pre-hospital, triage, diagnosis, management and disposition had a high percent completion rate with no significant difference between phases I and II. However, the primary survey variables in Phase I had a low percent completion rate which was significantly different from the high completion rates in phase II at both hospitals. A similar picture was observed for the secondary survey at both hospitals.
Conclusion: We developed and successfully piloted the road traffic accident trauma registry at two hospitals in Botswana. There is high data completion rate when using the electronic data registry as opposed to data collected using the paper-based/hardcopy existing data collection tools. We recommend the adoption and implementation of the trauma registry prototype in Botswana's health system.
ABSTRACT 7
INTEGRATION OF PROTEOMICS AND GENOMICS DATA DEMONSTRATES NOVEL POTENTIAL MECHANISMS OF PANCREATIC DUCTAL ADENOCARCINOMA IN BLACK AFRICAN PATIENTS
Nweke E1, Naicker P2, Stoychev S2, Devar J1, Candy G1
1Department of Surgery, University of Witwatersrand
2Department of Biosciences, Centre for Scientific and Industrial Research
Background: Pancreatic cancer (PDAC) accounts for 2.8% of new cancer cases worldwide and is projected to become the 2nd leading cause of cancer-related deaths by 2030. Patients of African ancestry appear to be at increased risk for PDAC with worse severity and outcome. The asymptomatic nature of this cancer, lack of specific diagnostic tests and aggressiveness account for low survival rates. Integrating protein and genome expression profiles help identify and better understand molecular variations in a disease. Thus, provide an avenue for discovery of better novel diagnostic, prognostic and therapeutic targets.
Aim: This proposed study seeks to describe and integrate protein and genomic profiles of black African PDAC patients.
Methods: The Human Research Ethics Committee of the University of Witwatersrand issue clearance for this study (M150778). Thirty tissues (15 tumours and 15 corresponding normal) were obtained from consenting black African PDAC patients undergoing Whipple procedure at Chris Hani Baragwanath and Donald Gordon Hospitals in Johannesburg. Samples were processed to obtain protein and DNA; subsequently used for protein arrays, SWATH-MS and DNA oncology arrays. The mutational profile obtained from DNA arrays was compared to databases such as TCGA to identify unique mutations which was then linked to protein expression. Pathway analysis was performed on proteins of interest using GeneMania, KEGG and REACTOME.
Results: We found significantly dysregulated proteins in tumour samples involved in key biological processes including cell cycle and Epithelial-Mesenchymal-Transition. Of interest, are novel mutations in genes such as COLIA1 TGM2, SPARC, and ZFHX3 which may play anti-tumorigenic roles. Additionally, these mutated genes also showed dysregulated expression.
Conclusion: The increased prevalence and mortality observed in PDAC patients of African ancestry across diverse population has been observed. This study has described protein expression and mutations observed in this subset of patients, therefore highlighted novel targets in PDAC.
ABSTRACT 8
INDICATIONS AND OUTCOMES FOR NON-TRAUMA EMERGENCY LAPAROTOMY: A COMPARISON OF RWANDA, SOUTH AFRICA AND THE UNITED STATES
Pohl L1, Richard J2, Abahuje E3,4, Coughlin A2, Englbrecht S1, Kariem N15, Kloppers C', Malatji S5, Sibomana I3, Chu K1,5
1Department of Surgery, University of Cape Town, Cape Town, South Africa
2Department of Surgery, University of Minnesota, Minneapolis, MN
3Department of Surgery, University of Rwanda, Kigali, Rwanda
4Department of Surgery, University Teaching Hospital of Kigali, Kigali, Rwanda
5Department of Surgery, New Somerset Hospital, Cape Town, South Africa
Background: Emergency surgical conditions requiring exploratory laparotomy (EL) can be challenging especially when patients present late with complicated disease.
Aims: The objective of this study was to describe the indications, outcomes, and risk factors for perioperative mortality after non-trauma EL in Rwanda, South Africa and the United States (U.S.)
Methods: This was a prospective study conducted at four hospitals in Rwanda, South Africa, and the United States from September 1, 2017 to August 31, 2018. All adult patients undergoing non-trauma EL were included.
Results: During the 12-month period, there were 633 EL at the four hospitals. Median age was 45 years (interquartile range 31, 61) and 354 (56%) were male. Overall, the most common indications for EL were appendicitis (n=133, 21%), peptic ulcer disease (n=101, 16%), and hernia (n=74, 12%). The most common indications in Rwanda were appendicitis (n=41, 19%) and hernia (n=37, 17%); in South Africa appendicitis (n=91, 28%) and peptic ulcer disease (n=60, 19%); and in the U.S., peptic ulcer disease (n=16, 19%) and adhesions leading to small bowel obstruction (n=16, 19%). Perioperative mortality rate (POMR) was 9%, with no statistical difference between hospitals (Rwanda 7%, South Africa 12%, U.S. 16%, p=0.173). Risk factors associated with increased POMR included high American Society of Anaesthesiologist score (ASA3) (adjusted odds ratio (aOR): 4.37, 95% confidence interval (CI): 1.91, 9.96, p= <0.001), age > 60 years (aOR: 3.10, 95% CI: 1.46, 6.59, p= 0.003) and reoperation (aOR: 2.43, 95% CI: 1.05, 5.63, p= 0.038). Appendicitis (aOR: 0.20, 95% CI: 0.04, 0.99, p= 0.050) and hernia (aOR: 0.28, 95% CI: 0.08, 0.97, p= 0.044) were associated with decreased POMR.
Conclusion: Emergency surgical conditions requiring EL vary between countries and POMR is high regardless of income setting.
ABSTRACT 9
IMMUNOHISTOCHEMISTRY ANALYSIS OF MACROPHAGES, DENDRITIC CELLS AND T LYMPHOCYTES MARKERS IN BREAST CANCERTISSUE SAMPLES AT AN ACADEMIC HOSPITAL IN TSHWANE
Mhlongo LN1, Mathebela PN1, Mokoena T1, Bida NM2
1Department of Surgery, University of Pretoria
2Department of Anatomical Pathology, University of Pretoria
Introduction/Background: The breast microenvironment has diverse capabilities to induce either beneficial or adverse consequences in genesis. The complex tissue microenvironment, which consists of cellular and non-cellular constituents, sustains the tumour; it may support tumour development, sustain and determine its growth, invasion and metastasis.
Aim(s): The aim of the study is to determine and quantify the phenotypes of macrophages, dendritic cells and T Lymphocytes in breast cancer tissue samples at SBAH-NHLS.
Methods: Samples included in this study were retrospective archival formalin fixed paraffin embedded tissue samples previously diagnosed with breast cancer from 2012-2018. A qualified pathologist assessed the eligibility of the tissue blocks for further studies. Specialised immunohistochemical stains were done on the cases. The University of Pretoria ethics committee approved the study: 196/2018.
Results: The sample consisted of 54 FFPE pre-selected tissue samples previously diagnosed with breast cancer, 100% female with age range between 30-98 and mean of 55. Histological distribution; 56% were ductal, 13% mucinous, 9% papillary, 7% comedo, 5 % lobular, 4% tubulolobular and 4% medullary carcinoma. P24 was expressed in 20.4%, CD3 in 100%, CD4 in 18.5%, CD8 in 90.7%, CD68 in 88.7%, CD163 in 65.6%, CD207 in 100%, CD208 in 30%, CD122 in 64.3% and FOXP3 was not detected in all cases.
Conclusion/Recommendations: The results show a higher level of macrophages, dendritic cells and cytotoxic T-cells, a decreased expression of helper T-cell and regulatory T-cells. The functional activated macrophages and dendritic cells were minimal within the tumour microenvironment; our findings explain an impaired secondary immune response in these breast cancer tissue samples.
ABSTRACT 10
IN SITU DETERMINATION OF NATURAL KILLER CELLS ANTITUMOUR IMMUNITY IN BREAST CANCER CELLS AT AN ACADEMIC HOSPITAL IN TSHWANE
Mhlongo LN1, Mathebela PN1, Mokoena T1, Bida NM2
1Department of Surgery, University of Pretoria
2Department of Anatomical Pathology, University of Pretoria
Introduction/Background: Breast cancer remains one of the common cancers leading to mortality and morbidity of women worldwide (WHO, 2008). Natural killer cells function to control local tumour growth and metastasis due to their ability to exert cellular cytotoxicity without any activation (Schreiber et.al, 2011). The type, density and location of immune cells on the tumour microenvironment predict clinical outcomes and the overall patient prognosis. Both the adaptive and innate immune responses play a significant role in anti-tumour responses, the interactions between the pathways of the innate and adaptive immune responses serve as an alternative to the development of an effective cancer therapy.
Aim(s): The aim of the study is to determine, locate and quantify Natural Killer cells in breast cancer tissue samples at SBAH-NHLS.
Methods: The study sample consisted of 50 formalin fixed paraffin embedded cases diagnosed with breast cancer at Steve Biko Academic Hospital-National Health Laboratory Services Anatomical Pathology Department from 2013- 2018. Immunohistochemistry markers were done on histology blocks pre-selected by pathologist. The University of Pretoria ethics committee approved the study (482/2017).
Results: All the patients were female, age range 30-98, with a mean of 55. Natural killer cells (NKCs) marker CD56 was expressed in 32.3% of the samples, and mature functional NKCs marker CD57 was expressed in 62.5% of the breast cancer samples. The higher expression of CD57 might be from other T-cell lineages.
Conclusion/Recommendations: The NKCs marker expressed were below 50%, these findings indicate a low/ impaired innate immune response, which serve as an explanation to increased breast cancer prevalence and decrease in therapeutic response.
ABSTRACT 11
HIV AND BREAST CANCER - OBSERVATIONAL STUDY OF BREAST CANCER MAMMOGRAPHIC PATTERNS IN HIV POSITIVE AND NEGATIVE PATIENTS
Vanmali A1, Buccimazza I2
1Department of Radiology, University of Kwazulu-Natal
2Department of General Surgery, University of Kwazulu-Natal
Background: Despite extensive research in the field of Human Immune Deficiency Virus /Acquired immune deficiency syndrome (HIV/AIDS), data regarding breast cancer incidence, prognosis, mammographic patterns, histological subtypes as well as the role of screening in this patient population is limited.
Aim: Determine if specific mammographic findings, histological features and patient profiles are unique to a cohort of HIV positive patients who develop breast cancer, by comparing these to an HIV negative cohort.
Materials and methods: Retrospective mammographic analysis of newly diagnosed breast cancer patients referred to the Addington Hospital Breast Clinic between August 2008 and June 2012, was conducted. Comparison of the mammographic features in HIV positive patients to an HIV negative cohort group (38 patients) was performed. Relationship between high-grade ductal carcinoma in situ (HGDCIS), HIV status and clustered and fine pleomorphic microcalcifications were assessed. Chi-square test was utilised. Institutional approval was obtained with BREC (REF: BE013/13).
Results: 38 HIV positive patients were included in the study. 9 of the 38 patients with HIV demonstrated multifocal breast cancer (p-value = 0.007) and 12 of the 38 patients with HIV demonstrated multicentric disease (p-value =0.05). Statistical significance between the presence of clustered microcalcification, fine pleomorphic microcalcification and HIV status noted. Presence of HGDCIS and HIV positive patients and, presence of fine pleomorphic, clustered microcalcification with HGDCIS confirmed biopsies and the HIV status of the patient demonstrated statistical significance. Mean age of HIV positive patients was 42.5 years and the HIV negative group that was 57.6 years (p-value = 0.000).
Conclusion: We demonstrated a statistically significant relationship between HIV status, presence of multifocal breast cancer and presence of clustered and fine pleomorphic micro-calcification. We demonstrated a statistically significant relationship between the presence of HGDCIS and HIV status and presence of clustered and fine pleomorphic microcalcification in HGDCIS confirmed biopsies in HIV positive patients.
ABSTRACT 12
ANTI-PLATELET THERAPY AS AN ADAPTIVE PRESSURE FOR TUMOUR CELL SURVIVAL - AN EX VIVO ANALYSIS
Xulu K1, Duarte R2, Augustine T1
1School of Anatomical Sciences, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg
2Department of Internal Medicine, School of Clinical Medicine; Faculty of Health Sciences, University of the Witwatersrand, Johannesburg
Background: Thromboembolic events are the second leading cause of mortality among breast cancer patients. Co-administration of antiplatelet therapy has been proposed as a treatment strategy against cancer-associated thromboembolic disorders; however, the efficacy of such dual treatment has not been established.
Ethical clearance for the study was obtained (M150263) from the Human Research Ethics Committee, University of the Witwatersrand.
Methods: Using ex vivo cell culture models, we investigated firstly, the direct effects of Aspirin and Clopidogrel cocktail on Anastrozole-treated hormone-dependent breast cancer cell lines (MCF-7/T47D). Secondly, we coupled this study with defining the inflammatory profile resulting from cancer cell exposure to vascular components.
Results: Assays to determine induced cytotoxicity (neutral red, lactate dehydrogenase and annexin V/PI assays) revealed phenotype-dependent ultrastructural alterations that are more suggestive of features associated with promotion of cellular invasion as opposed to cell death. We are currently analysing 13 cytokines to determine whether these results reflect the generation of a pro-inflammatory microenvironment to ensure cell survival as an adaptive mechanism to selective pressures caused by antiplatelet therapy.
Conclusion: At this juncture we recommend further research and caution in the clinical setting as breast cancer sub-phenotypes not clinically identified may respond differentially to dual anti-platelet/hormone-therapy treatment, which while preventing thromboembolic complications may do so at the expense of encouraging cellular survival mechanisms that in turn may potentiate tumour progression.
ABSTRACT 13
COMPLETENESS OF HISTOPATHOLOGICAL REPORTING IN BREAST CANCER: RESULTS FROM FOUR SOUTH AFRICAN BREAST CENTRES
Toma A, Cubasch H, Joffe M, Ayeni O, Nel C, Nietz S
Department of Surgery, University of Witwatersrand
Introduction: Quality pathology reporting forms the cornerstone for the establishment of specialised breast services. Using current EUSOMA standards, we audited the reporting practices of four independent South African academic breast centres.
Materials & methods: We included 1853 consecutive cases of histologically confirmed invasive breast cancer between July 2015 to September 2017. Patients were recruited at two units in Gauteng Province (CHBAH & CMJAH) and two units in KwaZulu Natal (IALCH/Ngwelezana & GH). We compared our available records against EUSOMA quality standards. A histology report would be complete if it included: histological type, grade, ER, PR and HER-2. Equivocal HER-2 cases on IHC required additional FISH testing, Ki67 was optional. Excisional surgical specimen additionally required pathological stage, size of invasive component, peritumoral vascular invasion and distance to nearest radial margin for completeness. EUSOMA require > 95% completeness as a minimum standard but the ideal target is > 98%.
Rsults: For core biopsies, completeness was: 89.9% CHBAH, 91% CMJAH, 43% IALCH and 63.2% GH. Overall completeness for the cohort was 74.7%. Excisional biopsy completeness was 52.2% CHBAH, 61.6% CMJAH, 16.5% IALCH and 29.7% GH. Overall completeness for the cohort was 42%. Grading was absent for 45.7% of Durban patients with 72.2% of the remainder being grade 2. Luminal subtyping based on receptor status showed significant differences between Gauteng and KZN sites with luminal A subtype making 17.6% in Gauteng and 26.2% in KZN. A possible explanation for the poorer performance of excisional specimens could be that receptors were not routinely repeated after 6 months, contrary to EUSOMA standards.
Conclusion: All centres fell short of the required 95% to achieve a clean audit as per EUSOMA standards. CMJAH (91%) and CHBAH (89.9%) were closest to achieving this for the core biopsy specimen. All centres showed inferior report completeness for the surgical specimen. Significant inter-centre differences in tumour grading and intrinsic subtypes require further attention and are unlikely due to biological differences in the source populations.
ABSTRACT 14
CLINICAL BREAST SCREENING OF WOMEN WORKING WITHIN THE CAPE UNION MART GROUP: A PILOT STUDY: INTERIM FINDINGS
Edge J1, Martin L1, Wegelin L1, Dedekind B2
1Stellenbosch University, Faculty of Medicine & Health Sciences, Cape Town
2Christiaan Barnard memorial Hospital, Cape Town
Background: Breast screening is a controversial issue. There are 3 modalities that have been studied, self-examination, clinical breast examination (CBE) and mammographic screening. In South Africa, there is no state-run breast screening programme for women. Mammographic surveillance is available only to some. CBE as a screening modality has been studied with mixed results.
Aim of the study: To offer risk stratified CBE to all women working within the Cape Union Mart group and compare demographic and clinical factors between those with a 10 year risk of breast cancer of <1% (group A) with those with a breast cancer risk >1% (group B).
Methodology: This was a cross-sectional study. All consenting women had their medical history taken and a risk assessment using the IBIS calculator. Eligible women underwent a CBE which was performed by a trained breast nurse. Any woman with a suspicious change in their breast was referred to an appropriate breast clinic for further investigation. HREC: N18/08/086
Results: A total of 171 were included in the study of which 17 (9.9%) women were in group A and 154 (90.1%) in group B. Of those that had a CBE, 14 (82.4%) and 154 (100%) were in groups A and B, respectively. (See Table 1)
Conclusion: The IBIS risk calculator can be used in conjunction with a clinical breast screening programme
ABSTRACT 15
PATIENT AND TUMOUR FACTORS AFFECTING THE HISTOLOGY OF SENTINEL LYMPH NODES BIOPSY IN BREAST CANCER AT UNIVERSITAS ACADEMIC HOSPITAL, BLOEMFONTEIN
Letsoara S, Pearce N
Department of General Surgery, University of Free State
Introduction/Background: Sentinel lymph node biopsy is an accepted management in clinically node negative breast cancer patients (T1-T3) for deciding whether axillae dissection should be done or not.
Aim(s): Primary aim was to determine factors affecting histology of sentinel lymph node biopsy. Secondary was to determine the histological characteristics of the sentinel lymph node and final histological status of the axilla if sentinel lymph node was positive.
Methods: Retrospective analytical study of patients who underwent mastectomy or lumpectomy with sentinel lymph nodes biopsy between 2007 to 2016 (n = 60). Males and ductal carcinoma in-situ patients were excluded.
* Ethical considerations: HSREC 31/2017(UFS- HSD2017/0183)
Results:
Demographics: Age ranged from 36 to 90 years and its association with sentinel lymph node histology was statistically significant ( p-value 0.0242). Race and pre-op chemotherapy did not have statistically significant association with sentinel lymph node histology ( p-value 0.7935 and 1.000).
Tumour factors: Location of the tumour, type of tumour, size of tumour all with p-value of 1.000, histological type (p-value 0.7464), grade (p-value 0.6244), lymph vascular infiltration (p-value 1.000) and hormone receptors (ER-positive p value 0.6434, PR-positive p-value 0.7290, HER-positive p-value 0.2341 and ER/PR/HER-positive p value 1.000) did not have statistically significant association with sentinel lymph node histology. Sentinel lymph node biopsy histology was reported as either positive or negative. There was a statistically significant association between histology of sentinel lymph node biopsy and other nodes in the axilla (p-value < 0.001).
Conclusion/Recommendations: The study did not prove our hypothesis that- tumour size, site, grade, and lymph vascular infiltration will affect histology of sentinel lymph node as was also found with receptors studies. Age affected histology of sentinel lymph node biopsy- which we did not predict. Sample size and inadequate lymph vascular infiltration reporting might have affected results. Histology of sentinel lymph node biopsy predicted histology of the axilla.
ABSTRACT 16
A RETROSPECTIVE STUDY OF 16 PATIENTS WITH SARCOMAS OR PHYLLODES TUMOURS (BORDERLINE OR MALIGNANT) OF THE BREAST AND A COMPARISON WITH PATIENTS WITH BREAST CARCINOMA.
Lindqvist E1, de Jager L2, Baatjes K2, Conradie W2, Burger H2, Edge J2
1Karolinska Institute, Stockholm;
2Stellenbosch University, Faculty of Medicine & Health Sciences, Cape Town
Introduction/Background: Sarcomas and malignant or borderline phyllodes tumours (SPT) of the breast have high local recurrence rates and the prognosis is often poor.
Aim(s): Our aim in this study was to compare the pathological characteristics of patients with SPT of the breast seen at Tygerberg Hospital (TBH) with those presenting with breast carcinoma.
Methods: We performed a retrospective cohort study including all patients with newly diagnosed SPT of the breast discussed at the TBH breast and sarcoma combined clinic in the last four years, (1/1/2015 to 31/12/2018). Patients were identified using the National Health Laboratory Services (NHLS) information system. Breast carcinoma patients were taken from a retrospective database and the first 50 new breast carcinoma patients seen in 2018 were used as a comparative group. Patient demographics and tumour characteristics were captured through the NHLS, the Picture Archiving and Communication System, and the TBH Enterprise Content Management electronic record systems.
Results: Sixteen patients with SPT were identified. All patients in both cohorts were female. Not all patients in either group had an HIV test, FNA or core biopsy.
See Table.
Conclusion/Recommendations: When compared to women with breast cancer, patients with SPT were significantly younger and had larger tumours. Cytology was not useful in diagnosing SPT.
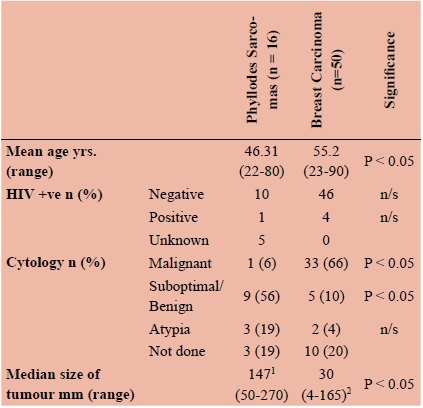
1. Pathological measurement of tumour size
2. Radiological measurement of tumour size: US or CT scan when tumour too big for US
ABSTRACT 17
IDIOPATHIC GRANULOMATOUS MASTITIS IN A SINGLE CENTRE BREAST UNIT IN DURBAN, SOUTH AFRICA
Hariparsad SD, Buccimazza I
Breast, Endocrine, Soft Tissue Unit, Specialized Surgical Services, Inhosi Albert Luthuli Central Hospital, University of KZN
Background: Idiopathic lobular granulomatous mastitis (ILGM) is a rare chronic inflammatory of the breast. The clinical and radiologic presentation is similar to that of breast carcinoma and is reported to occur in young parous females. Diagnosis and treatment can be challenging.
Aims: This retrospective chart review aims to document our local experience with this condition.
Methods: Data regarding eight patients who were treated for ILGM over from 2012 to 2019 were analysed from a public hospital single centre breast unit in Durban, South Africa. All files of patients treated with granulomatous mastitis were reviewed. Only patients with confirmed features of non-necrotizing granulomatous inflammation of the breast were included for analysis. Demographic, clinical presentation, investigative and treatment data was captured and analysed.
Results: All eight patients presented with a breast lump while three presented with mastalgia, and one presented with a nipple discharge. Five patients had left sided disease, one patient had bilateral disease, and two had right sided disease. The duration for symptoms at presentation ranged from 2-10 months. Seven patients were pre-menopausal, and only two were on oral contraception (OC) at the time of presentation. Four patients had mammograms, with one patient having a focal opacity, one having an asymmetrical density, and two having no focal mass, but increased density of the breast. Seven patients had radiologist reported ultrasounds where both heterogenous and hypoechoic lesions were noted as well as architectural distortion with varying overlap of findings. All patients were treated with steroids until resolution. The mean treatment duration was 6.4 months. One patient had two episodes of recurrence that were treated with methotrexate.
Conclusions: ILGM is a rare breast condition that presents a diagnostic and treatment challenge. Appropriate investigation and histopathological assessment are paramount to avoid unnecessary surgery and to ensure good treatment outcomes.
ABSTRACT 18
ILEOSIGMOID KNOT: KALAFONG ACADEMIC HOSPITAL EXPERIENCE
Jaffer T, Montwedi D
Department of Surgery, Kalafong Academic Hospital, University of Pretoria
Background: Ileosigmoid knotting (ISK), or double volvulus, is a rare cause of intestinal obstruction with rapid deterioration in the patients' clinical condition resulting in fatal consequences.
Aim: Improve clinical knowledge of ISK in a local setting allowing earlier recognition and improved management.
Method: A 7 year retrospective review (January 2011-January 2018) of patients presenting with ISK at Kalafong Academic Hospital (KAH) was conducted. We evaluated our local patient populations' clinical, biochemical and radiological signs, intra-operative and post-operative outcomes.
Results: Ten ileosigmoid knot patients presented to KAH over the study period; average age was 44,2 years old with a 100 percent male predominance. One patient died perioperatively and one was HIV positive. Ninety percent of patients had no previous surgical history. 80 percent had deranged kidney function on admission. All patients presented with signs of peritonitis, while 80 percent had abdominal distention. On plain abdominal radiographs, 90 percent had large bowel obstruction features and 70 percent had small bowel obstruction features. 70 percent had no air in the rectum and 50 percent had a coffee bean sign. Forty percent had ileocaecal valve involvement with a Hartman's procedure performed in 70 percent of patients and primary anastomoses performed in 20 percent of patients. Fifty percent of patients developed a superficial surgical site infection. Average length of stay was 15,4 days.
Conclusion: Ileosigmoid knots should be considered as a cause of bowel obstruction in male patients regardless of a history of previous abdominal surgeries. Radiological features suggestive of small and large bowel obstruction should alert the surgeon of ISK being a possible cause. Surgical management is almost always required but being aware of ISK as a cause can allow the surgeon to prepare and manage the patient more effectively.
ABSTRACT 19
MANAGEMENT OF RECTAL CANCER. A SINGLE CENTRE STUDY
Moodley K1, Naidoo MM2, Madiba TE1,3
Department of Surgery, Nelson R. Mandela School of Medicine, College of Health Sciences University of KwaZulu-Natal
2Department of General Surgery, Addington Hospital, Durban, KwaZulu-Natal
3Gastrointestinal Cancer Research Centre, University of KwaZulu-Natal, Durban, South Africa
Introduction: There is paucity of literature regarding surgical management of rectal cancer in South Africa.
Purpose: To document management and outcome of rectal cancer in our setting.
Study setting Durban Colorectal Unit situated in a tertiary referral Hospital.
Study population: Patients with rectal cancer were extracted from the Colorectal Cancer Database.
Study design: This was a retrospective analysis of prospectively collected data collected from the database. The data documented included demographics, clinical presentation, disease stage, management, outcome and follow-up. UKZN (Ref.BE259/16)
Results: A total of 1944 patients were seen of whom 1043 had rectal cancer (563 and 480 females. Mean age was 58 (+ 14.55) years and 150 patients (14.38%) were < 40 years old. Tumour-related complications occurred in 147 patients (14.09%) namely obstruction (125), perforation (7) and fistula (15). A total of 289 patients (30.81%) received neo-adjuvant therapy, 208 (22.17%) received adjuvant therapy and 245 (26.12%) received palliative therapy while 1 patient (0.11%) received both neoadjuvant and adjuvant therapy. Five hundred and fourteen patients (49.28%) underwent resection, namely abdominoperineal resection (235) and anterior resection (262). Open surgery was performed in 421 and 81 underwent laparoscopic surgery. Patients presented with stage I (9.11%), stage II (17.83%), stage III (18.22%) and stage IV (26.85%). Five hundred and seventy patients (54.65%) are known to have demised, 211 (20.23%). Patients have been followed up for 18.92 (+ 24.26) months. Recurrence was documented in 74 (7.09%) patients with a mean disease-free interval was 27.33 months. Limitations included patients lost to follow up and missing data.
Conclusion: Rectal cancer was seen in all population groups. Age of presentation was lower than international literature and there was a slight male preponderance. Metastatic disease was seen in 9.97% Resection rate was 49.28%. Open surgery predominated in our series.
ABSTRACT 20
THE MANAGEMENT OF RECTOVAGINAL FISTULA. THE DURBAN EXPERIENCE
Sibiya SR 1, Ramphal S2, Madiba TE1
Departments of Surgery, University of KwaZulu-Natal, Durban 2Obstetrics & Gynaecology, University of KwaZulu-Natal, Durban
Background: The aetiology of Rectovaginal fistula (RVF) is multifactorial and the condition is bothersome to both the patient and the surgeon due to their irritating and embarrassing symptoms and high failure rate after repair.
Aim: To document the management and outcomes of RVF in the Durban Colorectal Unit
Study setting: Colorectal Unit at Inkosi Albert Luthuli Central Hospital, a tertiary referral hospital
Study population: All patients with rectovaginal fistula treated at the colorectal unit.
Methods: Retrospective analysis of the management of all patients with RVF. The data were extracted from the RVF database between 2006 and 2018 and analysed. Data collected included demographics, aetiology, management and outcome. UKZN (Ref No:BE297//18 sub-study of BE231/13)
Results: There were 43 patients accrued over the study period. The median age at presentation was 36 years (IQR 28-42).The HIV status was positive (28), negative (4) and unknown (11) . The causes were obstetric (15), spontaneous (9) secondary to abscess (9), previous surgery (4), perineal sepsis (2) and radiation (2). Spontaneous aetiology was seen in HIV positive (8) and diabetic (1) patients. There was additional anorectal fistula (4) and anal sphincter weakness (7). The median duration of RVF symptoms before referral was 4.5 months. The fistula was above (35), below (2), or through the sphincter (6). A prior diverting colostomy was created in 26 patients. Thirty-seven patients underwent 47 surgical procedures (including 10 redo's).After repair the initial success rate was 72.2% and the final success rate was 97%. 2/6 fistulae healed after conservative management.
Conclusion: Obstetric injury was the leading cause of RVF. HIV positive patients were in the majority. Spontaneous fistulae were seen in immunocompromised patients. Initial success rate was 72.2% and final success rate was 97% over a healing time 3 months.
ABSTRACT 21
DESCRIBING ACUTE PRESENTATIONS OF NON HPV-ASSOCIATED PERIANAL CONDITIONS ON HIV POSITIVE AND NEGATIVE PATIENTS AT PRINCESS MARINA HOSPITAL
Motsumi MJ1, Tlhakanelo JT2
1Department of Surgery, Faculty of Medicine, University of Botswana
2Department of Family Medicine and Public Health, Faculty of Medicine, University of Botswana
Introduction: A lot has been written about the Human papilloma virus (HPV) - associated perianal conditions but there is little about non-HPV associated perianal conditions in relation to the patients' HIV status.
Aim: To describe the diagnoses and presentations of non HPV-associated perianal conditions in HIV positive and negative patients presenting acutely at PMH.
Methods: A one-year (January -December 2017) retrospective study conducted at Princess Marina Hospital, Gaborone. Ethical clearance was granted by the University of Botswana, Ministry of Health and Princess Marina Hospital. Data was collected from the Accident and Emergency department triage forms and medical records into a password protected Access database.
Results: One hundred and fourteen (114) patient files were reviewed. Sixty-six (66) were male and forty-four (44) were female. The mean age was 35.0 years (SD = 11.9). Of the 114 patients 68 were HIV negative, 40 were positive and 6 had unknown HIV status. All of the HIV positive patients were on highly active antiretroviral therapy. The commonest diagnosis was haemorrhoids accounting for 56.1% (64/114) followed by perianal abscess & fistulae in ano at 36.0% (41/114). In the HIV positive group, the infectious perianal conditions occurred in patients with a relatively lower mean CD4 count. Abscesses & fistulae in ano are more common in HIV positive patients while haemorrhoids and anal fissures are common in HIV negative patients. The above-mentioned association was found to be statistically significant (p<0.001).
Conclusion: The commonest non HPV-associated perianal condition presenting at PMH is haemorrhoids followed by perianal abscess & fistula in ano. HIV positive patients tend to develop perianal abscesses & fistulae in ano while HIV negative patients tend to develop haemorrhoids and anal fissures. HIV positive patients who present with infectious pathologies tend to have a relatively lower CD4 count
ABSTRACT 22
THE ROLE OF CARCINOEMBRYONIC ANTIGEN IN PREDICTING COLORECTAL CANCER IN RESOURCE POOR SETTING OF KWAZULU-NATAL, SOUTH AFRICA
Naicker YD, Moolla Z, Madiba TE
Department of Surgery, School of Clinical Medicine, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
Background: Colorectal cancer (CRC) is the fourth most common malignancy in South Africa. Currently the most reliable screening tool, colonoscopy, lacks compliance and access in resource deprived settings of KwaZulu-Natal.
Aim: The aim of this study was to determine whether serum CEA levels in patients symptomatic for lower GI pathology correlates with the histological presence and severity of primary colorectal cancer in a large referral centre within KwaZulu-Natal. Perhaps CEA may have a larger role as a risk indicator for CRC development in these resource deprived communities.
Methods: This study was a retrospective analysis of prospectively collected clinical data of 380 patients with colorectal cancer attending a tertiary referral centre. Patients were of various age groups, various population groups and both genders. Serum levels of CEA were analysed and stratified into < 5μg/l and > 5μg/l. Data were analysed using descriptive statistics. Ethical Approval by Biomedical Research Ethics, UKZN (Ref: BE016/17).
Results: The mean CEA level of the study population was 170.0 ± 623.3 μg/l. The majority (229; 60.26%) had a CEA level > 5μg/l and 151 (39.74%) had a CEA level < 5μg/l. There was no significant correlation between CEA levels and gender (p=0.8) or age (p=0.6). CEA levels were highest in the Black race group. Pairwise comparison demonstrated a statistically significant difference between the Black and Indian population groups (p=0.02). The current study demonstrates an upregulation of CEA as the stage of CRC progresses (p<0.0001).
Conclusion: There was no significant difference in CEA levels across age or gender. A positive correlation was noted between CEA level and stage of CRC. CEA levels were highest in the black race group. Low sensitivity of CEA as a screening test for CRC was confirmed.
ABSTRACT 23
INFANTILE HYPERTROPHIC PYLORIC STENOSIS: PROFILE, MANAGEMENT AND OUTCOME OF PATIENTS ADMITTED TO A TERTIARY HOSPITAL IN BLOEMFONTEIN, SOUTH AFRICA
Arnold R1, Khokho K1, Narrainsamy K1, Brits E2, Joubert G3
1Undergraduate medical student, School of Medicine, Faculty of Health Sciences, UFS, Bloemfontein, RSA
2Department of Surgery, Faculty of Health Sciences, UFS, Bloemfontein, RSA
3Department of Biostatistics, Faculty of Health Sciences, UFS, Bloemfontein, RSA
Introduction/Background: Infantile hypertrophic pyloric stenosis (IHPS) is the thickening of both muscle layers of the pylorus and is most commonly found in first-born males. It usually presents with projectile, non-bilious vomiting. Late presentation leads to severe dehydration and malnutrition with deranged serum-electrolytes and acid-base imbalance delaying treatment and prolonging hospital stay
Aim(s): To evaluate the profile, management and outcome of IHPS at a tertiary hospital in Bloemfontein, South Africa.
Methods: The study was a retrospective, descriptive record review including all patients with IHPS admitted to Universitas Hospital from January 2008 to February 2016. Of the 22 patients admitted, files for 19 patients were available for inclusion.
Results: Sixteen (84.2%) of the 19 patients were male. Out of those with available birth order (n = 11), two were first-, two second-, six third- and one fourth-born. The patient' ages ranged from 27-194 days (median 51 days). The most common symptoms were projectile vomiting (78.9%) and poor weight gain (68.4%). Six patients had no ultrasound done and 17 patients underwent a Ramstedt-pyloromyotomy. Eight patients received atropine as part of their initial management. The duration of symptoms ranged from 1-58 days (median 14 days). There was no reported mortality. The length of stay ranged between 2-60 days (median 7 days).
Conclusion: The gender distribution and age at presentation were in keeping with the literature, but not the birth order. The delay before surgery emphasises the poor general condition and deranged biochemical state the patients present at the hospital
ABSTRACT 24
DELAYED REPAIR OF UNCOMPLICATED INGUINAL HERNIAS IN INFANTS IS SAFE: A 6 YEAR AUDIT, 2010-2015, AT THE TYGERBERG CHILDREN'S HOSPITAL.
Botes SN1, Edge J1, Apffelstaedt JP2, Sidler D3
1ivision of General Surgery, Stellenbosch University, Cape Town, South Africa
2Panaroma, Private Practice, Cape Town,
3Division of Paediatric surgery, Tygerberg Children's Hospital, University of Stellenbosch
Introduction/Background: Incarceration with potential strangulation and bowel necrosis of infant inguinal hernias is the main indication for urgent repair. Lack of theatre time delays inguinal hernia repair, resulting in prolonged hospitalization. To offset this prolonged, often unnecessary in hospital management, infants are discharged to be operated on an elective list. The concern with delaying the repair, is the risk of incarceration.
Aim(s): We report a series of patients with uncomplicated hernias who were discharged home to have their elective surgery at a later stage (mean 8.78 weeks) and assessed the safety of this approach.
Methods: After ethical approval (HREC nr S16/10/218), A retrospective audit was performed of all infants with an inguinal hernia from Jan 2010 to June 2015. Incomplete records and infants operated after their first birthday were excluded. Two groups were identified; immediate surgery for infants with uncomplicated hernias, and delayed surgery for infants with uncomplicated hernias. Incarceration/ strangulation rates in the interim period were documented for the delayed group, and comparison made between the groups regarding perioperative and anaesthetic complications. Length of hospital stay post-operatively was also documented.
Results: The incarceration rate after being discharged home was 4.1%. There was, however, no significant difference in the peri-operative complications between the two groups, including in the incarcerated hernia group. Length of hospital stay post- operatively was similar.
Conclusion/Recommendations: Delayed repair, up to 2 months later, for uncomplicated infant hernia is safe.
ABSTRACT 25
COMPLICATIONS IN THE PLACEMENT OF CENTRAL LINES FOR PAEDIATRIC ONCOLOGYPATIENTS AT UNIVERSITAS ACADEMIC HOSPITAL, FROM 1992 TO MARCH 2018.
Magooa K1, Mohone L1, Ndovo P1, Rampeta P1, Tsilo K1, Brits E2, Joubert G3
1Undergraduate medical student, School of Medicine, Faculty of Health Sciences, UFS, Bloemfontein, RSA
2Department of Surgery, Faculty of Health Sciences, UFS, Bloemfontein, RSA
3Department of Biostatistics, Faculty of Health Sciences, UFS, Bloemfontein, RSA
Introduction/Background: Central venous access devices (CVADs) such as External tunnelled cuffed catheters (Hickman Lines) are notoriously associated with complications such as central line associated infections and more severely, systemic sepsis.
Aim: To determine the complications of central lines for chemotherapy in paediatric oncology patients treated by the Paediatric, Haematology and Oncology Unit at Universitas Academic Hospital in Bloemfontein from 1992 to March 2018.
Methods: This was a retrospective descriptive study. The study population was paediatric oncology patients, 16 years and younger, that received CVAD's and treated by Paediatric Haematology and Oncology Unit at Universitas Academic Hospital in Bloemfontein. Information was collected from the Paediatric Haematology and Oncology database.
Results: There were 293 lines inserted with a median age of 64.7 months. There were no in-situ local complications in 183(62.5%) of the lines while 39(13.3 %) showed line sepsis which was the most common complication. Of the 39 lines that had line sepsis, 23% had no systemic sepsis and 61.5% were neutropenic and septic. In 190 lines the patients had symptoms of systemic sepsis and accompanying neutropenia. Of these 190 lines, 128(67.4%) did not develop in-situ line complications. 85(44.7%) lines were removed because it was the end of treatment and only 31(16.3%) lines were removed as a result of line sepsis.
Conclusion: Despite the study population having characteristics that make them more prone to infections, there was a significantly low incidence of line sepsis (13.3%). The special care taken intra-operatively and the meticulous aseptic handling and maintenance post-operatively can be the reason for the low infective complication values.
ABSTRACT 26
THE PROFILE AND OUTCOME OF SMALL BOWEL ATRESIA AT UNIVERSITAS ACADEMIC HOSPITAL
du Preez H, Brits E
Division of Paediatric Surgery, Department of General Surgery, University of the Free State
Introduction/Background: Universitas Academic Hospital is located and drains the entire central South Africa. Associated congenital anomalies and prematurity are the main predictors of mortality in first world countries. In third world countries, late referrals and lack of resources, contribute to mortality
Aim: To objectively describe the outcome of small bowel atresia at our institution.
Methods: A retrospective descriptive study was done. Patient sample included all neonates admitted with small bowel atresia from 1 January 2010- 31 October 2016. We analysed patient information and recorded data including birth demographics, status on arrival, in hospital stay and outcomes.
♣ thical approval: HSREC 184/2016(UFS-HSD2016/1491)
Results: Our study sample was 92 patients. Median gestation was 34 weeks. Average birthweight was 2,2kg. The majority were born in the Free State (69.6%). Only 7 patients were diagnosed antenatally and only 13 (14,1%) were born in a tertiary institution. The commonest associated congenital anomaly was a cardiac lesion. (43,5%) Late referrals were common, with 67(72,8%) arriving after 48 hours of birth, 56 (60,8%) arrived dehydrated and 51 (55,4%) arrived septic. The median age at surgery was 7,5 days after being admitted for a median time of 2 days. The median age full feeds were reached was 18 days and 26 (28,6%) had a feeding intolerance. The median number of septic episodes were 2 per patient. Median length of stay was 28 days. We had a low mortality rate, 8 (8,7%) were palliated and 10 (10,9%) demised. Mortality was strongly associated with prematurity.
Conclusion: Despite the majority of patients being referred late, our mortality was comparable to first world countries. We were able to overcome this burden due to access to resources, sophisticated equipment and a low surgical complication rate.
Length of stay could be decreased with a feeding protocol and discharge goals.
ABSTRACT 27
RESECTION OF HEPATOCELLULAR CARCINOMA. A PERIOPERATIVE OUTCOMES ANALYSIS
Obery G, Krige JEJ, Jonas EG, Bernon M, Burmeister S, Kotze UK, Kloppers C
Department of Surgery, University of Cape Town Health Sciences Faculty and Surgical Gastroenterology and HPB Units, Groote Schuur Hospital, Cape Town, South Africa
Background: Hepatocellular carcinoma (HCC) is a leading cause of cancer in Africa. Liver resection (LR), local tumour ablation and liver transplantation are the only curative treatment options in selected patients. Major liver resections can have significant morbidity and mortality rates.
Objectives: This study evaluated perioperative outcome in patients with HCC who underwent LR.
Methods: All patients with HCC treated with resection from 1990-2018 were identified from a prospective departmental database. Demographic data, operative management including number of liver segments resected and post-operative morbidity and mortality using the Accordion classification were analysed.
Results: Forty-three patients (25 men, 18 women, median age 47.5 years, range 18 - 79) underwent LR. Seven patients had an HCC and underlying cirrhosis, 10 had fibrolamellar HCC and 26 had an HCC occurring in a non-cirrhotic liver. Number of segments resected ranged from 1 - 5 (median n=4, range 1 - 5). Ten patients had a minor resection (< 3 segments), and 33 underwent major resections (3 segments n=6, 4 segs n=23, 5 segs n=4). Median operating time was 240 minutes (range 120 - 570). Median intra-operative blood loss was 750 ml (range 80 - 2500) and 13 patients received an intra-operative blood transfusion (range 375 - 1500 ml). Median total inflow ischaemic time during liver parenchymal transection was 35 minutes (range 0 - 117). Median postoperative hospital stay was 8 days (range 5 - 24) and median ICU stay of 2 days (range 0 - 6). Twelve patients (28%) had 15 postoperative complications. Accordion grades in these 12 patients were grade 1 n=8, grade 2 n=2, grade 3 n=1, grade 4 n=1. There was no perioperative mortality.
Conclusion: This study shows that with the application of modern liver resection techniques in specialised HPB surgical units, major liver resections can be performed safely in carefully selected patients with minimal morbidity and no mortality.
ABSTRACT 28
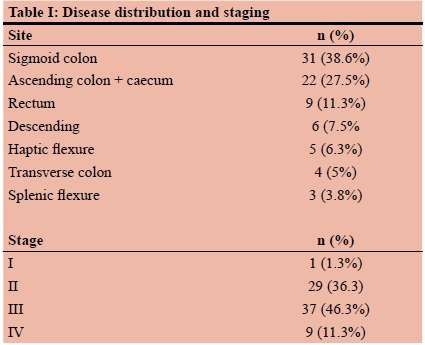
CLINICOPATHOLOGICAL AUDIT OF BOWEL PERFORATION IN PATIENTS WITH COLORECTAL CANCER
Norman J, Madiba TE
Department of Surgery, University of KwaZulu-Natal, Durban
Introduction: Colorectal cancer is the second leading cause of cancer-related mortality in the world. The risk of mortality increases with perforation. However, literature on malignant perforation is lacking in the African setting.
Purpose: The purpose of this study was to present the clinicopathological audit of patients presenting with perforated colorectal cancer.
Methods:
Study setting: Colorectal Unit situated at Inkosi Albert Luthuli Central Hospital, Durban.
Study population: Patients presenting with perforated colorectal cancer at the Colorectal Unit. Data were extracted from the colorectal cancer database.
Study design: This is a retrospective analysis of prospectively collected data. Data analysed spanned 19 years (2000-2018). Data analysed included demographics, clinical presentation, staging, management and outcome.
Ethical Approval: Biomedical Research Ethics Committee, UKZN (Ref.: E198/04)
Results: Eighty out of 2220 patients with colorectal cancer had bowel perforation (4%). Median age was 52.5 years and M:F ratio was 1:1.2. Eighteen patients (47.5%) were < 40 years old. The perforation was either contained (75) or free (5). Site distribution and staging are shown in Table I. Resection rate was 97.5% with disease recurrence in 16.7%. Median follow-up was 9 months. Thirty-two patients are known to have died with a median survival of 4 months.
Conclusion: Malignant perforation occurred in 4% of patients with colorectal cancer. Contained perforation predominated. Young patients were relatively more common. The most common site was the sigmoid colon followed by ascending colon. There was a high resection rate (97%) and recurrent disease occurred in 17%. Median survival was 4 months.
ABSTRACT 29
A REVIEW OF GERIATRIC INJURIES AT A MAJOR TRAUMA CENTER IN SOUTH AFRICA
Da Costa JP1, Laing J2, Kong VY1,2, Bruce JL2, Laing G2, Clarke DL1,2
1Department of Surgery, University of the Witwatersrand, Johannesburg
2Department of Surgery, University of Kwa Zulu-Natal, Durban, South Africa
Introduction: Trauma in South Africa has been referred to as a malignant epidemic but the impact of trauma on the elderly has often been overlooked. This paper sets out to address this.
Methods: This study was based in Grey's Hospital, Pietermaritzburg, South Africa. Patients over the age of sixty-five years admitted following trauma between December 2012 and December 2018 were reviewed. Ethics approval was granted by the Biomedical Research Ethics Committee of UKZN (#: BCA 207/09 and BCA 221/13).
Results: Over the five years, 281 patients met our inclusion criteria. There were 150 males (53.38%) and 97 females (34.5%). On average, participants were 72 years old (range: 65-97). There were 211 (75.09%) instances of blunt trauma, 41 (14.59%) cases of penetrating trauma and 14 (4.98%) cases of other types of trauma. The most common forms of blunt trauma were accidental falls (76), motor-vehicle accidents (46) and pedestrian-vehicle accidents (31). Penetrating trauma was most commonly gunshot (22) and knife wounds (14). Other trauma was predominantly dog (6) and snake (6) bites. There were 72 incidents of assault (25.26%). Assaults were generally committed by a single perpetrator who was frequently known to the victim. No significant differences in the proportion of injuries between males and females was noted. 44 patients (15.66%) required surgical intervention with respiratory, renal and cardiac complications being seen most frequently. Seventeen patients required ICU admission with 5 requiring ventilation. Ultimately, 241 (85.77%) patients survived; 32 (11.39%) died and 8 (2.85%) had an unknown outcome.
Conclusion: Geriatric trauma in South Africa is relatively rare but will increase as the population ages. There is a high incidence of assault as a mechanism and this highlights that the elderly is a vulnerable group. Managing these patients is challenging and is associated with significant morbidity and mortality rates.
ABSTRACT 30
THE SPECTRUM OF ANIMAL RELATED INJURIES MANAGED AT A MAJOR TRAUMA CENTRE IN SOUTH AFRICA
Wessels EU1, Kong VY1,2, Buitendag J3, Moffatt S4, Weale R5, Ras AB2, Ras M2, Smith MTD2, Laing GL2, Bruce JL2, Bekker W2, Manchev V2, ClarkeD1, 2
1Department of Surgery, University of the Witwatersrand, Johannesburg, South Africa
2Department of Surgery, University of KwaZulu Natal, Durban, South Africa
3Department of Surgery, Tygerberg Hospital, Stellenbosch University, Cape Town, South Africa
4Department of Surgery, University Hospitals Coventry and Warwickshire NHS Trust, Coventry, United Kingdom
5Department of Surgery, North West Deanery, Manchester, United Kingdom
Introduction: Humans come into contact and interact with an array of animals in a number of areas and environments. We set out to review our experience with animal-related injuries in Pietermaritzburg, KwaZulu Natal, South Africa.
Methods: All patients who sustained an injury secondary to an interaction with an animal in the period December 2012-December 2017 were identified from the Hybrid Electronic Medical Registry.
Results: There were 104 patients (75% male). The mean age in the study was 32.8 years (range 1 to 76). From 104 animal-related injuries, 67 were blunt trauma, 39 penetrating trauma and 3 a combination of the 2. The species causing trauma included dogs (53), horses (29), cows (18) and one each of the following: buffalo, warthog, impala and goat. The median time from injury to hospitalisation was 46.62 hours (range 0 to 504). Injuries occurred to the head (32), face (9), neck (32), abdomen (22), urogenital system (6), upper limb (39) and lower limb (39). The Injury Severity Score mean for the patients was 8.16. In 49 patients the treatment was non-operative. In the remaining 55 patients, a total of 68 operative procedures were required. Operations included wound debridement/surgical washout (38), laparotomy (9), arterial repair/ligation (8), skin graft (4), craniotomy (5), fasciotomy (2), amputation (1), and placement of an ICP monitor (1). 49 of these operations were for patients with dog bite injuries. The mean hospital stay was 0.13 days (range of 0-4). Four patients were admitted to the Intensive Care Unit and two patients died.
Conclusion: Human interactions with animals may result in injuries which require surgical treatment. The most common animal injury is a dog bite but in the case of the larger domestic farm animals, blunt force type injuries and goring can result in significant injuries which require complex surgical interventions.
ABSTRACT 31
TRAUMA IN PREGNANCY REVISITED
Moffatt S1, Kong V2, Goldberg B3, Clarke D4
1Department of Surgery, Grey's hospital
2 Department of Surgery, University of Kwa Zulu-Natal
3Department of Surgery, University of the Witwatersrand
4Department of surgery, Grey's Hospital
Introduction: Much has been written about trauma in South Africa, but certain vulnerable groups remain under-researched. This paper revisits our institution's experience with trauma in pregnancy and aims to look at.
Methods: All pregnant patients who were admitted to the Pietermaritzburg Metropolitan Trauma Service (PMTS) following trauma between December 2012 and December 2018 were identified from the Hybrid Electronic Medical Registry (HEMR). Basic demographic and physiological data were documented along with the mechanism and the severity of the injury as well as fetal outcomes and patient management.
Results: During the six-year study period, 2990 female patients were admitted by the PMTS in total, 90 of whom were pregnant. The mean age was 25.64 years with a range of 17 to 43 years. The mechanism of injury included motor vehicle accident (MVA) 25, stab wounds (SW) 19, assault other than SW or gunshot wounds (GSW) 19, pedestrian vehicle accident (PVA) 11, GSW 8, snake bite 5, fall from vehicle 3, impalement 1, dog bite 1, hanging 1, sexual assault 1, iatrogenic injury 1 and being hit by a falling object 1. A subset of patients sustained more than a single mechanism. A total of 30 patients were managed operatively. The mean time of gestation was 19.16 weeks (range 5-36). 3 patients died. There were 16 fetal deaths (including 3 lost following the mother's death). 45 foetuses were recorded as surviving at the point of discharge. 25 fetal outcomes were not specifically recorded. There were 2 threatened miscarriages/vaginal bleeds, 1 ectopic pregnancy and 1 positive pregnancy test with no recorded outcome. There were no premature births due to trauma.
Conclusion: Common broad mechanisms of injury involved assault of some form or road accidents (MVA/PVA). Trauma in pregnancy is challenging to manage. The mother must take priority over any other considerations.
ABSTRACT 32
EVALUATION OF MONOCYTE/MACROPHAGE PROFILE IN BREAST CANCER PATIENTS AT STEVE BIKO TERTIARY HOSPITALS
Jaffer T1, SetlaiP1, MokoenaT1, Durandt C3
1Department of Surgery, University of Pretoria 2Department of Immunology, University of Pretoria
Introduction/Background: Breast cancer (BC) is the most frequently diagnosed female cancer in Sub-saharan Africa. Monocytes (Mo) are precursors of macrophages (M<|)). Monocytes are recruited into the tumour microenviroment where they differentiate into tumour associated macrophages (TAMs). Macrophages are classified into M1 M<|) which are anti-tumour whilst M2 M<|), also referred to as TAMs, are pro-tumour thus favour cancer progression/metastasis. High frequency of TAMs is associated with poor clinical prognosis in Breast Cancer (BC) patients. Both Mo/M<|) populations are viral reservoirs and transport vehicles throughout the life cycle of human immunodeficiency virus (HIV).
Aim(s): This study evaluated Monocyte/Macrophage profiles in HIV+ and HIV- BC patients undergoing surgical therapy.
Methods: Peripheral blood mononuclear cells (98% purity) from 16 HIV- and 5 HIV + BC patients were analysed pre-operatively, 24hrs & 1week post-operatively, University of Pretoria ethical approval number 498-2017. Flow cytometry markers anti-CD80/CD284 antibodies (M1 Mɸ)), anti-CD163/ CD206 (M2 Mɸ) and anti CD16/CD14 antibodies (Mo) were used.
Results:
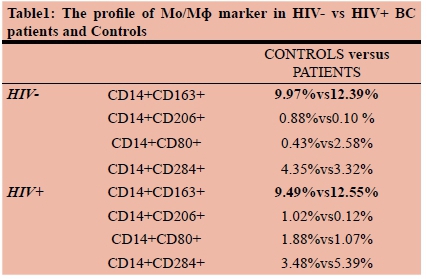
CD14+CD16+ levels 24hours to 1week post-op were 9.11 and 23.79% respectively in HIV+ BC patients and 7.3 and 7.98% in negative patients.
Conclusion/Recommendations: A slight increase in CD14+/ CD163+ levels in BC patients than controls were observed. Increased M2 markers have been reported in BC patients in literature, however our results will be validated by ongoing follow-up studies. This includes failure of CD14+CD16+ levels to return to base one-week post-Op in HIV+ BC patients.
ABSTRACT 33
BACTERIOLOGY AND RESISTANCE IN APPENDICITIS AT DR GEORGE MUKHARI ACADEMIC HOSPITAL
Mosasi TC1, Koto MZ1, Shikwambane-Ntlemo G2
1Department of General Surgery; SMU
2Department of Microbiology, SMU
Background and objectives: To prevent septicaemia and surgical site infections after appendectomy, antibiotics are recommended in acute appendicitis. The objective of this study was to evaluate the bacteriology and resistance in both complicated and uncomplicated appendicitis in order to guide and help with the correct way to use antibiotics and preventing resistance.
Methods: Data of patients who presented between 01 July 2018 and 31 March 2019 to Dr George Mukhari Hospital with acute appendicitis was collected. There were 118 patients with acute appendicitis. The microbiology reports of all the specimen that were sent for analysis were obtained. The reports were analysed, looking particularly for the organisms cultured as well as their sensitivity and resistance.
Results: Bacteria were isolated from 102 of 118 specimen (86%). The most common organism was E.coli, which was present in 75 of 102 (73%) patients with acute appendicitis. Less frequent organisms were Klebsiella pneumonia (40 cases; 39%), Streptococcus spp. (32 cases; 31%), Enterococcus spp. (19 cases; 18%), and Pseudomonas aeruginosa (12 cases; 11%). E.coli was mostly sensitive to amoxicillin-clavulanic acid, ampicillin/amoxicillin, ciprofloxacin, cefuroxime and gentamycin. Sensitivity profile of Klebsiella pneumonia was similar to E.coli. Unfortunately, resistance was only provided in few cases.
Conclusion: The most common organisms in acute appendicitis are E.coli, Klebsiella pneumonia, Streptococcus spp, Enterococcus spp, and Pseudomonas aeruginosa. These organisms are, however, sensitive to the commonest antibiotics given at Dr George Mukhari Hospital for acute appendicitis. It was difficult to assess the resistance pattern as not enough information was provided on microbiological reports.
ABSTRACT 34
OUTCOMES OF COMPLICATED APPENDICITIS IN A RESOURCE LIMITED SETTING: IS CONSERVATIVE MANAGEMENT A BETTER OPTION?
Adu-Gyamfi R1, Forgan T2
Division of Surgery, Stellenbosch University/Tygerberg Academic Hospital
2Division of Surgery, Stellenbosch University/Tygerberg Academic Hospital
Introduction/Background: Recent data and studies seem to be favouring the conservative management of complicated appendicitis. The World Society of Emergency Surgery (WSES) Jerusalem guidelines on the management of complicated appendicitis (CA) recognizes that appendicectomy is a safe treatment option if performed by an experienced surgeon, but ultimately supports the use of conservative management. That said, the management of patients with CA remains controversial, with very little available data, particularly in terms of resource constrained health systems.
Aim(s): This study aimed to compare the efficacy of treatment, length of hospital stay (LOS) and overall cost of treatment of patients with CA who either underwent surgery or were managed conservatively.
Methods: This was a retrospective study conducted at a single tertiary care centre (i.e. Tygerberg Academic Hospital, Western Cape) between 01 January 2016 and 31 December 2017. This study was approved by the Health Research Ethics Committee (HREC) of the University of Stellenbosch.
Results: 141 patients presented with CA during the study period. Ninety-two patients (65.2%) underwent surgery (SG) and the remaining 49 (34.8%) were managed non-operatively (CG). SG patients demonstrated a significantly longer hospital stay than CG patients. Complications during admission (number) were evident in only the SG patients. 23 patients had complications on initial admission and were in SG. Despite there being no significant difference in complication rate at 1-year follow up, SG had a 27.2% readmission rate compared with a 20.4% rate in CG. Significantly higher costs were associated with SG.
Conclusion/Recommendations: CA is a common presentation in the state health system. Our findings, in terms of length of stay, complications and overall cost of treatment, provide some evidence that conservative management of CA can be considered as appropriate in an emerging economy. Further studies are however recommended.
ABSTRACT 35
CONSERVATIVE MANAGEMENT OF UNCOMPLICATED APPENDICITIS IN A RESOURCE- CONSTRAINED ENVIRONMENT: FEASIBLE PRACTICE?
Adu-Gyamfi R1, Forgan T2
1 Division of Surgery, Stellenbosch University, & Tygerberg Academic Hospital
2Division of Surgery, Stellenbosch University, & Tygerberg Academic Hospital
Introduction/Background: Acute appendicitis is one of the most common causes of the acute abdomen and emergency abdominal surgery. Fear of perforation, coupled with the introduction of laparoscopic surgery, has led to a low threshold for operative intervention. This has contributed to a high negative appendicectomy rate, high surgery-related morbidity and increased cost of care. In a resource-constrained environment, negative appendicetomy incurs significant losses from relative loss in theatre time, cost of procedure, management of possible complications, and hospital bed occupancy. There is evidence, mostly from the advanced economies, to suggest that uncomplicated appendicitis (UA) can be effectively and safely treated with antibiotics to reduce overall costs of treatment and economic losses. However, there is very little evidence that similar management guidelines can be instituted in an emerging economy where resources are scarce.
Aim(s): To assess the outcomes of antibiotic treatment as an option for UA, compared with appendicectomy, in a resource-constrained setting.
Methods: This was a retrospective study conducted at a single tertiary care centre (i.e. Tygerberg Academic Hospital, Western Cape) between 01 January 2016 and 31 December 2017. This study was approved by the Health Research Ethics Committee (HREC) of the University of Stellenbosch.
Results:118 patients presented with UA. Eighty patients (67.8%) underwent surgery (SG), while the remaining 38 patients (32.2%) were managed with antibiotic alone (AG). Length of hospital stay was significantly longer in the SG patients. At 6 weeks, the recurrence rate of acute appendicitis in the AG patients was 5.3% (2 patients). These were successfully treated with appendicectomy. Recurrence in AG patients was not evident at 1 year. Overall, significantly higher costs were associated with SG.
Conclusion/Recommendations: Even though preliminary evidence seems to be in favour of medical management of UA, further studies need to be conducted to aid in the formulation of appropriate guidelines in our setting.
ABSTRACT 36
PREVALENCE AND FACTORS ASSOCIATED WITH COMPLICATED ACUTE APPENDICITIS IN CHILDREN OF <13: ONE YEAR RETROSPECTIVE STUDY
Loko EM1, Apalata RT2, Delgado A3
1Department of Surgery, Nelson Mandela Academic, Hospital, WSU
2Department of Pathology, Microbiology, WSU AND NHLS
3Department of Surgery, Paediatrics Surgery, WSU
Introduction: NMAH as a single Centre receiving patients from about 20 districts hospitals where populations are mainly poor and essentially represented by blacks. Appendicitis is the most common cause of acute abdomen in children as in adult worldwide. About 50% of patients admitted at NMAH paediatric surgery from appendicitis.
Aims: To determine the prevalence and factors associated with complicated acute appendicitis in children of <13 years admitted at NMAH.
Methods: A cross-sectional retrospective study was conducted on a convenient sample size of 310 patients collected from April 2018 to April 2019 using a chart review. SPSS 22 software was used for data analysis.
Results: A total of 310 children were enrolled of which 137 (44.2%) were females and 173(55.8%) were males. The mean age of the study participants was 9.3 years (SD 2.4years) ranging from 2 to 13 years.
Out of 277 cases, 210 (75.8%) were complicated vs 67 (24.2%) were uncomplicated appendicitis. Of 210 complicated appendicitis, 100 (47.6%) were perforated and 110 (52.3%) were non perforated whilst 67 (24.2%)uncomplicated appendicitis were non perforated histologically(Chi square=46.6; p<0.0001).
Of 310 cases 45 (14.5%) developed post op complications: 51.1% surgical wound sepsis, 22.2% abdominal sepsis, 17.8% surgical site infection and abdominal sepsis. 8.8% readmission rate.
Patients who spend more than 24 hours from arrival at accident and emergency to theatre were high likely to develop complicated appendicitis as compare to those who spent less or equal to 24 hours (OR=1.9; CI: 0.7-5.6) but this difference did not achieve statistical significance (p=0.17).
Conclusion: There is a high rate of non-perforated appendicitis that are histologically perforated and time from A&E arrival to theatre is a key determine factor to complication.
Patients arriving to A&E diagnosed with acute appendicitis should be taken to theatre within the 24 hours of arrival.
ABSTRACT 37
INCIDENCE OF SURGICAL SITE INFECTION (SSI) AFTER PRIMARY OR DELAYED WOUND CLOSURE IN ADULT PATIENTS WITH RUPTURED ACUTE APPENDICITIS: A RETROSPECTIVE ANALYSIS
Langasiki P, Molaoa SZ
Department of Surgery, Nelson Mandela Academic Hospital and Walter Sisulu University
Introduction: Appendicitis, although a common surgical condition, continues to be a diagnostic and management challenge. Life-time risk of developing the condition is estimated to be about 7%. Appendicectomy without post-operative antibiotics remains the standard of care in uncomplicated appendicitis. However, complicated appendicitis warrants appendicectomy and post-operative antibiotics. The role of primary wound closure or delayed wound closure to prevent SSI after appendicectomy for ruptured appendix has been the area of controversy.
Rupture appendix remains a common presentation at Nelson Mandela Academic Hospital; and wound infection following open appendicectomy for ruptured appendix has been an ongoing problem.
Aim of the study: The aim of this study is to compare the risk of SSI after primary and delayed primary wound closure after appendicectomy for ruptured appendix.
Materials and Method: Data was collected retrospectively from case records of adult patients who were operated for ruptured appendix over a one year period (January 2017 to January 2018). Incidence of SSI was compared between the group of patients whose wounds were closed primarily and those who underwent delayed primary closure.
Results: Over a one year period, 91 patients presented with ruptured appendix. There were 58 (64%) males and 33 (36%) females, with mean age of 27 years. Sixty-five patients were managed with delayed primary closure (DPC) and 26 patients with primary closure (PC). Of 91 patients who presented with ruptured appendix, the incidence of SSI was 26.37% (24). Of 65 patients who underwent DPC, incidence of SSI was 3% (2); on the other hand, there was 84.6% (22 of 26) risk of SSI in those who underwent PC. PC increases Risk of SSI 28.2 fold (Relative Risk of SSI after PC) or 81.6% of SSI in this study was attributed to PC.
Conclusion: The results of this study has demonstrated that primary closure of the skin after open appendicectomy for ruptured appendix is associated with 28 fold increase in the risk of SSI. Emphasis should therefore be places on DPC as the standard of care in patients at high risk of postoperative SSI.
ABSTRACT 38
THE INCIDENCE OF COMPLICATED APPENDICITIS AMONG PATIENTS PRESENTING WITH ACUTE APPENDICITIS AT NELSON MANDELA ACADEMIC HOSPITAL
Saqu T, Molaoa SZ
Department of Surgery, Nelson Mandela Academic Hospital and Walter Sisulu University
Introduction: Acute appendicitis is a common surgical condition with the incidence of 100 per100 000; and the lifetime risk of developing the disease of 8.6% and 6.7% in males and females, respectively. Ninety percent of cases occurs in children and young adults, and 10% in patients over the age of sixty years. Low income countries have higher incidence of complicated appendicitis (36.25%) in comparison with middle and high income countries with the incidence of 35.33%. The incidence of complicate appendicitis and its associated mortality and morbidity has not been studied at Nelson Mandela academic Hospital.
Aim of the study: The aim of this study is to determine the incidence of complicated acute appendicitis and its associated morbidity and mortality at our institution.
Material and Methods: The data was collected prospectively from patients of three years of age and above who presented at emergency unit with acute appendicitis; from January to December 2016. Ethical approval was obtained from the University Ethics Committee.
Results: During the study period 466 patients with acute appendicitis were admitted. The mean age of the patients was 21 years. There were 230 (49.4%) males and 236 (50.6%) females. The incidence of complicated appendicitis was 64.8% (302). One hundred and ninety three (64%) of whom had ruptured appendix with generalised peritonitis; and 109 (36%) had appendicular abscess. There was 164 (35.2%) cases of simple appendicitis. Of 302 patients with complicated appendicitis, 30 (14.8%) developed intra-abdominal abscesses; and there was 25% (75) incidence of surgical site infection (SSI). There were four (1.3%) death. Length of hospitalisation was up to five days in 76%; 6 to 10 days in 9.4% and more than 10 days in 14% of patients.
Conclusion: The incidence of complicated appendicitis at our institution is high. Though mortality in complicated appendicitis was low in this study, it demonstrated association with high morbidity and long hospital stay.
ABSTRACT 39
AUDIT OF BURN PATIENTS PRESENTING TO KALAFONG ACADEMIC HOSPITAL: A 5 YEAR REVIEW
Jaffer T, Montwedi D
Department of Surgery, Kalafong Academic Hospital, University of Pretoria
Background: Burn injuries are common and cause tremendous physical and emotional injury to those affected. Management of burn wounds are extensive and multi-disciplinary which often leaves a large economic impact on the health system. Kalafong Academic Hospital (KAH) has a resource constraint 12 bed ward which accepts burn injuries from across Pretoria as well as areas north of the Jukskei River.
Aim: Review and improve the immediate and long-term management of burn patients at KAH.
Method: A 5 year retrospective review (January 2014 -December 2018) of adult (12 years or older) patients admitted to the KAH burns ward or ICU. Data was reviewed to identify patient demographics, burn injury patterns and length of hospital stay.
Results: 456 adult patients were admitted over the study period (female: 37,4%, male: 62,6%). Most patients were in the 21-40-year age range (21-30 years: 35,7%; 31-40 years: 25,65%). Flame burns accounted for 75,44% of admissions. Young males between 21-30 years accounts for 56,5% of electrical burns. February and July showed the most admissions during the year (49). Approximately 4,82% of burn patients required ICU admission. Over the 5-year study period; mortality per TBSA was as follows: 0.33% below 20% TBSA, 7,96% between 20 - 50% TBSA, 55,56% between 50-70% TBSA and 95% for >70% TBSA group. Length of hospital stay varied on the TBSA burnt, averaging 56,49 days in hospital across all burn admissions.
Conclusion: Burn injuries can be fatal if not managed brisk and appropriately. Adequate protocols should be in place to allow appropriate management of burn wounds. Burn units should ideally have an in-ward dedicated burn theatre as well as ICU rooms to allow for adequate and prompt management.
ABSTRACT 40
EVALUATING TRAUMA SCORING SYSTEMS FOR PATIENTS PRESENTING WITH GUNSHOT INJURIES TO A DISTRICT-LEVEL URBAN PUBLIC HOSPITAL IN CAPE TOWN
Aspelund AL1, Patel MQ2, Kurland L3, McCaul M4, van Hoving DJ5
1Department of Research and Education, Karolinsha Institutet, Stockholm, Sweden
2Department of Surgery, Khayelitsha Hospital, Cape Town, South Africa
3Department of Medical Sciences, Department of Emergency Medicine, Örebro
4Biostatistics Unit, Division of Epidemiology and Biostatistics, Department of Global Health, Stellenbosch University, South Africa
5Division of Emergency Medicine, Stellenbosch University, Cape Town, South Africa
Introduction: Trauma scoring systems are widely used in emergency settings to guide clinical decisions and to predict mortality. It remains unclear which system is most suitable to use for patients with gunshot injuries at district-level hospitals. This study compares the Triage Early Warning Score (TEWS), Injury Severity Score (ISS), Trauma Score-Injury Severity Score (TRISS), Kampala Trauma Score (KTS) and Revised Trauma Score (RTS) as predictors of mortality among patients with gunshot injuries at a district-level urban public hospital in Cape Town, South Africa.
Aims: To compare trauma scoring systems in the setting of gunshot injuries at a district-level hospital in predicting mortality.
Material and Methods: Gunshot-injured patients admitted to the resuscitation area of Khayelitsha Hospital between 1 January 2016 and 31 December 2017 were retrospectively analysed. The study was approved by Stellenbosch University Health Research Ethics Committee (Ref: N18/03/033). Receiver Operating Characteristic (ROC) curve analysis were used to determine the accuracy of each score to predict in-hospital mortality. The odds ratio (with 95% confidence intervals) was used as a measure of association.
Results: In total, 331 patients were included in analysing the different scores (abstracted from database n = 431, exclusions: missing files n = 16, non-gunshot injury n = 10, <14 years n=1, information incomplete to calculate scores n = 73). The mortality rate was 6% (n=20). The TRISS and KTS had the highest area under the ROC curve (AUC), 0.9 (95% CI 0.830.96) and 0.86 (95% CI 0.79-0.94) respectively. The KTS had the highest sensitivity (90%, 95% CI 68%-99%), while the TEWS and RTS had the highest specificity (91%, 95% CI 87%-94% each) (see Table).
Conclusion/Recommendations: None of the different scoring systems performed better in predicting mortality in this hightrauma burden area. The results are limited by the low number of recorded deaths and further studies are needed.
ABSTRACT 41
THE GAP IN OPERATIVE EXPOSURE IN TRAUMA SURGERY: QUANTIFYING THE BENEFITS OF AN INTERNATIONAL ROTATION
Barmparas G1, Navsaria P2, Dhillon N1, Edu S2, Margulies DR1, Ley EJ1, Gewertz BL1, Nicol AJ2
1Cedars-Sinai Medical Center, Department of Surgery, Los Angeles, CA USA
2Department of Surgery, University of Cape Town Health Sciences Faculty
3Trauma Centre, Groote Schuur Hospital, Observatory, Cape Town, South Africa
Background: International rotations with hands-on experience are commonly cited as a potential supplement to the current experience of surgical trainees in trauma, however, quantification of this experience remains unclear.
Methods: A link to an online survey was distributed by electronic mail to physicians who rotated for any period of time at the Trauma Unit of the Groote-Schuur Hospital of the University of Cape Town from 1/1/2006 to 12/2016.
Results: Of 160 participants, 75 (47%) completed the survey. A high proportion (45%) had performed less than 25 trauma-related surgical procedures during their previous training. The majority (56%) performed >10 trauma laparotomies and sternotomies/thoracotomies during their rotation, while 43% performed >5 vascular procedures. The level of perceived confidence in managing trauma patients increased significantly from a median of 3/10 to 7/10 (p<0.05).
Conclusion: Rotations at large-volume trauma centres locally offer the opportunity for a handson operative experience and may enhance the confidence of international surgical trainees. Further standardization of these opportunities may result in a larger scale participation of graduate residents and fellows.
ABSTRACT 42
PENETRATING ABDOMINAL TRAUMA IN THE ERA OF SELECTIVE CONSERVATISM A PROSPECTIVE COHORT STUDY IN A LEVEL 1 TRAUMA UNIT
Sander A1 Spence RT2, Ellsemere J2, Hoogerboord M2, Nicol A1, Edu S1, Navsaria P1
1University of Cape Town, Department of General Surgery, South Africa
2Dalhousie University, Department of General Surgery, Canada
Background: Penetrating abdominal trauma (PAT) in South Africa represents a significant burden of disease. The current global trend has seen management shift towards selective conservatism.
Aim: The purpose of this study is to compare the presentation, management and outcomes of PAT patients managed operatively, both immediately and delayed (failed NOM), as well as non-operatively (NOM) in order to provide further evidence-based guidance for the safe implementation of selective conservatism in PAT.
Methods: Prospective cohort study of all patients presenting with PAT to Groote Schuur Hospital, Cape Town, South Africa from 01 May 2015 to 30 April 2017. Presentation, management and outcomes of patients were compared by operative strategy. Univariate predictors of failed NOM were explored. The positive predictive value (PPV) of operative indications for therapeutic laparotomy was calculated and outcomes between the subgroups were compared.
Results: During the 2-year study period, 805 patients with penetrating abdominal trauma were managed. There were 502 (62.4%) and 303 (37.6%) patients with gunshot (GSW) and stab wounds (SW), respectively. The majority were young men (94.7%), with a mean age of 28.3 years (95%CI 27.7-28.9) and median ISS 13 (IQR 9-22). More than one penetrating injury was present in 68.2% of SW and 64.0% of GSW. Successful non-operative management was achieved in 300 (37.5%) patients and 501 (62.5%) were managed operatively; 477 (59.6%) underwent immediate laparotomy and 24 (3.0%) failed non-operative management. Patients managed by immediate laparotomy were more likely to have sustained a GSW, anterior abdominal wound and have higher median ISS. On univariate analysis; number, location and mechanism of injuries were not associated with failed NOM. Rates of therapeutic laparotomy were achieved in 91.0% in the immediate and 85.3% in the failed NOM cohorts. On arrival, immediate laparotomy was performed for haemodynamic instability in 44 (5.5%) patients (PPV 93.2%), peritonism in 298 (37.2%) patients (PPV 93.3%), unreliable clinical assessment in 21(2.6%) patients (PPV 66.7%), radiological findings in 54 (6.7%) patients (PPV 87.0%) and for organ evisceration in 29 (3.6%) patients (PPV 89.7%). Of those failing NOM, 2 (8.3%) became haemodynamically unstable (PPV 100%), 14(58.3%) developed peritonism (PPV 85.7%), 10 (41.7%) had positive radiological findings (PPV 87.5%) and 8 (33.3%) developed signs of sepsis (PPV 87.5%). The mortality rate was 1.7% in the NOM, 10.9% in immediate laparotomy and 0% in the failed NOM subgroups. The rate of complications, ICU admission, reoperation and missed injuries were no different in the immediate and failed NOM cohorts (p>0.05).
Conclusion: Patients presenting with PAT in the absence of haemodynamic instability, peritonism, organ evisceration, unreliable clinical examination and positive radiological findings can be managed expectantly without increased morbidity or mortality.
ABSTRACT 43
COMPLIANCE WITH SURGICAL SAFETY CHECKLIST COMPLETION OF KALAFONG HOSPITAL THEATRE
Montwedi OD
Department of Surgery; University of Pretoria
Background: The WHO undertook number of global and regional initiatives to address surgical safety. First initiatives focussed on access and quality of care and second challenge "Safe Surgery Saves Lives, focusses on safety of surgical care. Surgical safety checklist was published in 2008 and has the potential to minimise post-operative adverse events. Adherence to it will reduce unnecessary perioperative complications. International study of 357 hospitals in 58 countries showed 38% lower odds of 30-day mortality compared to places where the checklist was not adopted. There is a need for on-going feedback and audits on compliance to this safety checklist to avoid unnecessary complications.
Aim: To evaluate adherence/ compliance to the WHO checklist at Kalafong Hospital Theatre.
Methods:.Files of patients who underwent surgical procedures in October and November 2018 were collected, WHO surgical safety checklist were retrieved and evaluated for completeness in relation to time of day, weekday, emergency or elective surgery. Poor compliance includes incomplete and blank forms.
Results: 421 surgical safety checklists were evaluated randomly. Compliance was 48.93%. There was a tendency for incomplete filling of forms at night, weekends and emergency. The most commonly omitted steps were Time out and sign out factors.
Discussion / Conclusion: Approximately 234 million procedures are performed annually worldwide with complications between 3-16%. Most of these can be avoided according to many studies. Studies from Ethiopia and 15 other African countries highlight lack of compliance as ours also confirms. Barriers to lack of compliance need to be evaluated. Auditing of compliance should become part of performance indicators and national core standards and should be regularly conducted at every hospital if adverse events are to be avoided. Compliance was suboptimal in our institution and should be improved.
ABSTRACT 44
PREDICTORS OF POST PARATHYROIDECTOMY HYPOCALCEMIA IN THE TREATMENT OF PRIMARY HYPERPARATHYROIDISM AT TYGERBERG HOSPITAL
Mouton HP, Nzama DZ, Conradie W
Department of Surgery, Faculty of Medicine and Health Sciences, Stellenbosch University
Introduction: Primary hyperparathyroidism (PH) is defined as autonomous parathyroid hormone (PTH) production, characterised by elevations in serum calcium (Ca) and PTH levels. Hypocalcaemia is a complication in 15-30% of cases.
Aim(s): To identify pre-operative predictors of hypocalcemia in our population.
Methods: Retrospective review of all patients that underwent parathyroidectomy for PH at TBH between Jan 2010 and Mar 2019. Approval was granted by the Health Research Ethics Committee of Stellenbosch University. Due to the short retrospective study period, only data from 137 patients was available for review. Of these, 87 (64%) underwent parathyroidectomy for PH, whilst incomplete, post-operative Ca levels were available for 80 patients. Patients were divided into 2 groups based on post-operative Ca levels (Group 1: >1.99 (n=69); Group 2: <1.99 (n=11). Baseline characteristics were compared.
Results:
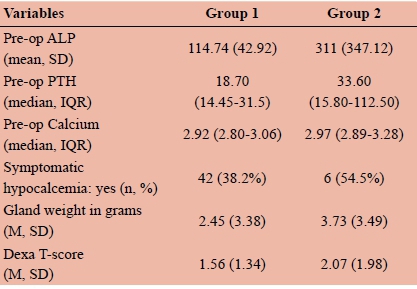
Conclusion: Patients in Group 2 demonstrated higher pre-operative ALP, PTH and Ca levels. Despite no significant differences seen between the 2 groups, certain pre-operative trends were noted. Due to incomplete data, we recommend that a prospective study be conducted.
ABSTRACT 45
A RETROSPECTIVE REVIEW OF PEPTIC ULCER PERFORATIONS IN HARARE, ZIMBABWE
Mlambo BR1, Maunganidze AJV1, Chinyowa S1, Wren S2
1 Department of Surgery, University of Zimbabwe
2Department of Surgery, Stanford University
Introduction/Background: The limited literature on peptic ulcer perforation in Africa depicts a disease where young adults are most at risk, with smoking and alcohol being significant risk factors for perforation. This is in contrast to Western literature where the disease largely affects elderly patients with co-morbidities taking non-steroidal anti-inflammatory drugs (NSAIDS). Several clinical prediction models (CPMs) exist for triage and risk stratification of these patients but none has been validated in our setting.
Aim(s): To identify risk factors associated with mortality from perforated peptic ulcer disease (PUD) and to determine which CPM most accurately predicts mortality from peptic ulcer perforation in Harare, Zimbabwe.
Methods: We retrospectively reviewed records of patients at Parirenyatwa Hospital in whom a diagnosis of perforated PUD was made between 1 January 2017 and 15 September 2018. A data collection tool was used to abstract putative risk factors for mortality and information pertinent to all categories of selected CPMs. Receiver Operator Characteristic curves for each of the CPMs were compared to determine the best predictor of mortality. The main outcome was 30-day mortality. Ethical considerations: Ethics approval from the Joint Research and Ethics Committee (JREC)
Results: 105 patients were included with median age 36 years. M:F ratio was 23:3. NSAID use, alcohol and smoking were reported in 21.8%, 63.4% and 56.3% of patients respectively. Factors associated with mortality were presence of multiple co-morbidities (OR:3.7, p = 0.022); Ulcer size > 2 cm (OR 8.1, p = 0.000) and raised serum creatinine (OR 11.4, p = 0.000). AUC of the selected CPMs were: Mannheim Peritonitis Index Score 77.4% (95% CI 65.7- 89.1); Boey Score 75.9% (95% CI 63.5 - 88.4); Pulp Score 72.3% (95% CI 59.0 - 85.7) and Jabalpur Score 70.8% (95%CI 58.6 - 82.9).
Conclusion/Recommendations: Multiple co-morbidities, large ulcer size and raised serum creatinine were associated with higher risk of mortality. The Mannheim Peritonitis Index Score most accurately predicts mortality from perforated PUD in Harare.
ABSTRACT 46
COMPARISON OF 14C-UBT, PCR AND CLO TEST IN THE DETECTION OF HELICOBACTER PYLORI AMONG PATIENTS IN CHRIS HANI BARAGWANATH HOSPITAL SOUTH AFRICA
Idowu A1,2, Candy PG2, Mzukwa A1, Harrison U3, Palamides P3, Haas R3, Mbao M4, Mamdoo R4, Bolon J4, Chopdat N4, Gasim I4, Baga H4, Jolaiya Γ, Smith S6, Ally R4, Clarke AM1, Njom HA1
1Department of Biochemistry and Microbiology, University of Fort Hare, South Africa
2Department of Surgery, Faculty of Health Sciences, University of The Witwatersrand, South Africa
3Max von Pettenkofer-Institute, Faculty of Medicine, LMUMunich, Germany
4Division of Gastroenterology, Chris Hani Baragwanath Hospital Johannesburg, South Africa
5Department of Microbiology, University of Lagos, Nigeria
6Molecular Biology Department, Nigerian Institute of Medical Research, Lagos, Nigeria
Background: The global prevalence of Helicobacter pylori approaches 50%, with prevalence rates between 20 and 40% in developed countries and up to 90% in Africa and other developing nations. Several diagnostic methods (invasive and non-invasive) have been proposed for the detection of H. pylori infection with all of the tests having their limitations.
Aim: The study aimed at comparing carbon-14 urea breath test (14C UBT), polymerase chain reaction (PCR) and the Campylobacter-like organism (CLO) tests in the diagnosis of H. pylori infection in relation to the endoscopic assessment, and associated risk factors.
Method: Participants booked for upper gastroscopy were recruited for the study. The identified laboratory tests were conducted using standard procedures, and data of associated risk factors were collected by means of questionnaires. The research protocol was approved by the Ethics Committee of the Chris Hani Baragwanath Hospital (registration number M160228). Written informed consent was obtained from all participants.
Results: A total of 184 patients were enrolled between May and June 2016 in Baragwanath Hospital, 126(68.5%) showed a positive result in the 14C UBT, 150(81.5%) PCR and 122(66.3%) CLO test. All the CLO test positive patients were also confirmed positive in the 14C UBT. Significant disagreement occurred between 14C UBT vs PCR and as well as CLO vs PCR however, all the methods showed the agreement of 72.8% (positivity=111/184; negativity=23/184) and positive correlations (0.95, 0.37, 0.34). Of the 126 patients diagnosed by 14C UBT (as the gold standard), infection percentage was highest 56/126 (44.4%) in patients having gastritis. Acquisition of H. pylori was not significantly associated with any of the epidemiological / socioeconomically risk factors investigated, however, crowded living and lack of formal education showed high potential risk factors for the transmission of H. pylori.
Conclusion: Findings show a high percentage agreement among methods, however, for clinical practice, the diagnosis requires that two of these types of test to be positive, or that positive isolation of H. pylori by culture is obtained.
ABSTRACT 47
INDICATIONS AND RISK FACTORS FOR LIMB AMPUTATION IN HUMANITARIAN SURGERY
Naidu P1, Dominguez L2, Trelles M2, Chu K1
1Department of Surgery, Faculty of Health Sciences, University of Cape Town,
2Medical Unit, Operational Centre Brussels, Médecins Sans Frontières
Introduction/Background: Limb amputations (LA) are a common surgical procedure worldwide and usually a result of diabetes, atherosclerosis, infections, or traumatic injury. Médecins Sans Frontières (MSF) provides surgical care in areas of conflict (CON), natural disaster (ND), or other settings with poor surgical systems (PSS).
Aim(s): The objectives of this study were to describe indications for LA and their associated risk factors in the humanitarian setting.
Methods: The objectives of this study were to describe indications for LA and their associated risk factors in the humanitarian setting.
Ethical considerations: MSF Ethics Review Board
Results: There were 1621 LA in 1188 patients from 17 countries 73% were males and the median age was 30 years. Trauma was the most common indication for LA (n=1219,75%) with 51%(n=826) from unintentional trauma. Infection accounted for (n= 289, 18%). On multivariate analysis, age<30 years (OR=2.83, p<0.001), male gender (OR=2.23, p<0.001), CON setting (OR=3.98, p<0.001) and emergency procedure (OR=5.6, p<0.001) were associated with intentional trauma. CON setting was less likely to be associated with unintentional trauma (OR=0.67, p>0.001). Age >30 years (OR=3.09, p<0.001), female gender (OR=2.09, p<0.001), and non-emergency procedure (OR=4.53, p<0.001) were associated with infectious indications.
Conclusion/Recommendations: Trauma was the leading cause of LA in the humanitarian setting and improved post-amputation rehabilitation are needed in these contexts. Prevention of unintentional trauma, which was a most common indication, must be a focus on humanitarian organizations in addition to addressing the surgical care.
ABSTRACT 48
WHERE THERE IS NO ORTHOPAEDIC SURGEON: A WHATSAPP MHEALTH PLATFORM TO SUPPORT FRACTURE MANAGEMENT BY NON-SPECIALISTS IN SOUTH AFRICA
Kauta JN1, Groenewald J2, Arnold D2, Blankson B2, Omar A2, Naidu P1, Chu K1
1Department of Surgery, Faculty of Health Sciences, University of Cape Town
2Mitchell's Plain Hospital, Mitchell's Plain, Cape Town
Introduction/Background: Traumatic fractures are common in sub-Saharan Africa (SSA), a region with a shortfall of orthopaedic surgeons, and can result in morbidity if not appropriately treated. WhatsApp is an encrypted smartphone application with 1.5 billion users in 180 countries and ubiquitous in SSA. The objective of this study was to develop an mHealth platform to support fracture management by non-orthopaedic surgeons in Cape Town, South Africa.
Aim(s): The objective of this study was to identify benefits and barriers of training non-SA SSA surgeons at the University of Cape Town.
Methods: A WhatsApp Orthopaedic Referral Group (ORG), was created between non-orthopaedic community health clinic doctors (NON-ORTHO) and orthopaedic surgeons and residents (ORTHO) from a first-level hospital to manage all traumatic fractures. NON-ORTHO referred patients on ORG and advice was provided by ORTHO. Data from January 1-June 30, 2018 was analysed, and outcomes included response time, management advice, and treatment outcome.
Ethical considerations: Human Research Ethics Council UCT.
Results: 72 NON-ORTHO referred 836 patients to the 5-member ORTHO team. Median response time was 10 minutes (interquartile range,5-29 minutes). The proportion of responses under 1 hour was 88% (n=746). 371 (44.4%) were successfully treated by NON-ORTHO at the community health clinic, 359 (42.9%) were treated by ORTHO at the first-level hospital and 102 (12.2%) were directly referred to an orthopedic subspecialist at the third-level academic hospital.
Conclusion/Recommendations: South Africa has a limited number of orthopedic surgeons but a high burden of traumatic fractures. ORG provided a free tele-mentoring platform for non-orthopedic doctors to successfully manage selected cases at community health clinics. This type of mHealth platform can be applicable to other resource-limited settings if disease burden is high and specialists are scarce.
ABSTRACT 49
CLASSICAL MUSIC AND MELODIC DEATH METAL: INSIGHTS INTO AUDITORY VERBAL LEARNING AND MOOD
Gilbert A1, Augustine TN1, Correia AF2, Gravett N1
1School of Anatomical Sciences, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg
2Department of Psychology, School of Human and Community Development, Faculty of Humanities, University of the Witwatersrand, Johannesburg
Background: Classical music is thought to be an affective prime for memory processes; however, the effect of "melodic death" or "melodeath" metal music is unknown.
Aim: We assessed Vivaldi's "Four Seasons" Concerti (Spring) and Bel'akor's "Countless Skies" on the mood and learning of undergraduate health science students (Human Research Ethics Clearance H15/08/03).
Methods: Both pieces, composed in E major had fast tempos and positive valence. Duration and volume were controlled (10 minutes, 50 dB). After screening for a range of diseases and disorders, participants (N=22) completed a questionnaire describing factors that could influence subsequent assessments. Each participant partook in one intervention per week: Intervention 1 was baseline (silence), Intervention 2 and 3 were exposure to classical and melodeath music respectively. Before and after each intervention, participants completed the Brief Mood Introspection Scale (BMIS) and the Four Mood Introspection Scale (FMIS) to determine changes that may affect memory processes. To assess verbal learning and declarative memory processes, participants completed the Rey Auditory Verbal Learning Test (RAVLT) whereby a series of word lists were used to measure immediate, delayed and cued recall; attention and learning under information overload.
Results: Participants who studied to music regularly performed significantly worse (p<0.05) in immediate recall and learning under information overload; however, musical proficiency significantly enhanced attention. Neither musical piece had any significant effect on learning processes; however, both decreased "arousal-calm" and increased "positive-tired" measures (p<0.05). While "happiness" increased post-intervention, highlighting the E major effect, feelings of "anger" were recorded to melodeath. Although the lyrics were non-violent, death growl vocals may have contributed to this emotion. Overall, the emotional response to melodeath metal may be due to unfamiliarity with this genre and negative societal perceptions.
Conclusion: This study provides evidence that melodeath music does not have a detrimental effect on verbal and auditory memory, nor does classical music have any benefit, contrasting with current literature.
ABSTRACT 50
THE CONTRIBUTION OF THE UNIVERSITY OF CAPE TOWN TO THE TRAINING OF SUB-SAHARAN AFRICAN SURGEONS
Naidu P1, Lategan C1, Devenish L1, Chu K2
1Department of Surgery, Faculty of Health Sciences, University of Cape Town
2Department of Global Health, University of Stellenbosch
Introduction/Background: Sub-Saharan Africa (SSA) has a shortage of surgeon specialists. Many SSA countries lack residency programs but South Africa (SA), a middle-income country, has several post-graduate surgical training programs.
Aim(s): The objective of this study was to identify benefits and barriers of training non-SA SSA surgeons at the University of Cape Town.
Methods: This was a 2-part cross-sectional survey administered between June 1, 2018 and March 1, 2019 to 1) surgical heads of divisions and 2) surgical residents and fellows who graduated between 2007-2017 and whose home country was in SSA but not SA. All data was captured on REDCap, a secure online database.
Ethical considerations: Human Research Ethics Council UCT.
Results: 7/10 division heads responded and reported benefits of having SSA trainees included having more junior staff (n=5, 71%) and the establishment of regional networks (n=4,71%). Negative impacts included increased training load (28%, n=2) and fewer cases for SA trainees (28%, n=2). 30/78 (38%) trainees responded. 83% (n=25) of trainees were male. 80% (n=24) returned to their home country after training; 83% (n=22) worked in the public sector and 90% (n=27) in teaching hospitals.
Conclusion/Recommendations: SSA surgeons can utilize regional training programs until their own countries increase their training capacity. Regional training environments are more relevant than training in a high-income setting. The majority of trainees returned to their countries of origin, utilizing their skills in the public and academic sectors, contributing to the teaching of more trainees. The expansion of these programs is warranted especially the active recruitment of female SSA surgical trainees.
ABSTRACT 51
HELICOBACTER SPECIES IN RAT MODELS OF HYPERTENSION
Thiba A, Nweke E and Candy G
Department of Surgery, Health Sciences, University of the Witwatersrand, Johannesburg
Background: Helicobacter pylori infects half the world's population and is a known cause of gastritis and is associated with gastric and other cancers. H. pylori has been linked to other diseases, including cardiovascular disease (CVD) through epidemiological studies and blood pressure decreases upon successful eradication using antibiotics. Very little is known about the prevalence of Helicobacter spp in hypertension and whether or not H pylori is causal or simply associated with CVD.
Aim: To determine the presence and abundance of Helicobacter spp in hypertensive and normotensive animal models.
Methods: Stomach, intestinal and faecal samples were harvested from normotensive Dahl (n=4), Dahl salt sensitive (SSR; n=3) and spontaneously hypertensive (SHR; n=3) rats. The samples were cultured in microaerophilic conditions (5% O2-10% CO2-85% N2) and identified using matrix assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF) and biochemical tests. Furthermore, genomic DNA isolation, 16S rRNA gene sequencing, and analysis of microbial composition were performed on the samples.
Results: H mesocricetorum and H rodentum were identified in all the rat models. From the overall bacterial species identified in the gut, the normotensive rats had 2%, SSR, a 3%, whereas SHR had a 2% abundance of both species. SHRs had a 15% abundance of H mesocricetorum and a 5% abundance of H. ganmi. There was a higher prevalence of Helicobacter spp in the hypertensive rats than the normotensive rats.
Conclusion: The presence of Helicobacter spp has observed in both hypertensive and normotensive rat models with a higher abundance of Helicobacter spp in hypertensive models. These data support a role for the bacterium in CVD, but the mechanisms require elucidation.


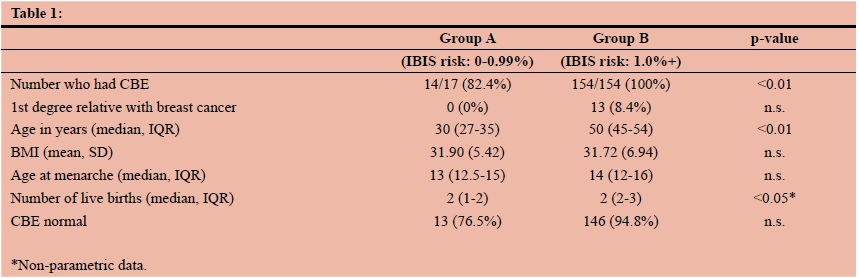{kind=link}
{kind=link}
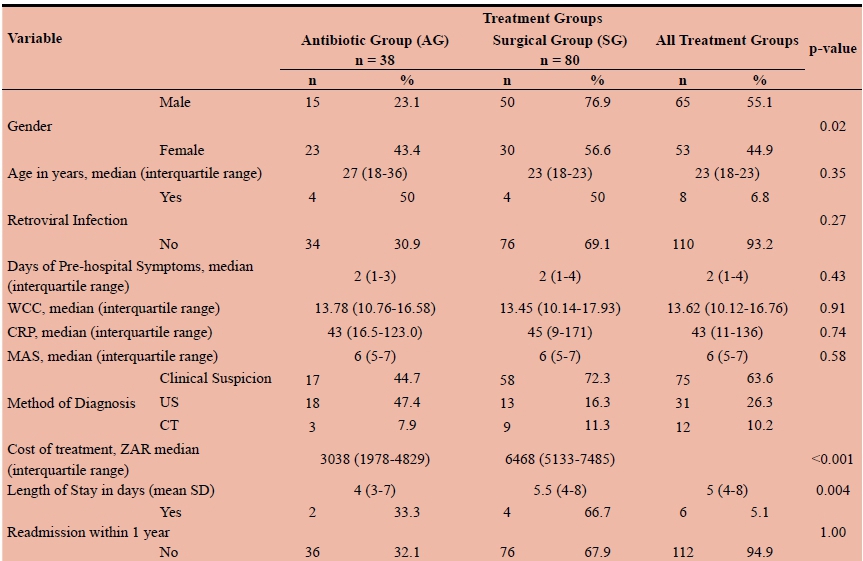{kind=link}
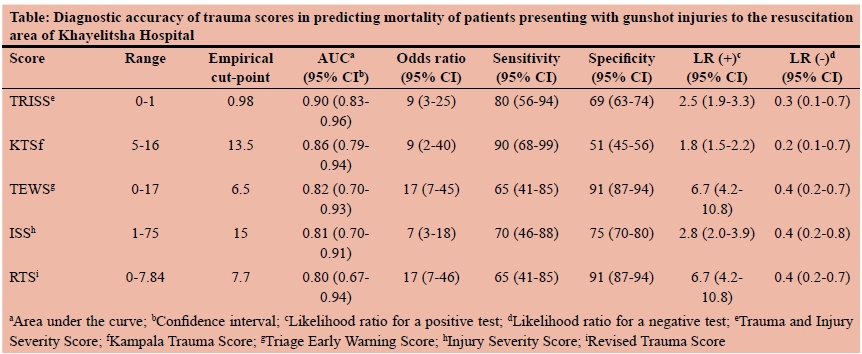{kind=link}