










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.57 no.1 Cape Town Mar. 2019
http://dx.doi.org/10.17159/2078-5151/2018/v56n3a2737
BREAST ONCOLOGY
Lymph node harvest in breast cancer patients with and without preoperative scintigraphy
J EdgeI; M ParkerII; M MaliepaardIII; O UngIV
IDivision of surgery, Stellenbosch University, Western Cape
IIUniversity of Cape Town, Cape Town
IIICharlotte Maxeke Johannesburg Academic Hospital, Johannesburg
IVUniversity of Queensland, Royal Brisbane and Women's Hospital, Qld, Australia
SUMMARY
BACKGROUND: Sentinel lymph node biopsy (SLNB) is the standard of care for women with node negative breast cancer. Tc99 nanocolloid is a popular tracer, facilitating preoperative lymphoscintigraphy to identify sentinel nodes. This study compares the number of sentinel lymph nodes identified at the time of surgery in women who had lymphoscintigraphy with those who did not
METHOD: All women with primary breast cancer undergoing a SLNB from 2003-2017 who were node negative and did not have neoadjuvant chemotherapy were retrospectively reviewed in this study
RESULTS: 576 women who had Tc99 preoperative injection were included in the study. Three hundred patients (Group 1) underwent lymphoscintigraphy preoperatively and 276 (Group 2) had no lymphoscintigraphy. The mean age at diagnosis for Groups 1 and 2 were 56 and 58 years, respectively. Both groups were also found to be similar in terms of histological subtype, tumour location, size, and HER2- and Estrogen receptor (ER) status. The surgery for the breast primary was similar in groups 1 and 2. While both groups had a median number of 2 nodes identified, the mean number of nodes identified for Group 2 (2.12) was 10% higher than for Group 1 (1.92) (p = 0.0026
CONCLUSION: This is the largest series to show that a preoperative lymphoscintigram (scan) can safely be omitted when performing a SLNB. As newer tracers are being used (e.g. Iron Oxide), it is important to know that accuracy of SLNB is not compromised by omission of a scan
Keywords: Lymphoscintigraphy, sentinel node biopsy, breast cancer
Background
SLNB for the management of radiologically and clinically node negative axillae in women with breast cancer has been used for the last 3 decades and has been shown to be a reliable and safe method to manage the axilla.1,2,3
For some surgeons the preferred technique for identifying the sentinel lymph node (SLN) in women with breast cancer is to use Tc 99 nanocolloid as there have been well-recorded cases of anaphylaxis with the use of patent blue.4
Once the colloid had been injected, a preoperative scan was routinely performed to identify the location and number of nodes. The scan takes about 2 hours and may mean the patient has to be seen the day before surgery. The injection of the nanocolloid costs R5460 ($386.00), the injection and a scan is R9830 ($696.72)5 approximately half the cost of the procedure is due to the preoperative scan.
SLNB has been performed at the Netcare Christiaan Barnard Hospital breast care unit since 2003. From May 2012, preoperative scans were omitted. A retrospective audit was performed to analyse the number of lymph nodes identified at the time of surgery (SLNB) in those who did not have preoperative lymphoscintigraphy performed, compared to an historical cohort of patients who did have a preoperative lymphoscitagram.
Objectives of study
To determine whether preoperative lymphoscintigraphy affects the number of nodes identified at the time of sentinel lymph node biopsy (SLNB).
Methods
The historical cohort (Group 1) had a preoperative lymphoscintigram. The number of nodes identified is compared with a subsequent group (Group 2) who did not have a scan. The Tc 99 nanocolloid was injected by the same nuclear medicine team throughout the study period using a consistent technique. In total, 3 ml was injected, 1ml into each of 3 areas: periareolar, intratumourly and subcutaneously. Intraoperatively, nodes from the axilla were sequentially removed until the background count recorded was < 5% of the initial node count.
When a preoperative scan was performed, the number of nodes removed was compared with the number and location seen on the scan to ensure all identified axillary nodes were removed. Identified intramammary nodes were not removed.
All breast cancer patients had their details captured electronically. The patient information was gathered from the histology notes held by the principle investigator. The number of nodes identified at the time of surgery was taken as the recorded number.
All women who had a SLNB performed at Christiaan Barnard Memorial Hospital between 2003 and 2016 were included in the study. After 2012, a routine preoperative scan was no longer requested. Patients treated before this time (Group 1) were compared to those who had their operation after 2012 (Group 2). Between 2003 and 2016, the indications for SLNB and the use of intraoperative assessment changed. Patients with positive nodes, those who had neoadjuvant chemotherapy (NACT), a second breast primary and more than one primary in the breast were excluded. Before 2011 (Group 1), every patient had intraoperative assessment of the SLN. When a positive node was identified, no further nodes were removed. As no further nodes were removed after identification of a positive node, there may have been fewer nodes removed in patients operated on before 2011. To remove the bias, all patients with positive nodes were excluded from the study. To further minimise bias, patients who received NACT were excluded from the study as the technique for performing a SLNB following NACT is different.
The following data were collected: age, histological subtype of breast cancer, primary breast procedure, side, tumour size, receptors status and number of nodes identified. The location of the tumour was not recorded as it does not affect drainage to the axilla.6
All analyses were performed on GraphPad Prism software v6.05 (GraphPad Software, Inc. San Diego, California). Patient demographics and clinical characteristics were analysed using descriptive statistics. Chi-square analysis and Mann Whitney U test were used, where applicable, for comparison of groups. A p-value of less than 0.05 was considered significant.
No financial assistance was received. Ethics committee approval was from University Cape Town: HREC 424/2107.
Results
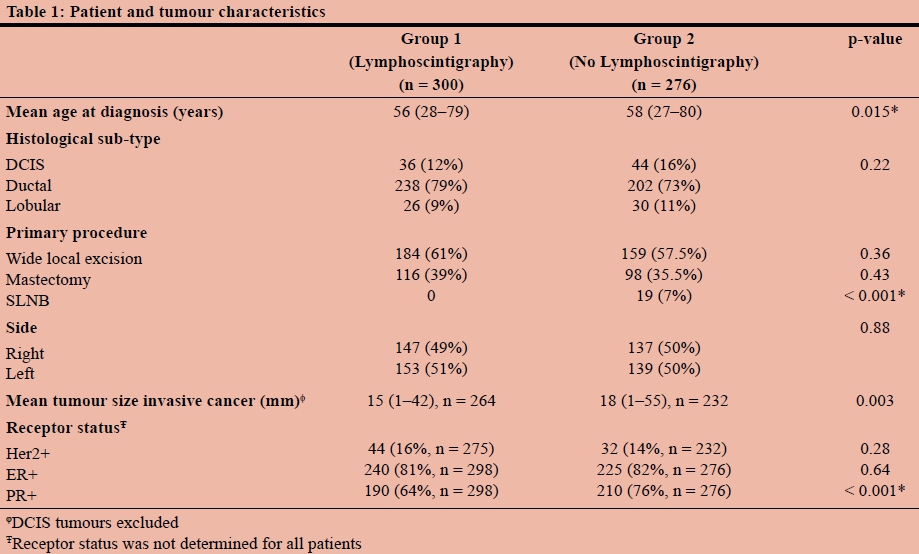
A total of 875 women had a SLNB in the study period. A preoperative scan was routinely performed before 2012 for 459 women. Of those, 159 (34.6%) had a positive node so were excluded from the study. 416 women had a scan after 2012. Of those 136 (32.4%) had a positive node and 4 had a scan as they had NACT or a second primary (Figure 1). A group of 576 women were therefore included in the study. Three hundred patients (Group 1) underwent lymphoscintigraphy preoperatively and 276 (Group 2) had no lymphoscintigraphy. The patient and tumour characteristics were comparable (Table 1). The mean age at diagnosis for Groups 1 and 2 were 56 and 58 years, respectively. Groups were also found to be similar in terms of histological subtype, size and HER2- and Estrogen receptor (ER) status. There was a significant difference in progesterone receptor (PR) status (p < 0.001).
The surgery for the breast primary was similar in Groups 1 and 2. A wide local excision was performed 61% and 57.7% respectively. However, with increasing use of primary systemic therapy there were more sentinel node biopsies performed as a sole procedure in the second group (0% vs 7%) (Table 1).
While both groups had a median number of 2 nodes identified, the mean number of nodes identified for Group 2 (2.12) was 10% higher than for Group 1 (1.92) (p = 0.0026). Table 2 shows that the majority of patients (> 70%) in either group had 1 or 2 nodes identified. However, fewer patients in Group 2 (27%) had a single node identified than in Group 1 (44%) (p < 0.001) (Table 2).
Discussion
In 1977, Cabanas first described the technique of lymph node mapping for the management of penile cancer.7 He determined the SLN using anatomical landmarks. However, the technique was not reproducible so was not widely used. In 1992, Morton used blue dye to trace the sentinel node for melanoma.8 The following year, use of a gamma probe was added to the procedure and the first study was published using the technique to identify the SLN in women with breast cancer.
The accuracy of a SLNB in the management of women with breast cancer is dependent on many factors.9 One is the number of nodes identified at the time of surgery. For the patients in Group 1, the preoperative scan was checked preoperatively and then again intraoperatively after nodes had been removed to ensure all identified on the scan had been removed. Intramammary nodes were not routinely removed.
After a thorough literature review and a period of not routinely seeing the preoperative scan before the procedure, a single breast institution stopped requesting a routine preoperative scan during 2012. The number of nodes removed after the change in practice was recorded and compared to the historical cohort.
Over the years, a number of changes in SLNB protocol were made. Initially, every patient had intraoperative assessment of the SLN. When a positive node was identified, no further nodes were removed. This practice was changed after the publication of The American College of Surgeons Oncology Group ZOO11 study.10 Subsequently, only patients who had a mastectomy had intraoperative assessment. As the surgeon did not remove any further nodes after identification of a positive node, there may have been fewer nodes removed in patients operated on before 2011. To remove the bias, all patients with positive nodes were excluded from the study.
Node positive patients who received neoadjuvant chemotherapy and became node negative were traditionally treated with an axillary clearance. With increasing evidence about the safety of performing a SLNB, this practice was gradually changed.11-14 However, the technique used for these patients is different: a preoperative scan is performed, a dual tracer used and the procedure is converted to an axillary clearance if the nodes are not clearly found. To minimise bias, patients who had a SLNB after primary chemotherapy were excluded.
On average, more nodes were identified in Group 2, where the preoperative scan was omitted. However,the small (10%) difference, may not be considered clinically relevant and we therefore maintain that omission of lymphoscintigraphy does not practically influence intraoperative node assessment. That the number of nodes removed without the use of lymphoscintigraphy was slightly higher suggests that this approach is not inferior.
It is possible that, the slight difference between groups could be explained by a shorter time between injection of the nanocolloid and the operative procedure in Group 2. In Group 1, the lymphoscintigrams had to be done at a neighbouring hospital so, although all the patients had surgery within 24 hours after injection, many patients had their nanocolloid the afternoon before surgery. In the second group, all patients had their surgery within 8 hours of being injected. Although the technique used remained the same throughout the study period, the probe used to identify the nodes was changed in 2008. Therefore, the counts recorded intraoperatively cannot be accurately compared.
Alternatives to Tc nanocolloid are being used more frequently.15,16 The majority of these techniques do not allow any preoperative scanning. It is important to ascertain that the accuracy of the procedure is not affected.
The limitation of the study is that it does not give any indication of longterm outcome of patients not managed with a preoperative scan.
Conclusion
Our study is the largest to date to show that a preoperative scan in an uncomplicated patient with breast cancer makes little difference to the number of lymph nodes identified at the time of surgery. This is consistent with other audits that have shown that lymphoscintigraphy adds little value to intraoperative node identification.17,18
Acknowledgement: Thanks to Matthew Brutus who contributed to data collection
We have no conflict of interest to declare
REFERENCES
1. Kim T, Giuliano AE, Lyman GH. Lymphatic mapping and sentinel lymph node biopsy in early-stage breast carcinoma: a meta-analysis. Cancer. 2006;106(1):4-16. doi: 10.1002/cncr.21568 [ Links ]
2. Veronesi U, Viale G, Paganelli G, et al. Sentinel lymph node biopsy in breast cancer: ten year results of a randomized controlled study, Ann Surg. 2010;251(4):595-600 doi: 10.1097/ SLA.0b013e3181c0e92a [ Links ]
3. Krag DN, Weaver DL, Alex JC, et al. Surgical resection and radiolocalization of the sentinel lymph node in breast cancer using a gamma probe. Surg Oncol. 1993;2(6):335-9. PMID:8130940 [ Links ]
4. Platt P, Roberts L. Anaphylaxis to patent blue dye-misadventure or misdemeanour. Anaesth Intensive Care. 2011;39(4):166-7. ISSN 0310-057X [ Links ]
5. Conversion rate 3/11/2017. R14.11:$1.00
6. Blumgarrt E, Uren R, Nielsen P, Nash M, Reynolds H. Predicting lymphatic drainage patterns and primary tumour location in patients with breast cancer. Br Can Res Treat. 2011;699-705. doi: 130: 699-705. 10.1007/s10549-011-1737-2 [ Links ]
7. Cabanas RM. An approach for the treatment of penile carcinoma. Cancer. 1977;39(2):456-66. PMID: 837331 [ Links ]
8. Morton DL, Wen DR, Wong JH, et al. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg. 1992;127(4):392-9. PMID:1558490 [ Links ]
9. Yi M, Meric-Bernstam F, Ross MI, Akins JS, Hwang RF, Lucci A, et al. How many sentinel lymph nodes are enough during sentinel lymph node dissection for breastcancer? Cancer. 2008;113(1):30-7. doi: 10.1002/cncr.23514 [ Links ]
10. Giuliano AE, Hunt KK, Ballman KV, Beitsch PD, Whitworth PW, Blumencranz PW, et al. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinelnode metastasis: a randomized clinical trial. JAMA. 2011;305(6):569-75. doi: 10.1001/jama.2011.90 [ Links ]
11. Kuehn T, Bauerfeind I, Fehm T, et al. Sentinel-lymph-node biopsy in patients with breast cancer before and after neoadjuvant chemotherapy (SENTINA): A prospective, multicentre cohort study. Lancet Oncol. 2013;14(7):609-618. doi: 10.1016/S1470-2045 [ Links ]
12. Shen J, Gilcrease MZ, Babiera GV, et al. Feasibility and accuracy of sentinel lymph node biopsy after preoperative chemotherapy in breast cancer patients with documented axillary metastases. Cancer. 2007;109(7):1255-63. doi: 10.1002. [ Links ]
13. Takahashi M, Jinno H, Hayashida T, et al. Correlation between clinical nodal status and sentinel lymph node biopsy false negative rate after neoadjuvant chemotherapy. World J Surg. 2012;36(12):2847-52. doi: 10.1007/s00268-012-1704-z [ Links ]
14. Boileau J-F, Poirier B, Basik M, et al. Sentinel node biopsy after neoadjuvant chemotherapy in biopsyproven node-positive breast cancer: The SN FNAC study. J Clin Oncol. 2015;33(3):258-64. doi: 10.1200/JCO.2014.55.782 [ Links ]
15. Ahmed M, Purushotham AD, Douek M. Novel techniques for sentinel lymph node biopsy in breast cancer: a systematic review. Lancet Oncol. 2014;15(8):e351-62. doi: 10.1016/S1470-2045(13)70590-4 [ Links ]
16. Ahmed M, Anninga B, Goyal S, Young P, Pankhurst QA, Douek M; Mag SNOLL Trialists Group. Magnetic sentinel node and occult lesion localization in breast cancer (MagSNOLL Trial). Br J Surg. 2015;102(6):646-52. doi: 10.1002/bjs.9800 [ Links ]
17. Sharma N, Pinto A, Notghi A, Sintler M. Preoperative Scintigrams to Identify the Sentinel Lymph Node in Breast Cancer: a Waste of Time? Indian J Surg. 2015;77(Suppl 3): 1480-3. doi: 10.1007/s12262-013-0994-1 [ Links ]
18. Burak WE, Walker MJ, Yee LD, et al. Routine preoperative lymphoscintigraphy is not necessary prior to sentinel node biopsy for breast cancer. Am J Surg. 1999;177(6):445-9. PMID: 10414690 [ Links ]
 Correspondence:
Correspondence:
Dr Jenny Edge
dr@jennyedge.co.za


{kind=link}
{kind=link}
{kind=link}