










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.56 no.3 Cape Town Set. 2018
http://dx.doi.org/10.17159/2078-5151/2018/v56n3a2253
GENERAL SURGERY
Surgical resources in South Africa: a review of the number of functional operating theatres
AJ Dell; D Kahn
Department of Surgery, University of Cape Town Health Sciences Faculty, Groote Schuur Hospital, Observatory, Cape Town, South Africa
ABSTRACT
BACKGROUND: Surgery has previously been neglected as a development initiative, despite the obvious effect of surgical illnesses on morbidity and mortality. Recently, greater attention has been given to surgical services, as there is growing evidence of cost-effectiveness of surgical interventions. Operating theatre numbers have been used as a measure of surgical capacity, despite there being limitations associated with this use of this metric. This study aims to analyse part of the surgical resources in South Africa.
METHODS: A descriptive analysis of surgical infrastructure in all nine provinces was performed. The total number of functional operating theatres was documented for all public and private hospitals in South Africa. Hospitals were contacted during the period from 1 October 2014 until 31 December 2014.
RESULTS: The results showed 3.59 operating theatres per 100 000 population. This fell below the global average of 6.2 operating theatres per 100 000 as well as other developed countries. Theatres were concentrated in metropolitan areas, and there were a greater number of private operating theatres per insured population than in the uninsured public sector.
CONCLUSION: Strengthening surgical systems will reduce the surgical burden of disease and improve health outcomes globally. Little is known about the available surgical resources such as operating theatre density, although using this metric to evaluate surgical capacity has its limitations.
Key words: Global surgery, Surgical Resources
Introduction
Surgical conditions lead to premature death and disability resulting in an enormous economic burden. Recently, greater attention has been given to surgical capacity, as there is growing evidence of cost-effectiveness of surgical interventions.13 Surgery has been referred to as the "neglected stepchild" of global health, which has resulted from inequalities between high (HIC) and low-income countries (LIC).4
Lancet Commission on Global Surgery
The WHO Global Initiative for Essential and Emergency Surgery (GIEESC) Situational Analysis tool for evaluating a facility's surgical services identifies strengths and weaknesses as well as gaps in infrastructure, human resources, surgical innovations and equipment and is currently used in around 138 countries.5 They proposed surgical metrics designed specifically to capture facility-level data on structural capacity, process issues and outcomes. The Lancet Commission on Global Surgery has expanded upon these and developed six Lancet Indicators.6 Assessing surgical infrastructure and resources in developing countries is problematic as there are few electronic networks which allow data sharing and evaluation. Most studies performed in LMIC extrapolate data in order to calculate the numbers of operating theatres and other resources, as data collection efforts are labour intensive and expensive.
A template for a National Surgical Plan has been proposed and involves infrastructure (tracking number of facilities), workforce (density and distribution of surgical, anaesthetic and obstetric specialists), service delivery (Bellwether procedures), financing, and information management (robust information systems).6 Funk et al. estimated the global distribution of operating theatres by extrapolating data from 769 hospital profiles in 92 countries. They used linear regression models and estimates by WHO and World Bank to estimate economic, population and health data.7 They found that the total number of theatres was not publicly reported by each country. The proportion of operating theatres without pulse oximetry in Africa was between 51% and 70%, and in addition to the lack of monitoring and basic supplies, there was a lack of physical space equipped for surgery.
Surgical resources in South Africa
South Africa had an estimated population of 54 million inhabitants in 2014.8 The World Bank has designated South Africa an upper-middle (ring and cross-refunt to UMIC) with a GDP of 6 619 $US per capita.9 There are nine provinces which are divided into metropolitan and district municipalities, which district municipalities, wi are further divided into local municipalities. The nine provinces are: the Eastern Cape (EC), the Free State (FS), Gauteng (GP), KwaZulu-Natal (KZN), Limpopo (LP), Mpumalanga (MP), North West (NW), the Northern Cape (NC) and the Western Cape (WC).10
As a result of years of oppression and segregation, many South Africans are still suffering the consequences, resulting in poor access to safe and affordable health care. Slow service delivery is problematic and many South Africans in rural areas migrate to urban areas in search of basic treatments. Public hospitals are classified as district, regional, central (includes tertiary) and specialised according to the National Health Act of 2003.11 Private hospitals are largely managed as for profit hospitals and are accessible to those who are able to afford health insurance, which comprises 16% of South Africans.12 Few South African studies have looked at the burden of surgical disease or at existing surgical infrastructure.
Materials and methods
Study design and data collection
The study is a descriptive analysis of operating theatre density in South Africa. It documents the number of functional operating theatres in all provinces and in both sectors. All public and private hospitals were contacted telephonically and via email, and were requested to provide the number of functional operating theatres in use at the time. There was a 100% response rate for all hospitals. Public hospitals included all district, regional and central hospitals. Clinics and so-called specialised hospitals such as psychiatric, tuberculosis and rehabilitation facilities were excluded. It was assumed that limited surgery or no surgery was being conducted at these facilities. Private facilities that performed day theatre cases were included unless they strictly performed obstetric or orthopaedic procedures. A list of all hospitals in South Africa was obtained from the Department of Health and cross-referenced with electronic databases of hospitals in South Africa (Medpages and hospital websites). Hospitals were contacted during the period 1 October 2014 to 31 December 2014. Private hospital data was available from the Hospital Association of South Africa (HASA).
Variables and characteristics measured
The number of functional operating theatres was documented for each facility. Operating theatres which were not in use were excluded. These were reported to be non-functional for largely equipment and staffing reasons. This data was captured as part of a larger study which assessed several other instances of surgical infrastructure and human resources, which meant that in-depth validation of functionality was not performed.
Data Analysis
The captured variables were entered into a Microsoft Excel (2013) spreadsheet. Population data was obtained from the Statistics South Africa (Stats SA) website.8 The number of functional operating theatres per 100 000 people was calculated for each province and district. In order for an accurate comparison to be made, public sector resources were calculated per uninsured population, and private sector resources were calculated per insured population. Private access was not strictly confined to insured patients, as out-of-pocket payments from uninsured patients were common. Permission to conduct research was obtained from the Department of Health in each province as well as individual hospitals. This research was approved by the Human Research and Ethics Committee at the University of Cape Town. (HREC 515/2013, 515/2014, 515/2015). Departmental Research Council for the Department of Surgery was obtained. There were no conflicts of interest.
Results
Number of Operating theatres
There were 544 hospitals, of which 217 were private hospitals and 327 were public hospitals. Of the 327 public hospitals, 257 (79%) were district level hospitals, 49 (15%) were regional hospitals and 21 (6%) were central/level three hospitals. District hospitals had one functional operating theatre on average, regional hospitals had five functional operating theatres and the central hospitals had 13 functional operating theatres.
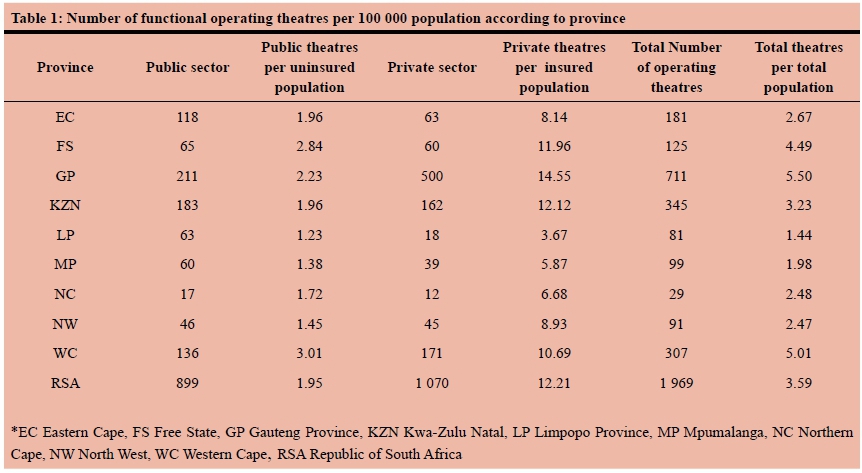
There was a total of 1 969 functional operating theatres in South Africa, with 54% of these in the private sector and 46% in the public sector (Table 1). The fewest functional theatres per total population were in Limpopo (1.44 per 100 000), whereas the most were in Gauteng (5.5 per 100 000) and the Western Cape (5.01 per 100 000). Overall, South Africa had a functional theatre density of 3.59 per 100 000 total population. Of the 899 operational theatres in the public sector, fewest were in the Northern Cape (n=17) and most were in Gauteng (n=211). Similarly, the fewest private theatres were found in Northern Cape (n=12) and most in Gauteng (n=500).
A more accurate comparison was performed between sectors when insured versus uninsured population were assessed. There were 1.95 operating theatres per 100 000 uninsured population in the public sector compared with 12.21 operating theatres per 100 000 insured population in the private sector.
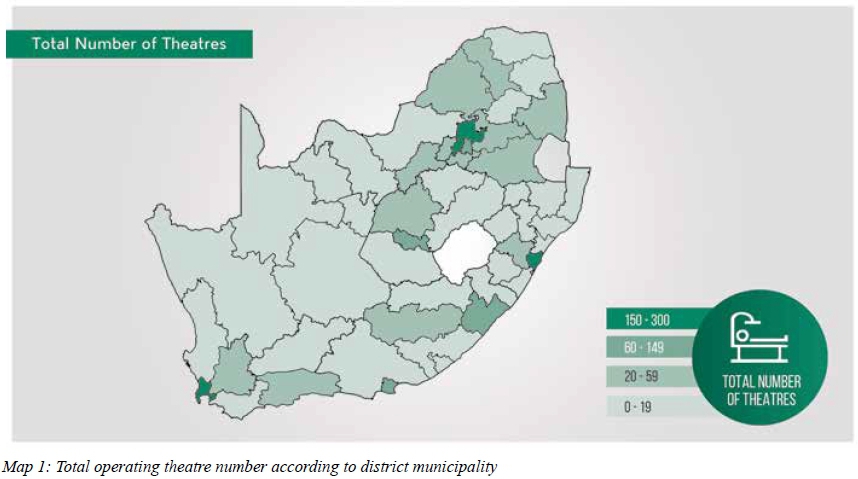
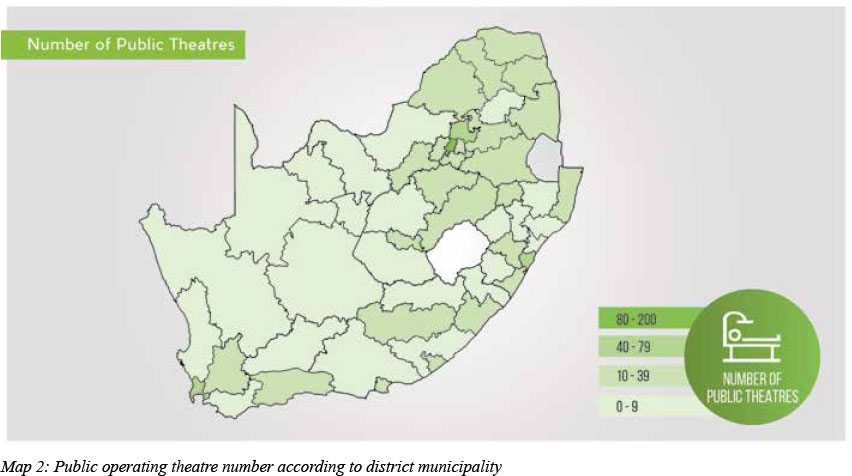
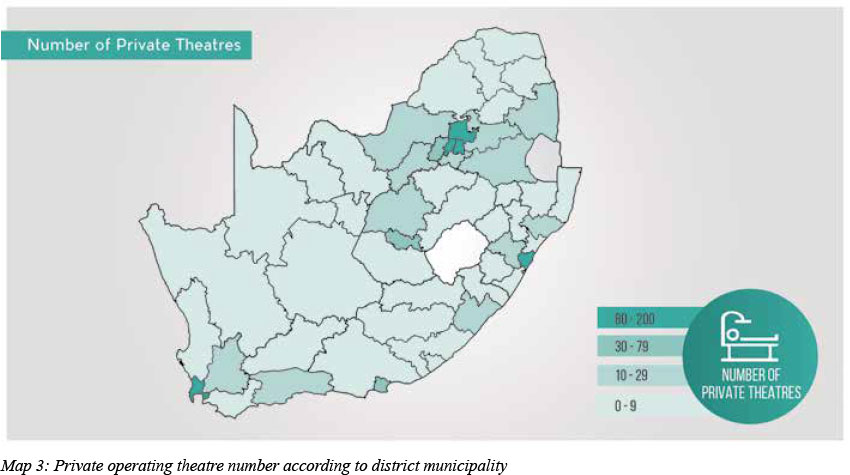
Map 1 demonstrates the total number of operating theatres according to district municipality. Maps 2 and 3 demonstrate the number of public and private operating theatres according to district municipality, respectively.
Discussion
Functional operating theatre density in South Africa
Operating theatre density has been used as an indicator of provision of surgical care. There were 1 969 functional operating theatres in South Africa. The actual theatre number was over 2 000, but a number of theatres were not being utilised for a variety of reasons. The majority of non-functional theatres were located at district level hospitals in EC and KZN. Common reasons for non-use included: lack of theatre staff (nurses, anaesthetists and surgeons), non-functional anaesthetic machines or lack of surgical supplies. A district facility which had two theatres but only utilised one would be reported as having one functional operating theatre. As no formal checklist was used to verify functionality, this was a limitation and affected data validity. No hospitals reported lack of infrastructure such as water or oxygen. It was found, particularly at district level, that inexperienced anaesthetists and surgeons were unable to safely perform surgery or there were no recovery nurses available. In addition, most district level hospitals did not have functional anaesthetic machines, and were only performing spinal anaesthesia for cases such as caesarean sections. Reinstating public operating theatre function could be used to improve theatre numbers through the use of existing infrastructure, thereby avoiding the added expense.
Private hospitals are an important part of the South African health care system, although few people have health insurance. The largest number of medical aid beneficiaries reside in GP (26.6%), followed by WC (25.5%) and FS (18%) and the majority of private facilities are located in these metropoles.12 These areas contain nearly 70% of all functional operating theatres. This may offer an explanation as to why people migrate to large cities in search of surgical care which may be perceived to be superior in the private sector. This further compounds inaccessibility and escalating costs of surgical treatment. The largest number of private operating theatres were owned by Netcare (30%), Life Hospital group (26.7%) and Mediclinic (22.8%).
Funk et al. estimated that Southern sub-Saharan Africa had 3.1 operating theatres compared to the current data which demonstrated 3.59 functional operating theatres per 100 000.7 There were 1.95 operating theatres in the public sector compared 12.21 theatres in the private sector per 100 000 population. The WC, GP, FS and KZN had greater than 10 private operating theatres per insured population, which was comparable with HICs (10-25 theatres per 100 000).7 Private sector theatre density was greater than the global average (6.2 per 100 000) in nearly all provinces apart from LP and MP. These provinces also had the lowest medical aid coverage in South Africa.12 Funk et al. demonstrated that LICs, which comprise more than 2 billion people, had far fewer operating theatres (1-1.3 per 100 000) despite the high burden of surgical disease. In South Africa, public sector theatre density was similar to LICs in most provinces and below the global average in all provinces. This highlighted inequitable access to operating theatres between health sectors and in turn, access to surgical care.
A global recommendation for the optimal number of operating theatres is currently lacking, partly due to the fact that theatre density alone does not equate to surgical outputs. Weiser et al. showed that a disproportionately low volume of surgeries were being performed in LICs.13 With there being fewer operating theatres in developing countries such as South Africa, and in particular the public health sector, it is expected that fewer surgeries are being performed. This negatively impacts access to surgical care and ultimately health outcomes.
The private hospital business model generates income only when a theatre is in use. Utilisation is therefore a simple measure of the efficiency of a theatre, because its ability to generate revenue rises as its use increases.14 Internationally, it is agreed that theatres are unable to run at 100% capacity and that a 70-80% utilisation is realistic.15,17 Although nearly all private theatres were reportedly being used, this is likely to be an overestimation. Most public hospital theatre lists have long waiting periods, whereas the perception exists that private theatres are being under-utilised. There appears to be limited published research providing utilisation benchmarks for South African private operating theatres, however one descriptive study showed that theatre utilisation in a single private hospital was higher (48%) than was observed in public institutions.14 Van As et al. estimated theatre utilisation in South African public hospitals to range between 30% and 40%.18 Measuring actual surgical volumes and utilisation rates in all hospitals would be needed in order to verify surgical capacity and efficiency.
Conclusion
This study provided an assessment of existing theatre density, although analysis of infrastructure alone may not assess theatre function. Running water, the continuous supply of oxygen, pulse oximetry and theatre staff are all essential components of functional operating theatres, hence a closer look at national theatre utilisation would be more appropriate. Van As et al. have recommended aligning theatre demand and supply, ensuring staff availability, maximising theatre utilisation, optimising patient selection and surgical bed utilisation in order to improve theatre management.14 District theatre accreditation is a means of utilising existing infrastructure rather than acquiring new surgical resources. The WHO GIEESC tool is an accurate means of assessing theatre functionality and should be carried out by all theatre complexes in order to identify deficiencies. Data from the South African Surgical Outcomes Study (SASOS) proposed health budget reallocation towards identifying and managing potential surgical pathologies at district level as well as providing sufficient surgical and critical care services at higher levels in order to improve surgical outcomes.19 This requires addressing gaps in infrastructure, personnel and equipment.
Acknowledgements
Faculty of Health Sciences, University of Cape Town. Images courtesy of Ms. Alicia Nicola.
REFERENCES
1. Ozgediz D, Jamison D, Cherian M, McQueen K. The Burden of surgical conditions and access to surgical care in low- and middle-income countries. Bull World Health Organ. Aug 2008;86(8):646-7. Available from: doi: 10.2471/BLT.07.050435 PMID: 18797625 PMCID: PMC2649455 [ Links ]
2. Bickler S, Ozgediz D, Gosselin R, Weier T, Spiegel D, Hsia R, Dunbar P, Mcqueen K et al. Key concepts for estimating the burden of surgical conditions and the unmet need for surgical care. World J Surg. 2010;34:372-80. Available from: doi: 10.1007/s00268-009-0261-6 [ Links ]
3. Luboga S, Galukande M, Mabweijano J, Ozgediz D, Jayaraman S. Key aspects of Health Policy Development to Improve Surgical Services in Uganda. World J Surg. 2010;34:2511-7 Available from: doi 10.1007/s00268-010-0585-2 [ Links ]
4. Ozgediz D, Riviello R. The "other" neglected diseases in global public health: surgical conditions in sub-Saharan Africa. PLoS Med. 2008;5(6):e121. Available from: http://dx.doi.org/10.1371/journal.pmed.0050121 [ Links ]
5. World Health Organization. WHO meeting towards a Global Initiative for Emergency and Essential Surgical Care (GIEESC), summary report. 8-9 Dec 2005, Geneva, Switzerland. Available at: http://www.who.int/surgery/mission/GIEESC2005_Report.pdf [ Links ]
6. Meara, J, Hagander, L, and Leather, A. Surgery and global health; a Lancet Commission. Lancet. 2014;383(9911):12-3. Available from: doi: http://dx.doi.org/10.1016/S0140-6736(13)62345-4 [ Links ]
7. Funk L, Weiser T, Berry W, et al. Global operating theatre distribution and pulse oximetry supply: an estimation from reported data. Lancet. 2010;376:1055-61. Available from: doi: 10.1016/S0140-6736(10)60392-3 [ Links ]
8. Statistics SA Annual 2013/2014 report. Available from: www.statssa.gov.za [ Links ]
9. South African overview - World Bank. Available from: www.worldbank.org [ Links ]
10. http://www.southafrica.info/about/government/govprov
11. National Health Act, No 61 of 2003. Government Gazette. 655(34521). 12 Aug 2011. Government Notice no. 655. Cape Town. Government Printer. [ Links ]
12. Matsebula T, Willie M. Private hospitals. In: Harrison S, Bhana R, Ntuli A, eds. South African Health Review. Durban: Health Systems Trust. 2007;Chapter 11:159-64. [ Links ]
13. Weiser TG, Regenbogen S, Thompson K, Haynes AB, Lipsitz S, Berry W, Gawande A. An estimation of the global volume of surgery: A modelling strategy based on available data. Lancet. 12 Jul 2008;372(9633):139-44. Available from: doi 10.1016/S0140-6736(08)60878-8. Epub 2008. [ Links ]
14. Hartman D, Sunjka B. Private theatre utilisation in South Africa: A case study. S Afr Med J. 2013(accessed on 24 Jan 2018);103(5):285-7. doi: 10.7196/SAMJ.6460 [ Links ]
15. NHS Institute. The productive theatre - improving quality and efficiency in the operating theatre. Accessed on 24 Dec 2017. Available from: http://www.institute.nhs.uk/quality_and_value/productivity_series/the_productive_operating_theatre.html [ Links ]
16. Van Houdenhoven M, Hans EW, Klein G, et al. A norm utilisation for scarce hospital resources: Evidence from operating rooms in a Dutch university hospital. J Med Syst. 2007;31(4):231-6. Availble from: http://dx.doi.org/10.1007/s10916-007-9060-5 [ Links ]
17. Ballard SM, Kuhl ME. The use of simulation to determine maximum capacity in the surgical suite operating room. Proceedings of the 2006 Winter Simulation Conference, 3-6 Dec 2006. WSC 2006;433-438. Available from: http://dx.doi.org/10.1109%2FWSC.2006.323112 [ Links ]
18. Van As AB, Brey Z, Numanoglu A. Improving operating theatre efficiency in South Africa. S Afr Med J. 2011;101(7):444-8. [ Links ]
19. Biccard B, Madiba T. Surgical outcomes study investigators, on behalf of the South African. The South African Surgical Outcomes Study: A 7-day prospective observational cohort study. S Afr Med J. 2015(accessed on 24 Jan 2018);105(6):465-75. doi:10.7196/SAMJ.9435 [ Links ]
 Correspondence:
Correspondence:
Dr AJ Dell
angelajdell@gmail.com


{kind=link}
{kind=link}
{kind=link}
{kind=link}