










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.56 no.2 Cape Town Jun. 2018
http://dx.doi.org/10.17159/2078-5151/2018/v56n2a2351
VASCULAR SURGERY
Association between crural vessel patency and successful transmetatarsal amputation: a single centre experience
Dariush Kamali; Matthew Thomas; Peter van Loo; Ian Nichol
Department of General & Vascular Surgery, James Cook University Hospital, Middlesbrough, United Kingdom
ABSTRACT
BACKGROUND: Transmetatarsal amputation (TMA) has a reputation for failure, centred around wound breakdown. No study has looked at the direct association between the patency of individual crural arteries and the healing of TMA. TMA relies on a posterior skin flap which derives its blood supply from the posterior tibial (PT) artery. We investigated the association between PT patency and achievement of successful TMA.
METHODS: A retrospective review of all patients undergoing TMA for complications of peripheral arterial occlusive disease in a regional vascular tertiary referral centre over a 9 year period (2006-2015). TMA was considered successful by the absence of a higher-level amputation. Follow-up was for a minimum of 12 months.
RESULTS: 24 patients (21 male; mean age 64 years) were studied. TMA was successful in 16 (67%). On statistical analysis, successful TMA was not significantly associated with vessel patency in either superficial femoral artery (SFA), or any single or combination of named crural artery.
CONCLUSION: TMA healing can be achieved in the absence of a patent posterior tibial artery. We support the role of TMA in selected patients, given its benefits compared to transtibial amputation.
Keywords: Transmetatarsal amputation - Diabetes Mellitus - Crural artery - Angioplasty
Background
When used appropriately in the control of distal tissue loss and spreading foot sepsis, transmetatarsal amputation (TMA) offers the chance to maintain independent ambulation, avoiding the need for a prosthesis and allowing the patient to use "normal" footwear.
The procedure was first described as a method of partial foot preservation by McKittrick et al. in 1949.1 Despite such an established history, TMA wounds remain notoriously difficult to heal, with case series reporting wound failure rates of between 40-70%.28 Wound failure following TMA results in the need for further surgery in many patients, and can ultimately lead to transtibial or transfemoral amputation.
There have been several studies attempting to predict the factors that may lead to non-healing following TMA, but no specific factors have yet been shown definitively to promote TMA success. Tight blood glucose control as measured by HbA1c levels has been shown to predict successful TMA by Younger et al.,9 whilst Kono et al. found the presence of insulin-dependent diabetes to be associated with the need for re-amputation within 6 months of TMA.10 However, other studies have shown no association between diabetes and successful TMA healing.11,12
In a study of all major lower limb amputations that included above-knee, below-knee and transmetatarsal amputations, end-stage renal failure has been shown to predict early amputation failure.13 The same study also found other patient factors including that of a Body Mass Index (BMI) of greater than 30 and on-going patient tobacco use were predictors of early amputation failure.13 This link to tobacco use has been supported by Nguyen et al. who found that tobacco use of greater than 20 years pre-TMA was a significant predictive factor for non-healing.4
Anatomically, the documented presence of a clinically palpable pedal pulse on examination before TMA has also been found to predict successful healing post-TMA.7 Furthermore, the TMA procedure itself requires the formation of a plantar skin flap, whose main blood supply is derived from the posterior tibial artery. To our knowledge, no study has looked at the direct association between the patency of crural arteries confirmed by radiological imaging and the healing of TMA. Our primary outcome measure aimed to investigate association between posterior tibial artery patency and the achievement of successful TMA. Our secondary outcome measure investigated if there was association between patency of any crural artery and the achievement of successful TMA.
Patients and methods
All patients undergoing TMA for complications of peripheral arterial occlusive disease (PAOD) in a regional vascular tertiary referral centre over a 9-year period (2006-2015) were identified from the hospital's coding system. A retrospective review of patients' paper-based case notes and an electronic radiology imaging and reporting system (Infinitt Picture Archiving and Communication System) was performed. Demographic data including age, sex and co-morbidities was collected.
Data on crural artery status was also collected. Crural artery assessment - anterior tibial (AT), posterior tibial (PT) or peroneal (P) artery - was performed pre-operatively in all patients using either intra-arterial catheter angiography, computer-assisted tomography (CTA) or magnetic resonance angiography (MRA). All images were discussed at a specialist vascular multidisciplinary team meeting (MDT). Crural artery patency was considered satisfactory where at least one crural artery was seen to cross the ankle joint and in addition, where no further crural artery angioplasty was considered necessary by the MDT to further improve run-off. Where this was not the case, and the MDT considered it technically possible, revascularisation via angioplasty was performed by one of 3 consultant interventional radiologists before proceeding to TMA, in order to achieve satisfactory pre-operative crural artery patency and in-line flow.
TMA procedures were performed by one of 4 consultant vascular surgeons. TMA was considered successful where the patient did not require a further higher-level amputation. Patients were followed up for a minimum of 12 months.
Statistical analysis of those factors affecting TMA success was performed using a statistical software package (SPSS - Statistical Package for Social Sciences, IBM, New York, USA). Categorical variables were compared using the Pearson Chi-squared or Fisher Exact test, as appropriate. The level of significance was set at p < 0.05.
Results
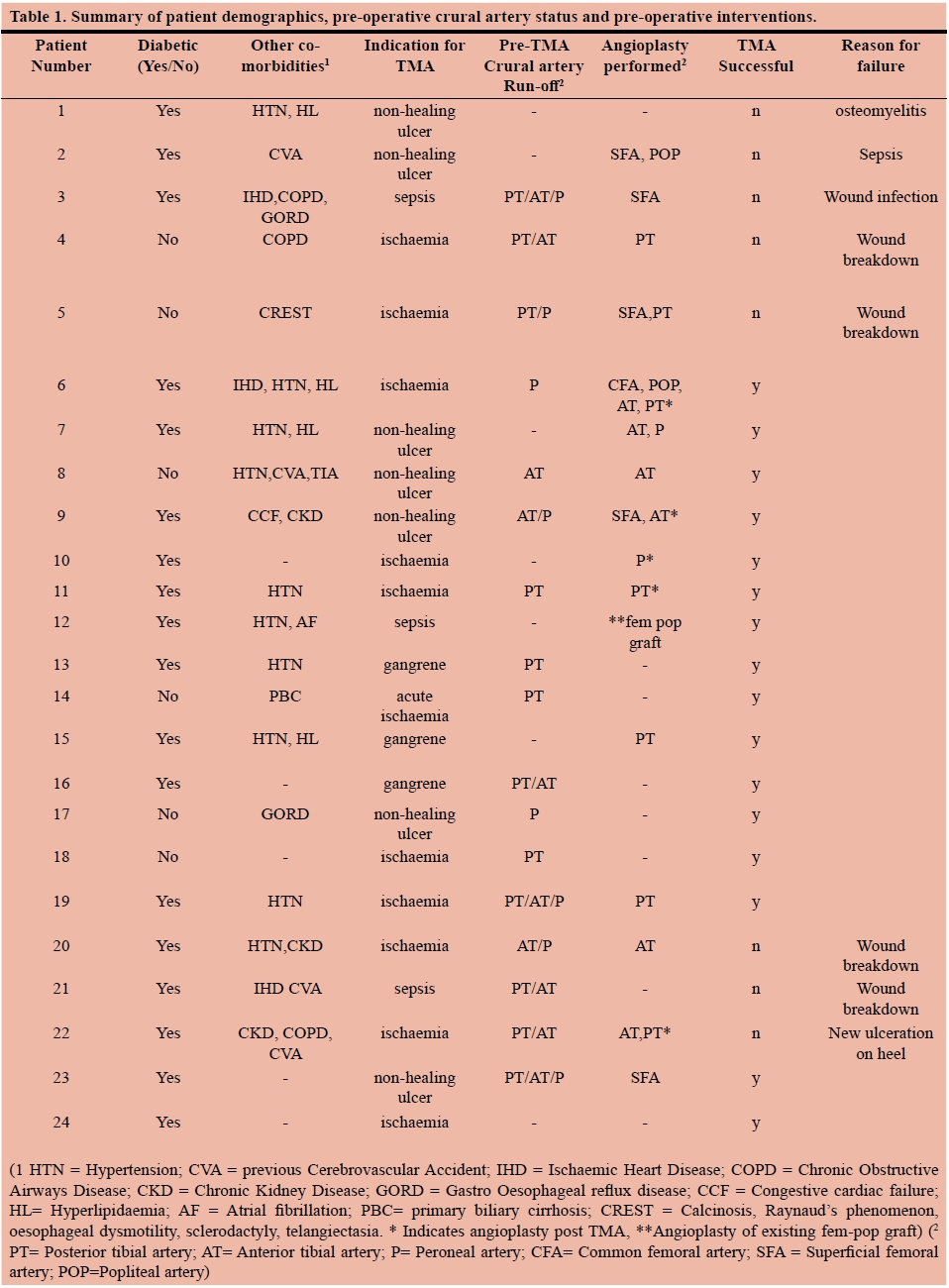
A total of 24 patients underwent TMA between October 2007 and April 2015. One patient died from pneumonia within 30 days of the procedure, and was therefore excluded from the analysis. Overall success of TMA was 67% (n = 16). Mean patient age was 64 years (range 29-76), with 21 males to 3 females. Table 1 summarises individual patient co-morbidities, pre-operative crural artery run-off and pre-operative crural artery interventions.
On pre-operative imaging, 8 patients were considered to have satisfactory crural artery patency without the need for further intervention. TMA was considered successful in 6 of these patients. A further 12 patients had at least one crural artery crossing the ankle on pre-TMA imaging, but went on to have pre-operative crural artery angioplasty to further improve run-off due to the presence of crural artery stenoses (PT treated in 5 patients, AT & PT treated in 2 patients, AT & P in 2 patients AT alone treated in 3 patients, P alone in 1 patient). Eight of these patients achieved successful TMA.
On their pre-operative imaging, 7 patients had no crural run-off crossing the ankle at all. Three (3) of these patients were deemed suitable by the MDT for pre-TMA crural artery angioplasty alone - P treated in 1 patient, PT treated in 1 patient, AT and P both treated in 1 patient. TMA was successful in 4 of these patients.
In addition to crural artery disease, 6 of the 24 patients also had superficial femoral artery (SFA) disease treated via SFA angioplasty; 3 of these 6 patients had both SFA and crural artery angioplasty. TMA failed in 3 out of these 6 patients. A further patient had angioplasty of an existing femoral-popliteal bypass graft which resulted in a successful TMA. On statistical analysis, successful TMA was not significantly associated with satisfactory vessel patency in SFA, any single crural artery or combination of vessels.
Of the 8 TMAs that were not considered successful, 7 went on to require a below knee amputation; the remaining patient was planned for a below knee amputation but died before the amputation was performed. The reasons for TMA failure can be found in Table 1. Twelve (12) of the 16 successful TMAs were achieved in diabetic patients, with 6 of the 8 failed TMAs occurring in diabetics. Two (2) failed TMAs occurred in a patient with chronic kidney disease. Neither diabetes nor chronic kidney disease was independently associated with TMA failure on statistical analysis.
Discussion
TMA requires the formation of a posterior skin flap that derives its blood supply from the PT artery. We therefore sought to investigate any potential association between crural artery patency and successful TMA, with a hypothesis that the presence of a patent PT artery crossing the ankle joint would be essential for a successful TMA. However, our results showed that no named crural artery was significantly associated with successful TMA, and that TMA can be achieved in the absence of a patent posterior tibial artery crossing the ankle joint. Furthermore, the fact that there was no positive association between angioplasty of any vessel and wound healing, we would advocate from our results that TMA could be considered without prior crural angioplasty, thereby eliminating the embolisation risk associated with this procedure.
Other parameters that may help to predict wound healing following TMA include measurement of toe pressures, and transcutaneous oxygen pressures (TcPO2). Toe pressures of greater than 50 mmHg in the diabetic sub-group have been shown to have a positive predictive value of 91% in determining successful TMA wound healing.13 A specificity and sensitivity of 71% in the prediction of partial wound foot amputation healing or failure has been shown with a "cut point" transcutaneous oxygen tension of 38 mmHg.14 Data on toe pressures and TcPO2 were not available in our study as neither parameter is routinely measured in our institution.
Limb salvage rates as high as 96.5% have also been reported when managing moderate to severe diabetic foot infections in the presence of at least one palpable pedal pulse, without attempts at revascularisation.15 Although diabetes was not shown to be a factor in wound breakdown in our study, we are unable to comment of the potential predictive effect of a palpable pedal pulse on TMA wound healing, as due to the retrospective nature of our study the necessary data was incomplete.
Whilst early revascularisation (< 30 days pre-amputation) has previously been shown to optimise wound healing in patients requiring minor lower extremity amputation (including TMA),2 we have failed to identify an association between any one specific vessel and successful TMA. This supports the work of Toursarkissan et al. who found no angiographic features that were predictive of limb salvage following TMA.5 TMA healing therefore seems to be a multifactorial process, which may be dependent on other patient-specific variables outside of the TMA's vascular supply, such as smoking history, tight glycaemic control and the presence of renal insufficiency, although this was not evident in our study.4,9,16 Nevertheless, our healing rates of 67% are favourable compared to some of the literature. Thus, we support the role of TMA in selected patients, even in those without a named crural artery or vessels not suitable for angioplasty, given its aforementioned benefits compared to trans tibial amputation.
Limitations of this study
Our study is limited by the small number of patients included for analysis, despite the 9-year review period, and by the retrospective nature of the data collection. Our small sample size may lead to the possibility of a type II error. However, the reality of a small number of patients receiving TMA at a major vascular centre in the North of England over a 9-year period may reflect a decrease in the popularity of the procedure, which may translate to other vascular centres, given the perceived problems with TMA wound healing.
Conclusion
Transmetatarsal amputation can be a successful operation despite the absence of a named crural vessel depicted on angiography. This offers the patient a chance to maintain independent ambulation and avoid the need for a prosthesis compared to transtibial or transfemoral amputation.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
REFERENCES
1. McKittrick LS, McKittrick JB, Risley TS. Transmetatarsal amputation for infection or gangrene in patients with diabetes mellitus. Ann Surg. 1949;130:826-40. [ Links ]
2. Sheahan MG, Hamdan AD, Veraldi JR, et al. Lower extremity minor amputations: The roles of diabetes mellitus and timing of revascularisation. J Vasc Surg. 2005;42:476-80. [ Links ]
3. Stone PA, Back MR, Armstrong PA, et al. Midfoot amputations expand limb salvage rates for diabetic foot infections. Ann Vasc Surg. 2005;19:805-11. [ Links ]
4. Nguyen TH, Gordon IL, Whalen D, et al. Transmetatarsal amputation: predictors of healing. Am Surg. 2006;72:973-77. [ Links ]
5. Toursarkissian B, Hagino RT, Khan K, et al. Healing of transmetatarsal amputation in the diabetic patient: is angiography predictive? Ann Vasc Surg. 2005;19:769-73. [ Links ]
6. Mwipatayi BP, Naidoo NG, Jeffery PC, et al. Transmetatarsal amputation: three-year experience at Groote Schuur Hospital. World J Surg. 2005;29:245-8. [ Links ]
7. Pollard J, Hamilton GA, Rush SM, et al. Mortality and morbidity after transmetatarsal amputation: retrospective review of 101 cases. J Foot Ankle Surg. 2006;45:91-7. [ Links ]
8. Thomas SR, Perkins JM, Magee TR, et al. Transmetatarsal amputation: an 8-year experience. Ann R Coll Surg Engl. 2001;83:164-6. [ Links ]
9. Younger AS, Awwad MA, Kalla TP, et al. Risk factors for failure of transmetatarsal amputation in diabetic patients: a cohort study. Foot Ankle Int. 2009;30:1177-82. [ Links ]
10. Kono Y, Muder RR. Identifying the incidence of and risk factors for reamputation among patients who underwent foot amputation. Ann Vasc Surg. 2012;26:1120-6. [ Links ]
11. Yeager RA, Moneta GL, Edwards JM, et al. Predictors of outcome of forefoot surgery for ulceration and gangrene. Am J Surg. 1998;175:388-90. [ Links ]
12. Landry GL, Silverman DA, Liem TK, et al. Predictors of healing and functional outcome following transmetatarsal amputations. Arch Surg. 2011;146:1005-9. [ Links ]
13. Stone PA, Back MR, Armstrong PA, Flaherty SK, Keeling WB, Johnson BL, et al. Midfoot amputations expand limb salvage rates for diabetic foot infections. Ann Vasc Surg. 2005;19:805-11. [ Links ]
14. Andrews KL, Dib MY, Shives TC, Hoskin TL, Liedl DA, Book AJ. Noninvasive arterial studies including transcutaneous oxygen pressure measurements with the limbs elevated or dependent to predict healing after partial foot amputation. Am J Phys Med Rehabil. 2013;92:385-92. [ Links ]
15. Aragon-Sanchez J, Lazaro-Martinez JL, Hernandez-Herrero C, Campillo-Vilorio N, Quintana-Marrero Y, Garcia-Morales E, et al. Surgical Treatment of limb- and life-threatening infections in the feet of patients with diabetes and at least one palpable pedal pulse: successes and lessons learnt. Int J Low Extrem Wounds. 2011;10:207-13. [ Links ]
16. O'Brien PJ, Cox MW, Shortell CK, et al. Risk factors for early failure of surgical amputations: an analysis of 8,878 isolated lower extremity amputation procedures. J Am Coll Surg. 2013;216:836-42. [ Links ]
 Correspondence:
Correspondence:
Mr Dariush Kamali
dariush.kamali@nhs.net


{kind=link}