








Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.55 n.4 Cape Town Nov. 2017
GENERAL SURGERY
Does the reporting of gastro-intestinal endoscopy meet the minimal terminology standard at King Edward VIII Hospital?
S P MaharajI; M A NoorbhaiI; T E MadibaI, II
IDepartment of Surgery, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban
IIGI Cancer Research Centre, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban
ABSTRACT
BACKGROUND: The Minimal Standard Terminology (MST) was developed to standardise endoscopic reporting. This study is aimed at assessing current reporting at a tertiary hospital and whether it meets this Minimal Standard Terminology.
METHODS: This was a retrospective observational study of upper endoscopy reports between January and December 2014. The data extracted were compared to the current reporting standard listed in the MST. To assess and grade the quality of reporting we developed a Gastrointestinal Reporting Score, which incorporates MST variables in addition to demographic details, indication for endoscopy, report legibility, sedation and the use of classification systems to describe pathology. Variables were classified as blank, partially complete or complete and assigned a score of 1-3. The reports were graded according to their overall score for all variables (Max 40) into Grade A (> 36), B (28-36) and C (< 28).
RESULTS: There were 100 patients of which 58 were female. Thirty-seven per cent were from the 60-75 year age group. Fifty-four endoscopies were performed by trainee specialists. Junior and senior consultants performed 36 and 9 upper endoscopies respectively. Indications for upper endoscopy were stated in 51 reports. The use of pre-procedural sedation was not stated in 51 reports. Four reports were illegible; one was conducted by a junior consultant, two by a fourth year trainee specialist and one by an unknown endoscopist whose name was illegible. Common classification systems for oesophagitis, gastropathy features, ulcer characteristics, and ulcer location are not routinely used. Based on the Gastrointestinal Reporting Score there were no Grade A reports, 16 Grade B and 84 Grade C reports.
CONCLUSION: The MST is not routinely utilised in our setting and reports are incomplete. There is a need for optimal upper endoscopic reporting, incorporating the MST guidelines.
Background
Non-structured handwritten or typed reports are not uniform amongst various endoscopists and may create confusion.1,2 There exists a plethora of endoscopy record systems worldwide which have not been standardised.3,4 This has led to the development of the Minimal Standard Terminology (MST) by the World Organisation of Digestive Endoscopy, whose objective was to put in place a "minimal" list of terms that could be included within a system used to record the results of a gastrointestinal endoscopic examination.1,2,4-6 A structured standardised method of endoscopic reporting would facilitate comparison and sharing of data from different Gastrointestinal (GI) Units1,2,7,8 and it would be easily adaptable to computerised reporting of endoscopy findings.7-9 We hypothesised that the current reporting of GI endoscopy is substandard. The aim of this study was to assess the current upper gastrointestinal reporting at a tertiary hospital in Durban and to assess if the current reporting meets the MST guidelines.
Methodology
Study setting
This retrospective study was conducted at King Edward VIII Hospital, a tertiary hospital in Durban, South Africa. It included all patients who had undergone upper endoscopy (oesophago-gastro-duodenoscopy) during the study period. The Gastrointestinal (GI) Unit receives either pre-booked elective patients or those with upper GI emergencies. Patient hospital numbers were retrieved from the existing GI unit filing system. This was then used to access each individual patient record from the hospital. The data were de-identified prior to assessment.
Study design
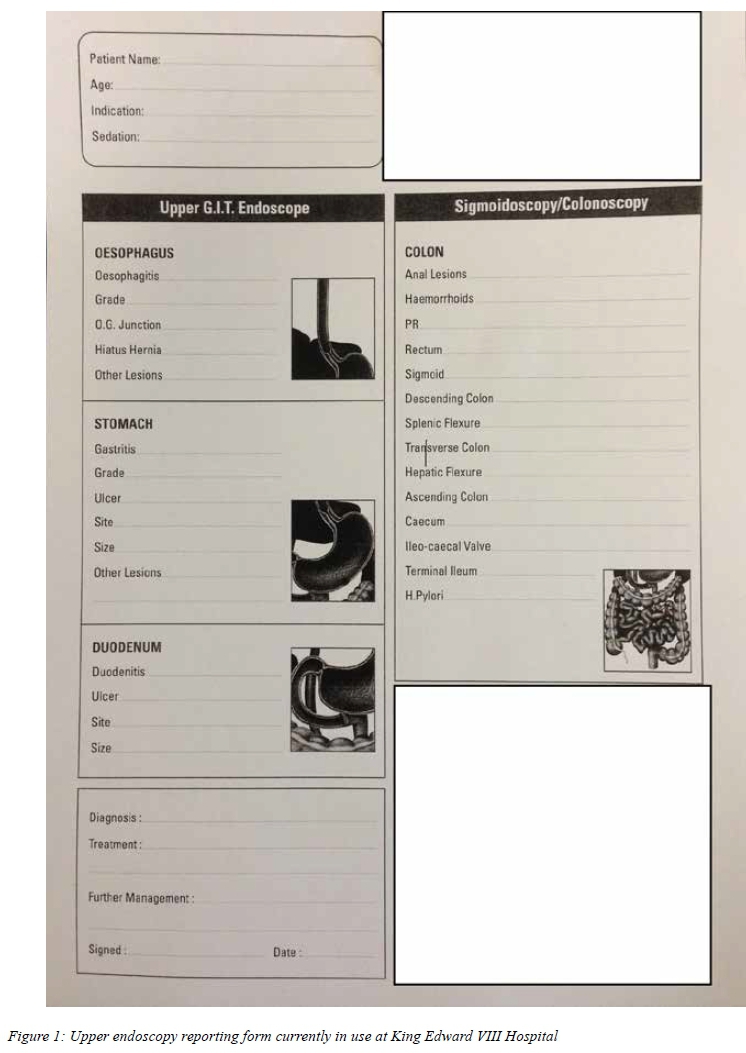
The study period was from 1 January 2014 to 31 December 2014. The variables were extracted from the existing upper GI reporting proforma (Figure 1). These included patient demographics, indication for endoscopy and use of sedation. The specific findings at oesophagoscopy, gastroscopy and duodenoscopy were also noted.
In addition, the study analysed the legibility of the handwritten report, level of experience of the endoscopist, use of known classification systems for various pathologies, procedures performed during the endoscopy and any omitted details. The authors used the Minimum Standard Terminology as the benchmark for endoscopic reporting and the variables extracted from the endoscopy reports were compared to the current reporting standard as listed in the MST version 3.0. The current MST 3.0 guidelines focus on anatomical structures, endoscopic findings and their characteristics, reasons for endoscopy, endoscopic diagnosis, endoscopic procedures and adverse events and takes into account the latest universally recognised and accepted classification systems.
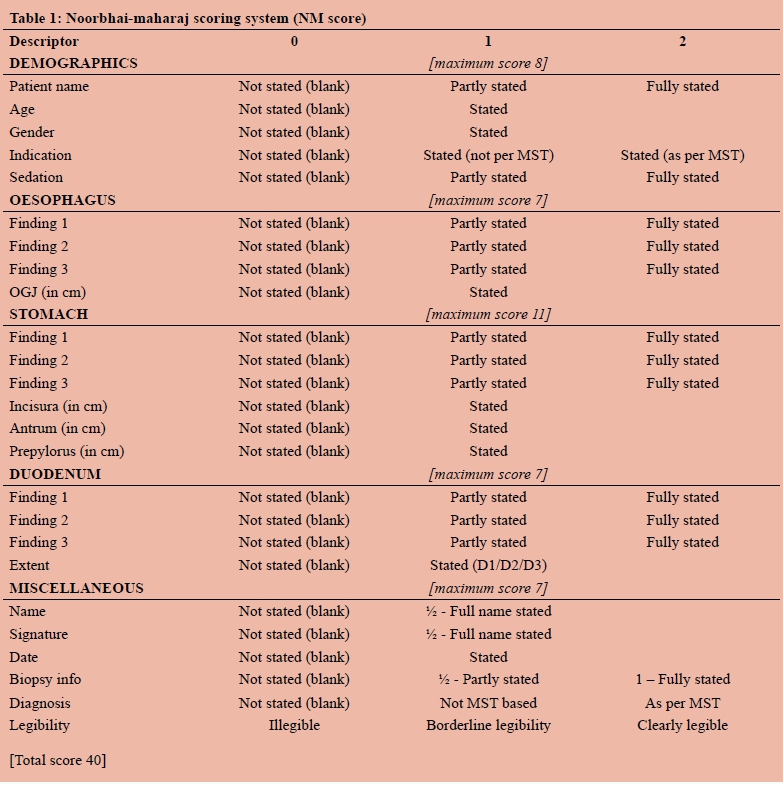
A Gastrointestinal Reporting Score was devised by the authors to assess the quality of reporting and is subsequently referred to as Noorbhai-Maharaj Score (NMS). In order to assess if reporting conformed to MST reporting, the score incorporated various variables listed in the MST. It also analysed the information under demographic details, indication for endoscopy, use of sedation as well as parts of the gastrointestinal tract (GIT) examined, namely oesophagus, stomach, duodenum as well as any other additional information. The reports were scored on whether the endoscopist recorded the date of report, indications for endoscopy, use of sedation, diagnosis, biopsy information, their name and signature. Legibility was graded as illegible, borderline, or clearly legible. Reports were given a score of zero (0) for a blank section, one (1) if partially stated and two (2) if fully stated. This is illustrated in Table I.
Provision was made in the NMS for findings in categories, namely demographics, the specific organs of the upper GIT (namely oesophagus, stomach and duodenum) and miscellaneous including diagnosis, name and signature of endoscopist as well as date and legibility. Reports were scored according to the detail of information supplied on the proforma as well as the knowledge and grading of relevant classifications systems. The score assessed the reporting of both negative and positive findings, comments on whether an action was undertaken or not and if known classification systems and specifics were used. It also assessed if a section was left blank or unstated, was partly stated or was fully stated. The score also assessed information with regard to biopsy of any abnormality. Provision was also made for endoscopist's name, signature, date, information regarding biopsy, diagnosis and legibility.
Maximum scores of8, 7, 11, 7 and 7 were given for 'Demographics', 'Oesophagus', 'Stomach', 'Duodenum' and 'Miscellaneous', giving a total of 40. The reports were graded according to their score into Grade A (> 36), B (28-36) and C (< 28).
Patients
A convenient sample of 100 patients was decided on for this preliminary study. The study period was 12 months from 1 January 2014 to 31 December 2014. Data were recorded on a custom-designed Microsoft Access database and were subsequently extracted into Microsoft Excel for analysis. Due to the predominantly qualitative nature of the study, a recognised statistical software package was not required.
Ethical considerations
The study was approved by the Biomedical Research Ethics Committee (BE 379/14) of the University of KwaZulu-Natal, Durban, South Africa.
Results
One hundred patients were included in the study of whom 58 were female. The average age was 52 years (median = 53; IQR 37-67, SD ± 18). The youngest patient was 15 years old and the oldest was 83 years old.
Indications
The indications for upper endoscopy were stated in 51 reports, including dyspepsia (22), heartburn (6), dysphagia (6), melaena (5), haematemesis (4), and abdominal pain (4). Patients with a recent endoscopic study (less than 6 weeks) who returned for a follow up endoscopy included a previous diagnosis of gastric ulcer (2), anaemia (1) and weight loss (1). Patients with no recent endoscopy with a past diagnosis included gastric ulcer (3), Gastro-Oesophageal Reflux Disease (3), and tumour/mass (2). Fifty-four endoscopies were performed by trainee specialists of whom 51 were 4th (final) year trainees and three were 3rd year trainees. Junior and senior consultants performed 36 and 9 upper endoscopies respectively. In one report, the endoscopist details were illegible.
Sedation and report legibility
Based on collateral information from nursing notes, none of the 100 patients were given sedation. Forty-nine reports stated that sedation was not used while in 51 reports this section was blank. Legible reports were seen in 96. The four illegible reports were conducted by a junior consultant (1), 4th year trainee specialist (2) and unknown endoscopist with illegible signature (1).
Endoscopic findings
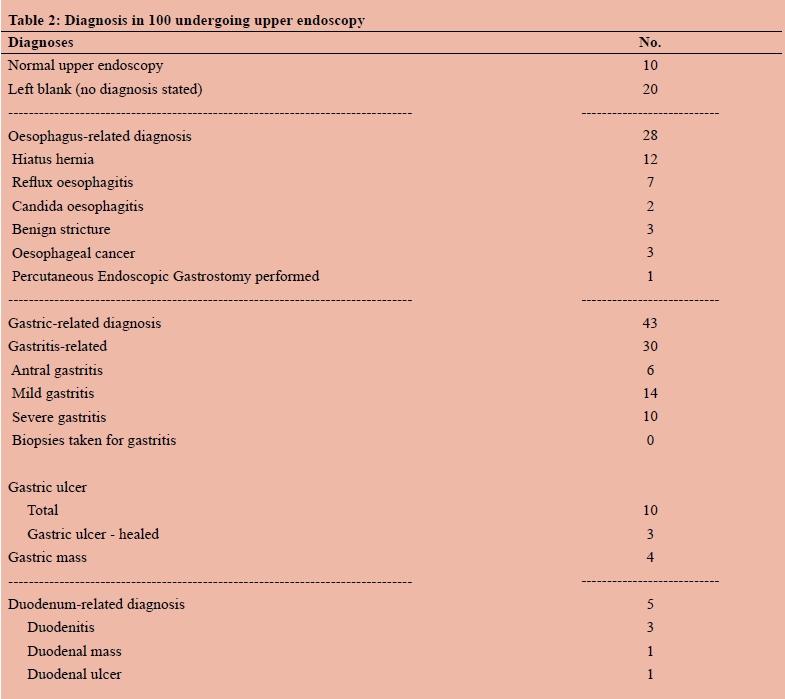
The various diagnoses made are shown in Table II. The oesophagoscopy, gastroscopy and duodenoscopy findings, reported in the GI record, are shown in Table III. The final diagnosis at endoscopy was reported as normal in 10 out of 100 patients and the final diagnosis was not given in 20 patients (i.e. the space was left blank). Oesophagus-related diagnoses were recorded in 28 patients, gastric-related diagnosis in 43 patients and duodenum-related diagnosis in 5 patients.
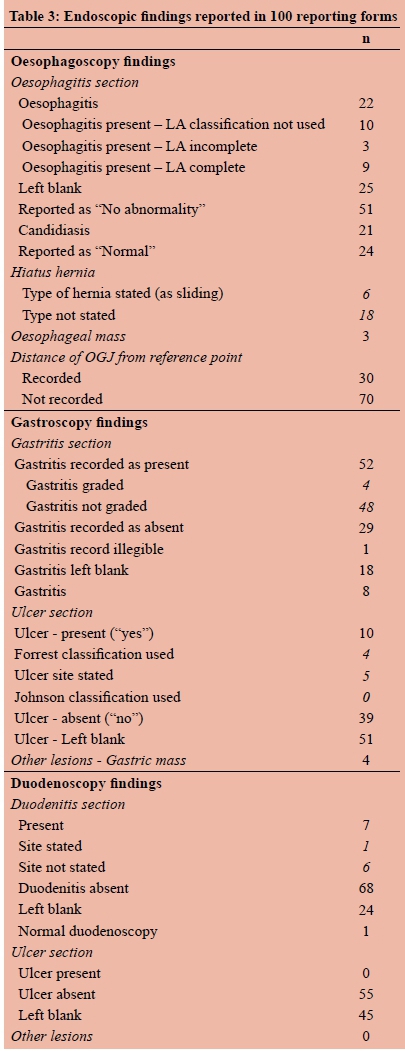
Thirty patients were said to have gastritis (antral gastritis 6, mild gastritis 14, and severe gastritis 10), none of whom had gastric biopsies taken. Gastric ulcers were seen in 10 patients none of which were bleeding. The Forrest classification was inappropriately applied in four of them. Biopsies were taken in six ulcers. There were no comments as to whether biopsies were taken in the remaining four ulcers. The site and number of biopsies were recorded in all four patients with gastric masses. With regard to the duodenum, the diagnoses made were duodenitis (3), duodenal mass (1), and duodenal ulcer (1). The latter diagnosis was strange since no patients were recorded as having "duodenal ulcer" in the duodenum section.
Treatment and Further management
The management section of the proforma, which was categorised into 'Treatment' and 'Further management' was also analysed. Findings under the "Treatment" section included 'Medication prescribed' (75), 'further investigations' (10), 'surveillance' (9) and spaces were left blank in 6 reports. Of the six blank "treatment" sections, the following data were recorded in the "Further management" section: 'repeat scope required' (2), required biopsy and result' (1), 'further investigations' (1) and blank spaces were left in 2 reports.
Noorbhai-Maharaj Reporting Score
The NMS was calculated on all reports. The maximum possible score is 40. There were no Grade A reports, 16 reports were graded as B, and 84 were graded as C. Scores less than 20 were seen in 60 reports.
Discussion
There is currently a lack of a universal reporting system in our setting. Reports are mostly in commercial-based proforma sheets and they are handwritten by endoscopists of different academic levels at the end of the procedure. This allows for the existence of poorly written and illegible reports. The current reporting system at the King Edward VIII Hospital's GI Unit falls into this category of reporting and assumes that the endoscopist is aware of all pertinent information relating to upper endoscopy including all grading systems and terminology for adequate reporting. The current MST 3.0 guidelines with respect to upper endoscopies focus on reasons for endoscopy, anatomical structures, endoscopic findings and their characteristics, endoscopic diagnosis, endoscopic procedures and adverse events. It also takes into account the latest universally recognised and accepted classification systems.
There were several areas that did not conform to the MST-based reporting system in this series. The indications were not routinely stated and, if they were, they were not based on the MST categories of either symptom or disease, for example, cholelithiasis. This, together with the fact that qualifiers for the indications such as duration and degree of the symptoms were not routinely reported and the use or omission of sedation was not routinely stated, suggest that endoscopists are not familiar with MST. The most common stomach finding amongst reports was gastritis. The MST 3.0 does not recognise gastritis as a diagnosis. Instead it recognizes various types of gastropathy which include portal gastropathy, hyperaemic, erosive, haemorrhagic, hypertrophic, NSAID-related and varioliform gastropathies.5 According to the Operative Link Gastric Assessment (OLGA) system of reporting, an initial diagnosis of a gastropathy is made at a stated site and is followed by histological confirmation of gastritis at that site. The term 'gastritis' therefore should be reserved for patients with histological confirmation.10,11 Accurate staging of the gastritis is fundamental in providing clinically relevant information on the overall status of the gastric mucosa with implications for prognosis, therapy and management.10 The challenge of the OLGA system is its requirement for a deep biopsy that includes the muscularis propria.11 Despite these limitations, the OLGA system provides significant clinically relevant information regarding the gastric mucosa.10 This was not the case in all reports in this study, and the use of this term as a diagnosis suggests lack of awareness of the use of the OLGA reporting system among endoscopists.
The Forrest classification was introduced to stratify patients with bleeding gastro-duodenal ulcers into high and low risk categories with regard to mortality12 as well as to identify patients at risk for re-bleeding thus assisting in further management.13,14 Scrutiny of reports in this study has identified inappropriate use of the Forrest classification by endoscopists to classify ulcers in patients who have no history of overt gastrointestinal bleeding. This casts doubt on the endoscopists' understanding of the relevance of this classification.
This study also revealed some apathy in reporting. The fact that some sections were left blank leaves one unsure if there was no abnormality or the parameter was not assessed at all. Leaving the endoscopic diagnosis blank and not commenting on planned management for the patients shows poor reporting with no attention to detail.
Knowledge of the MST 3.0 guideline reporting is beneficial to the qualified specialist because of the ability to align their reporting standards to that of MST 3.0, thus allowing them to compare data between GI Units. The benefit to the surgical trainee is the accurate reporting of their upper endoscopy experience which is a requirement for the Fellowship of the College of Surgeons of South Africa.15
This report assessment suggests that the current reporting can be improved. In contrast to the hand-written proforma-type reporting with a limited number of headings, the adoption of the more comprehensive MST reporting format will provide more accurate reporting and arm the endoscopist with the armamentarium to identify pathology more effectively. Reports with incomplete or blank sections can thereby be avoided. Furthermore, the MST is compatible with a computer-based reporting that can include more substantial information with drop-down menus.
The Noorbhai Maharaj Reporting Score was useful in this study in assessing and grading endoscopy reports. Its advantage is the fact that it will not change should MST 3.0 guidelines be amended or upgraded. This score can provide a framework for the improvement and monitoring of reporting of experienced endoscopists and trainees. This study does have limitations. It is retrospective and it was not possible to interrogate the endoscopists with regard to their thinking when they filled the forms incompletely. The heterogeneity of the data made it difficult to perform a simple analysis. Lastly, the numbers were too small to make a comparative analysis.
In conclusion, we have developed NMS which is an objective tool for assessing and grading upper endoscopy reports. It can be used by hospitals and GI units to assess and grade their reports and to compare these to the current MST 3.0 guidelines. This assessment has identified potential gaps in the existing endoscopic knowledge necessary to produce an optimal standard of reporting. It has also shown that MST is not routinely utilised in our setting. Reports were incomplete in the majority of cases. There is a need for optimal upper endoscopic reporting, incorporating the MST guidelines which reduces ambiguity and allows for cross-data analysis. A universal reporting system with standard terminology such as the MST guideline should be incorporated in gastrointestinal reporting in all hospitals in which upper gastrointestinal endoscopy is performed. This will help develop the knowledge base for specialists and trainee specialists alike.
Competing interests
The authors declare that they have no competing interests.
Notes relating to Noorbhai Maharaj score
Finding:
Not stated (Sections that are blank or not recorded) = 0 points. Partly stated (Simply recorded as present, excluded known classification systems/specifics) = 1 point Fully stated (Negative findings stated or if pathology exists the record includes details of known classification systems/ specifics) = 2 points
Biopsy:
Partly stated (e.g. recorded as biopsy taken, no details of site and number of biopsies) = 1 point Fully stated ( i.e. all details of site and number of biopsies clearly stated) = 2 points
Diagnosis:
"Diagnosis" made is not recognised as per the MST list of diagnoses = 1 point. Recorded diagnosis is recognised as per the MST list of diagnosis = 2 points. Grade A: Scores > 36, Grade B 28-36, Grade C < 28.
A score of / was given if name and signature were present as well as partially stated biopsy information. A score of one (1) was given if date was stated, borderline legibility as well as non-MST-based diagnoses given. A score of two (2) was given if biopsy information was fully stated, diagnosis as per MST and a clearly legible report.
Acknowledgements
We would like to thank Arpana Mohanlal and Thiruvashnee Thaver for their assistance with data collection.
REFERENCES
1. Aabakken L, Rembacken B, LeMoine O, et al. Minimal standard terminology for gastrointestinal endoscopy-MST 3.0. Endoscopy. 2009;41(8):727-8. [ Links ]
2. Delvaux M, Korman L, Armengol-Miro J, et al. The minimal standard terminology for digestive endoscopy: introduction to structured reporting. Int J Med Inform. 1998;48(1):217-25. [ Links ]
3. Delvaux MM. Standardization of the endoscopic report. In: Waye JD, Rex DK, Williams CB. Colonoscopy: Principles and Practice. Massachusetts: Blackwell; 2003. p 183-98. [ Links ]
4. Korman LY, Delvaux M, Crespi M. The minimal standard terminology in digestive endoscopy: perspective on a standard endoscopic vocabulary. Gastrointest Endosc. 2001;53(3):392-6. [ Links ]
5. Delvaux M, Crespi M, Korman L, et al. Minimal standard terminology for digestive endoscopy. Terms and attributes, Version 2.0. Normed Verlag, Bad Homburg, Englewood NJ; 2002. [ Links ]
6. Delvaux M, Korman L. Digestive Endoscopy: Minimal Standard Terminology 2.0. Committee For Minimal Standard Terminology, OMED Ed. 1998:06-1998. [ Links ]
7. Korman L, Delvaux M, Bidgood D. Structured reporting in gastrointestinal endoscopy: Integration with DICOM and minimal standard terminology. Int J Med Inform. 1998;48(1):201-6. [ Links ]
8. Delvaux MM. Minimal Standard Terminology for Data Processing in Digestive Endoscopy: A Trend Towards Standardization of Endoscopic Reports. Dig Endosc. 1999;11(4):301-14. [ Links ]
9. Haux R. Medical informatics: past, present, future. Int J Med Inform. 2010;79(9):599-610. [ Links ]
10. Rugge M, Meggio A, Pennelli G, et al. Gastritis staging in clinical practice: The OLGA staging system. Gut. 2007;56(5):631-6. [ Links ]
11. Sipponen P, Price AB. The Sydney System for classification of gastritis 20 years ago. J Gastroenterol Hepatol. 2011;26(1) Suppl:31-4. [ Links ]
12. Forrest JF, ND.; Shearman, DJ. Endoscopy in gastrointestinal bleeding. Lancet. 1974;2(7877):394-7. [ Links ]
13. Hadzibulic E, Govedarica S. Significance of Forrest classification, Rockall's and Blatchford's risk scoring system in prediction of rebleeding in peptic ulcer disease. Acta Medica Medianae. 2007;46(4):38-43. [ Links ]
14. de Groot NL, van Oijen M, Kessels K, et al. Reassessment of the predictive value of the Forrest classification for peptic ulcer rebleeding and mortality: can classification be simplified? Endosc. 2014;46(1):46-52. [ Links ]
15. CMSA. Regulations for admission to the Fellowship of the College of Surgeons of South Africa FCS (SA) Johannesburg College of Medicine of South Africa; 2015 [cited 10 May 2015]. Available from: http://www.collegemedsa.ac.za/view_exam.aspx?examid=46 [ Links ]
 Correspondence:
Correspondence:
Prof TEMadiba
madiba@ukzn.ac.za


{kind=link}
{kind=link}
{kind=link}