










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.55 no.4 Cape Town Nov. 2017
TRAUMA
Quantifying the funding gap for management of traumatic brain injury at a major trauma centre in South Africa
V Y KongI; J J OdendaalI; J L BruceI; G L LaingI; E JeromeI; B SartoriusII; P BrysiewiczII; D L ClarkeI, III
IPietermaritzburg Metropolitan Trauma Service, Department of Surgery, University of KwaZulu-Natal, Durban, South Africa
IISchool of Nursing and Public Health, University of KwaZulu-Natal, Durban, South Africa
IIIDepartment of Surgery, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: Trauma is an eminently preventable disease. However, prevention programs divert resources away from other priorities. Costing trauma related diseases helps policy makers to make decisions on re-source allocation. We used data from a prospective digital trauma registry to cost Traumatic Brain Injury (TBI) at our institution over a two-year period and to estimate the funding gap that exists in the care of TBI.
METHODS: All patients who were admitted to the Pietermaritzburg Metropolitan Trauma Service (PMTS) with TBI were identified from the Hybrid Electronic Medical Registry (HMER). A micro-costing model was utilised to generate costs for TBI. Costs were generated for two scenarios in which all moderate and severe TBI were admitted to ICU. The actual cost was then sub-tracted from the scenario costs to establish the funding gap.
RESULTS: During the period January 2012 to December 2014, a total of 3 301 patients were treated for TBI in PMB. The mean age was 30 years (SD 50). There were 2 632 (80%) males and 564 (20%) females. The racial breakdown was overwhelmingly African (96%), followed by Asian (2%), Caucasian (1%) and mixed race (1%). There were 2 540 mild (GCS 13-15), 326 moderate (9-12), and 329 severe (GCS <8) TBI admissions during the period under review. A total of 139 patients died (4.2%). A total of 242 (7.3%) patients were admitted to ICU. Of these 137 (57%) had a GCS of 9 or less. A total of 2 383 CT scans were performed. The total cost of TBI over the two-year period was ZAR 62 million. If all 326 patients with moderate TBI had been admitted to ICU there would have been a further 281 ICU admissions. This was labelled Scenario 1. If all patients with severe as well as moderate TBI had been admitted there would have been a further 500 ICU admissions. This was labelled Scenario 2. Based on Scenario 1 and Scenario 2 the total cost would have been ZAR 73 272 250 and ZAR 82 032 250 respectively. The funding gaps for Scenario 1 and Scenario 2 were ZAR 11 240 000 and ZAR 20 000 000 respectively.
CONCLUSION: There is a significant burden of TBI managed by the PMTS. The cost of managing TBI each year is in the order of sixty million ZAR. A significant funding gap exists in our environment. This data does not include any data on the broader social costs of TBI. Investing in programs to reduce and prevent TBI is justified by the potential for significant savings.
Introduction
Trauma is an eminently preventable disease. However, prevention programs divert resources away from other priorities. Governments and administrators need to be convinced that the resources devoted to prevention will be recuperated.13 For this reason, costing common traumatic conditions is important. Once the financial implications of injury are made explicit to planners it becomes clear that the financial outlay associated with prevention programs can be recuperated by the savings associated with reduced rates of injury. Globally, traumatic brain injury (TBI) is a major cause of both morbidity and mortality.48 In Sub-Saharan Africa, the incidence of TBI is 150-170 per 100 000 compared with a global average of 106 per 100 000.48 Dedicated programs to reduce the incidence and severity of TBI are urgently required. However, the physical and financial resources to manage this massive burden of disease are inadequate. This is especially the case in terms of access to critical care facilities. The development of an electronic trauma registry at our institution has allowed us to capture data in real time on all patients and allows us to provide a detailed overview of the burden of TBI in our setting. It also allows us to provide an accurate assessment of the resources necessary to manage severe TBI at an international standard.9 The aim of this study was to estimate the current cost of TBI to the hospital services in a moderate sized South African city by costing of TBI at our institution over a two year period.10 The secondary objective was to estimate the funding gap which exists between current expenditure and ideal expenditure for the management of this condition.
Clinical Setting
The Pietermaritzburg Metropolitan Trauma Service (PMTS) provides tertiary trauma care for over three million people in the city of Pietermaritzburg. The PMTS admit over 3000 trauma patients each year. An electronic trauma registry - the Hybrid Electronic Medical Registry (HMER) is maintained by PMTS and captures data prospectively at our institution. Ethics approval to maintain the registry has been obtained from the Biomedical Research Ethics Committee (BCA221/13 BREC) of the University of KwaZulu-Natal and from the Research Unit of the Department of Health. The admitting doctor records patient details onto an electronic proforma. This is the clerking process for all new trauma admissions so the clinical data is entered in real time. As the data is entered, it is then directly incorporated into the registry. The completed proforma is then printed and becomes the patient's clinical records. At operation (where relevant) and at discharge or death a similar process is followed. This system combines the functions of a medical registry and a medical record system. It also combines an electronic system with a paper-based system and hence the name HMER.
Methods
All patients with a TBI were identified from the HMER during the period January 2012 to December 2014. Standard demographic data was analysed. Patients were classified according to severity of head injury and age. We defined a severe TBI as Glasgow Coma Scale (GCS) < 8, moderate as GCS 9-12 and mild as GCS 13-15, in line with accepted international standards. We divided the cohort according to age: 0-5 years, 6-10 years, 10-17 years and adults. Data were processed and analysed using Stata 13.0 (StataCorp. 2013).
Costing Model
A micro-costing model was utilised in this study. Costs of consumables (e.g. analgesia) were obtained from the hospital finance manager. Cost of analgesia was estimated based on a set protocol given over the mean duration of hospital stay. The cost of computerised tomographic (CT) brain scan and formal report from attending radiologist were obtained from the manager from the department of radiology in our trauma center. Similarly, the cost for a battery of standard laboratory tests (e.g. full blood count, electrolytes, blood gas, etc.) was obtained from the laboratory manager and was estimated as a sum total based on a routine batch of tests undertaken during resuscitation and duration of hospital stay. All other information pertaining to the cost of operating room (ZAR 100 per minute), intensive care (ICU) stay (ZAR 8 000 per day) and general ward stay (ZAR 2 000 per day) were obtained from the hospital financial manager. The sum of each individual cost drivers was used to generate an estimated total cost. The individual cost formulae were depicted in Model 1. The total cost was calculated by summation of all the individual costs. We did not estimate the cost of surgery as all neurosurgical operations were performed at the neurosurgical unit in Durban.

Estimating the funding gap
Once the actual cost was estimated an ideal cost was developed based on analysis of patient data. This was generated by performing an ideal costing based on the principle of gradation of the best of all possible worlds. The most restricted resource in our environment is intensive care unit (ICU) admission. Two more ideal scenarios were then considered and were labelled Scenario 1 and Scenario 2. Scenario 1 was generated by assuming that all patients with moderate TBI should have been admitted to intensive care unit (ICU) / high dependency unit (HDU). Scenario 2 was generated by assuming that all patients with severe and moderate TBI were admitted to ICU. The funding gap was generated by subtracting the actual costs from the estimated cost of Scenario 1 and Scenario 2.
Results
During the study period from January 2012 to December 2014, a total of 3 301 patients were treated for TBI at PMTS. The mean age was 30 years (SD 50). There were 2 632 males and 564 females, with a male to female ratio of 4.7:1. Their mean age was 27.4 years ± SD 14.4 (range 0-92 years). Mechanism of TBI (Figure 1) was primarily interpersonal violence (39.4%), followed by Motor Vehicle Collision (16.7%), and Pedestrian-Vehicle Collision (14.1%) The breakdown of the admission GCS is provided in Table 1. There were 2 540 mild (GCS 13-15), 326 moderate (9-12), and 329 severe (GCS < 8) TBI during the period under review. A total of 139 patients died (4.2%). A total of 242 (7.3%) patients were admitted to ICU. ICU admission by GCS category varied significantly (Table 1). The mean GCS (SD) among those who survived was 13.7 (2.6) compared to 5.7 (4.0) among those who died (p-value < 0.001). Thirty three percent (110/329) of patients with an admission GCS < 8 died whereas only 4 (13/326) and 0.6 (16/2540) per cent of those with an admission GCS between 9-12 and > 13 died respectively (p-value < 0.001). A total of 69 patients (2.5%) had an oxygen saturation reading of < 90 on presentation. A total of 2 383 CT scans were performed and 1 789 (75%) demonstrated intracranial pathology.
Cost of management and funding gap
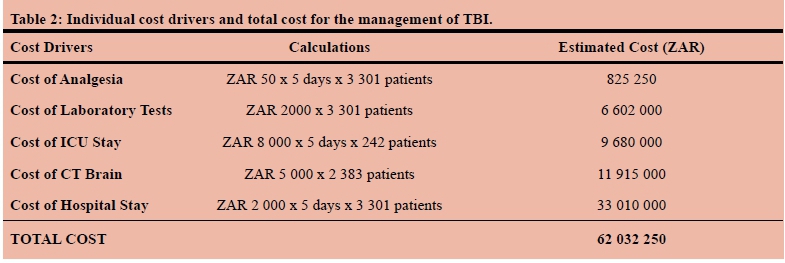
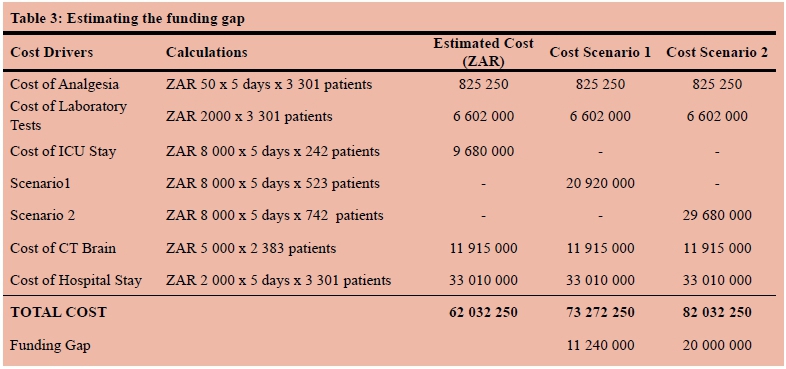
The individual cost drivers and total cost for managing the 3 301 patients over the three-year study period are summarised in Table 2. The total cost for managing all patients was ZAR 62 million. The greatest contribution to the overall cost was hospital stay followed by CT usage and then ICU admission. If all 326 patients with moderate TBI had been admitted to ICU, there would have been a further 281 ICU admissions. This was labelled Scenario 1. If all patients with severe as well as moderate TBI had been admitted there would have been a further 500 ICU admissions. This was labelled Scenario 2. Based on Scenario 1 and Scenario 2, the total cost would have been ZAR 73 272 250 and ZAR 82 032 250 respectively. The funding gaps for Scenario 1 and Scenario 2 were ZAR 11 240 000 and ZAR 20 000 000 respectively. Table 3 summarises these estimated funding gaps.
Discussion
Trauma in South Africa has been described as a malignant epidemic.1-3 This remains an apt description although it fails to emphasise the fact that trauma is also very much a neglected epidemic. The overall incidence of trauma in KZN Province for the years 2012-2014 was 17 per 1 000 population.3 This level of trauma demands a coordinated public health response, which mobilises across governmental sectors and involves broader society and a wide variety of stake-holders. Despite the paucity of data specific to TBI in the province, TBI must be regarded as a leading cause of death and disability in young adults both within the province and globally. In addition, recent evidence suggests that the incidence of TBI in low-middle income countries (LMIC) is increasing. If trauma is a neglected malignant epidemic, then TBI may very well be considered a neglected epidemic within an broader epidemic.1-3
In South Africa, tracking the burden of TBI is difficult as hospital record-keeping is suboptimal and very little funding is available for epidemiological monitoring and surveillance of trauma. In addition, interpersonal violence is a frequent cause of both trauma in general and TBI. The province-wide surveillance program in KZN suggests the ratio of intentional to non-intentional injury is 45:55.1-3 Improved patient outcomes will depend on an organised trauma system and a dedicated injury prevention program.
Estimating the cost of care is difficult in government facilities as financial metrics are poorly maintained. There are broadly two methods of calculating direct costs: the micro (bottom-up) and gross (top-down) approaches.10 Micro-costing involves recording and costing each component of a patient's care and summing them to obtain a total cost per patient. Gross-costing takes the overall institutional cost and divides it by the number of patients treated to generate an average cost per patient. Due to the level of detail involved in the micro-costing approach, this is regarded as the 'gold standard' for costing inpatient stays. However, it is labour intensive and impractical for use on a large scale.
Using a bottom-up approach, we have identified a major expenditure on TBI in our institutions. The cost of TBI in our environment is distorted by the fact that ICU resources are so restricted that a significant number of patients with moderate and serve TBI are denied access to ICU. Only 13% per cent of patients with a moderate TBI and 33% of patients with severe TBI were admitted to ICU. According to most international guidelines almost all of these patients with moderate or severe TBI should be admitted to the ICU for neuro-protective management. If we had complied with these guidelines, the cost of managing these patients would have increased dramatically as highlighted by our estimated funding gap.
There are a number of limitations associated with the costing model we have proposed. We have not costed the transportation to the neurosurgical service in Durban nor the cost of the operative interventions. Similarly, we have been unable to cost the care given to these patients once they have been repatriated from our institution back to their base district hospital. All this suggests that the true hospital cost of care will be even higher than what we have estimated in this project. In addition, this hospital-based costing provides a distorted view of the true financial burden of this injury. The long-term cost in terms of Disability-adjusted life year (DALY) and Quality-adjusted life years (QALY) is difficult to measure based on this methodology. Victims of TBI are frequently disabled and unable to return to work. TBI is not only associated with mortality but also with significant chronic morbidity in the form of long-term disability. The consequences of a TBI such as inability to care for oneself, epilepsy and loss of income are considerable. In addition, caring for a relative with TBI places a major strain on family and the broader community.
The issue of injury prevention is an important one and all these expenses associated with TBI can be avoided by preventing the injury in the first place.12-14 Most of the data on injury prevention suggests that educational interventions have a limited impact. Structural interventions such as pedestrian bridges and traffic calming have been shown to have an impact on behavior and to reduce the incidence of motor vehicle collisions. However, the most effective appears to be legislative interventions and improved enforcement. The issue of interpersonal violence is extremely contentious as the reasons for such high levels of such violence are poorly understood. Gun control is widely recommended as an intervention and has been implemented in South Africa. Reducing the rate of physical assault in our environment will require a multi-faceted approach which will include improved law enforcement, education and poverty eradication.
Conclusions
TBI result in significant hospital costs in KZN. If we managed patients according to international recommendations the cost of doing so would rise dramatically. In addition the long term consequences and costs of TBI are difficult to calculate and are likely to be even greater. Injury prevention programs will be a worthwhile investment, if they can reduce the burden of TBI.
REFERENCES
1. Laing GL, Skinner DL, Bruce JL, Aldous C, Oosthuizen GV, Clarke DL. Understanding the burden and outcome of trauma care drives a new trauma systems model. World J Surg. 2014 l;38(7):1699-706. doi: 10.1007/s00268-014-2448-8 [ Links ]
2. Muckart DJ. Trauma-the malignant epidemic. S Afr Med J. 1991;79:93-5. [ Links ]
3. Lutge E, Moodley N, Tefera A, Sartorius B, Hardcastle T, Clarke D. A hospital based surveillance system to assess the burden of trauma in KwaZulu-Natal Province South Africa. Injury. Jan 2016;47(1):135-40. doi: 10.1016/j.injury.2015.08.020. Epub 2015 Aug 21. [ Links ]
4. Wong JC, Linn KA, Shinohara RT, Mateen FJ. Traumatic brain injury in Africa in 2050: a modelling study. Eur J Neurol. 5 Oct 2015. doi: 10.1111/ene.12877 [ Links ]
5. Hyder AA, Wunderlich CA, Puvanachandra P, Gururaj G, Kobusingye OC. Neuro Rehabilitation. 2007;22(5):341-53. [ Links ]
6. Webster J, Taylor A, Balchin R. Traumatic brain injury, the hidden pandemic: A focused response to family and patient experiences and needs. S Afr Med J. Mar 2015;105(3):195-8. [ Links ]
7. Tran TM, Fuller AT, Kiryabwire J, Mukasa J, Muhumuza M, Ssenyojo H, Haglund MM. Distribution and characteristics of severe traumatic brain injury at Mulago National Referral Hospital in Uganda. World Neurosurg. Mar 2015;83(3):269-77. doi: 10.1016/j.wneu.2014.12.028. Epub 2014 Dec 19. [ Links ]
8. Zulu BM, Mulaudzi TV, Madiba TE, Muckart DJ: Outcome of head injuries in general surgical units with an off-site neurosurgical service. Injury. May 2007;38(5):576-83. [ Links ]
9. Okyere-Dede EK, Nkalakata MC, Nkomo T, Hadley GP, Madiba TE: Paediatric head injuries in the Kwazulu-Natal Province of South Africa: a developing country perspective. Trop Doct. Jan 2013;43(1):1-4. doi: 10.1177/0049475513480490 [ Links ]
10. Laing GL, Bruce JL, Skinner DL, Allorto NL, Clarke DL, Aldous C. Development, implementation and evaluation of a hybrid electronic medical record system specifically designed for a developing world surgical serviceWorld J Surg. 2014;38(6):1388-97. doi: 10.1007/s00268-013-2438-2 [ Links ]
11. Parkinson F, Kent SJ, Aldous C, Oosthuizen G, Clarke D. The hospital cost of road traffic accidents at a South African regional trauma centre: A micro-costing study. Injury. Jan 2014;45(1):342-5. doi: 10.1016/j.injury.2013.04.007. Epub 2013 Jun 2. [ Links ]
12. Staton C, Vissoci J, Gong E, Toomey N, Wafula R, Abdelgadir J, et al. Road Traffic Injury Prevention Initiatives: A Systematic Review and Metasummary of Effectiveness in Low and Middle Income Countries. PLoS One. 6 Jan 2016;11(1):e0144971. doi: 10.1371/journal.pone.0144971 [ Links ]
13. Nordberg E. Injuries as a public health problem in sub-Saharan Africa: epidemiology and prospects for control. East Afr Med J. Dec 2000;77(12 Suppl):S1-43. [ Links ]
14. Wesson HK, Boikhutso N, Hyder AA, Bertram M, Hofman KJ. Informing road traffic intervention choices in South Africa: the role of economic evaluations. Glob Health Action. 6 Jul 2016;9:30728. doi: 10.3402/gha.v9.30728. eCollection 2016. [ Links ]
 Correspondence:
Correspondence:
Victor Yeewai Kong
victorywkong@yahoo.com


{kind=link}
{kind=link}
{kind=link}