










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.55 no.4 Cape Town Nov. 2017
TRAUMA
Serum alcohol levels correlate with injury severity and resource utilization
A I Elshiere; M A Noorbhai; T E Madiba
Department of Surgery, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: Alcohol consumption leads to violence and poor judgement. The resultant trauma is the leading cause of emergency department visits. In South Africa, alcohol-related emergency visits can be as high as 57%. The purpose of this prospective study was to establish the prevalence of positive blood alcohol and Blood Alcohol Concentration (BAC) at a tertiary trauma unit in Durban, and to correlate it with injury severity, length of hospital stay and resource utilization.
METHODS: A total of 100 patients from King Edward trauma unit were analysed prospectively during the period December 2014 to February 2015. The BAC was correlated with Injury Severity Score (ISS), mechanism of injury, length of stay, and in-hospital mortality. Pearson chi-square test, Wilcoxon rank sum and student t-test were used for statistical analysis.
RESULTS: Eighty-eight patients were male. The mean age was 30 ± 9.3 years. Forty-seven patients tested positive for blood alcohol, of whom 81% were above the legal limit for professional drivers. The mean BAC among the alcohol positive patients was 0.146 g/dL. Positive blood alcohol was associated with significantly higher ISS scores (p = 0.0004). Injuries due to interpersonal violence were seen in 83 patients of whom 42 (51%) had positive blood alcohol. Hospital stay for alcohol positive patients was significantly longer compared to alcohol negative patients (p < 0.001).
CONCLUSION: The prevalence of blood alcohol in the trauma population is high. Positive blood alcohol is associated with high ISS and longer hospital stays.
Introduction
Excessive alcohol consumption is associated with physical and mental health problems, traffic accidents, falls, fires, and violence,1 owing to poor judgment. The resultant trauma accounts for 20% of emergency department visits.2,3 In South Africa, alcohol-related emergency department visits can be as high as 57%.4 Furthermore, alcohol-related injuries are more serious compared to other diseases and are responsible for economic loss due to lost productivity.1
The purpose of this prospective study was to assess the prevalence of positive blood alcohol levels at a tertiary trauma unit in Durban, and to correlate it with injury severity, length of hospital stay and resource utilization. South Africa is currently considering the reduction in the legal blood alcohol limit to less than 0.05 mg per 100 ml. This study will illustrate the burden of alcohol-related injuries at a tertiary hospital and will provide evidence to support the vision of reducing the blood alcohol limit.
Methods
Study setting
This prospective study was conducted at King Edward VIII Hospital in Durban, South Africa, to establish blood alcohol levels in all trauma patients during the 3-month period (December 2014-February 2015).
Study design
Patients were randomly selected based on the 'on-call' status of the principal investigator (AIE). The serum alcohol levels were collected by venepuncture on admission. No alcohol swabs were used to disinfect the skin prior to venepuncture. A Grey top BD Vacutainer® (Becton, Dickinson and Company, USA) (Ref 368921) with 10 mg sodium fluoride and 8 mg potassium oxalate as preservatives was used to collect each 5 ml sample. These tubes are routinely available within the trauma unit and have a reported stability of 2 days at 15-25°C.
Blood samples were collected for Serum Blood Alcohol Concentrations (BAC) in all 100 patients. The samples were taken by the study investigators and in some cases by the casualty officer. Once sampled, the tubes were tightly closed with no tube uncapping and the samples were then transported to Ampath Laboratory within 6 hours of blood sampling by the principal investigator. The laboratory is 5 kilometres from King Edward VIII Hospital and the distance can be covered in 10-15 minutes depending on traffic conditions. Samples were then analysed using the Roche/Hitachi cobas c501 analyser® (Roche, USA). The results were made available telephonically and via a password protected mobile application program within 6 hours. The alcohol levels were reported in grams per decilitre (g/dL). They were either reported as negative (0 g/dL) or specific values (>0 g/dL).
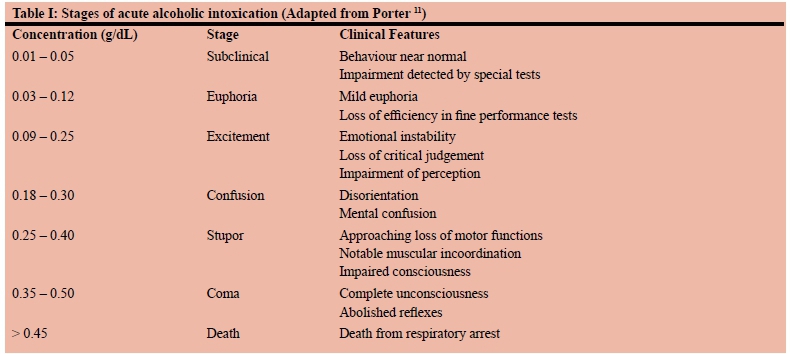
The serum alcohol levels, patient demographics and mechanism of injury were recorded. Vital signs (including GCS), serology, number of days in hospital, use of radiological investigations (x-rays, ultrasound, CT scan, etc.) and type of surgical intervention were documented. Data were then transferred from the data capture proforma onto a Microsoft Access database (Microsoft Office®, Redmond, Washington, USA). Results were compared to reference guide for various categories of blood alcohol levels. The stages of alcohol intoxication are shown in Table I. The current legal alcohol limits in South Africa are listed in the National Road Traffic Act No. 93 of 1996 (Section 65) for both nonprofessional and professional drivers.5 According to this Act, the legal alcohol limit for professional and non-professional drivers is < 0.020 g/dL and < 0.050 g/dL respectively. For the purposes of this study the BAC were categorized into Groups A (< 0.100 g/dL), B (0.100-0.200 g/dL) and C (> 0.200 g/dL). Group A was in keeping with levels within the legal limit in South Africa. Group B was in keeping with levels at which there is usually some loss of skill and slurred speech; and Group C was in keeping with levels at which disturbances of equilibrium, vision and perception may occur.
Statistical analysis
The BAC was then correlated with Injury Severity Score (ISS),6 mechanism of injury, length of stay, and in-hospital mortality. Pearson chi-square (or Fishers exact test where expected cell count was less than 5 observations) for categorical variables vs. alcohol status, T-test for comparison of continuous variable vs. alcohol status or Wilcoxon rank-sum for comparing continuous means vs. alcohol status. The data were analysed using the R statistics program. A p-value of < 0.05 was considered statistically significant.
Ethical considerations
This prospective study was approved by the Biomedical Research Ethics Committee (BE254/14) of the University of KwaZulu-Natal, Durban, South Africa. Further approval was obtained from the KwaZulu-Natal Department of Health via the Health Research and Knowledge Management Committee. Thereafter, the research committee at King Edward VIII hospital granted the remaining approval.
Results
One hundred randomly selected patients were included in the study of which 88 were male (male to female ratio 7:1). The average age was 30 years (median = 27; IQR 24-33, SD = 9.3 and range 18-63 years).
Forty-seven out of 100 patients tested positive for blood alcohol, including 41 out of 88 males (46.7%) and six out of 12 females (50.0%) (p = 0.824). The mean BAC among the alcohol positive patients was 0.146 g/dL. Fifteen patients fell into Group A (32%), 19 into Group B (40%), and 13 fell into Group C (28%) (Table II). The highest recorded BAC was 0.312 g/dL and 0.222 g/dL for males and females respectively. Only three patients fell within the South African legal limit for professional drivers (6.4%); six fell within the legal limit for non-professional drivers (12.8%) and the rest (80.9%) fell above the acceptable legal limit for all drivers in South Africa. Thirty-two out of 47 patients (68%) fell into the group in which they were at risk for disturbances of equilibrium, vision and perception.
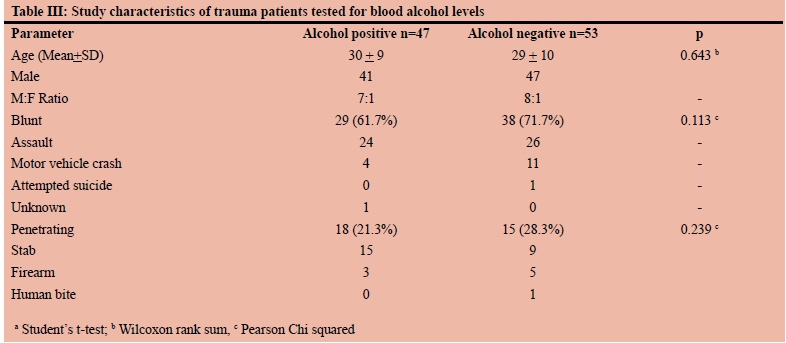
The study characteristics of alcohol negative and positive patients are shown in Table III. Blunt injury occurred in 67 patients (assaults 48, motor vehicle crashes 11, and other injuries 8). There was no positive relationship between BAC and mechanism of injury (p = 0.289). Thirty-three patients sustained penetrating trauma (stabs 24, firearms 8 and human bites 1). There was no positive correlation between BAC and any specific penetrating injuries (p = 0.239).
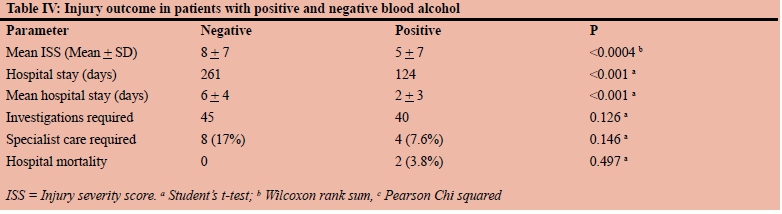
Table IV compares outcomes in alcohol positive and negative patients. The median ISS for the entire sample was 4 (IQR 0-7); it was statistically significantly higher amongst patients with positive blood alcohol (p = 0.0004). There was a significant difference in the length of stay (days) between alcohol positive (mean 5.5 ± 4.2, median 6.0, iQr 2.5-8.0) and alcohol negative patients (mean 2.3 ± 2.7, median 2.0, IQR 0-4.0) (p < 0.001) with alcohol positive patients staying twice as long as alcohol negative patients. The mean length of stay for patients in Groups A, B and C was 10, 10 and 12 days respectively. Thirty-one patients were discharged on the same day, 9 of whom had positive alcohol levels. The average alcohol level among this group was 0.160 g/dL which is higher than the mean of all alcohol positive patients (0.146 g/dL).
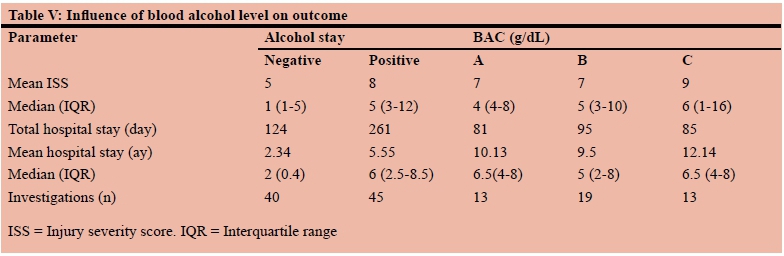
Table V shows the influence of alcohol on outcome. Basic radiological investigations (x-rays, full body Lodox x-rays, CT scans) were required in 92 patients, of whom 49 (53.3%) had positive blood alcohol. Thus 45 of 47 patients with blood alcohol required additional hospital resources compared to 40 of 53 blood alcohol negative patients (p = 0.146). Twelve patients required specialist referrals, of whom 8 (66.7 %) were alcohol positive, suggesting that alcohol positive patients required specialist consultations twice as often as alcohol negative patients (p = 0.146). Twelve patients required emergency surgery. Eight of these (66.7%) were alcohol positive and their injuries were due to interpersonal violence. The emergency surgical procedures included orthopaedic procedures (n = 2, 16.7%), craniotomy (n = 3, 25%), thoracotomy (n = 1, 8.3%), and laparotomy (n = 6, 50%). Only two patients died, both from the alcohol negative group.
Discussion
The net effect of alcohol consumption on health globally is detrimental with an estimated 3.8 - 7.1%% of all deaths and 4.6 - 7% of disability-adjusted life-years (DALYs) globally attributable to alcohol.7,8The amount of absolute alcohol consumption in South Africa was estimated at 10,3 litres per adult a year in 2000,7 and the estimated burden of disease attributable to alcohol use then was 7.1% of all deaths and 7.0% of total DALYs.9 The amount in 2015, was closer to 20 litres per adult and among the highest in the world.10
The test was outsourced to a private laboratory that offers this test routinely with a relatively quick turnaround time. In this study, the BAC was used as opposed to breath analysers, as the latter provide an indirect estimation of BAC and are thus associated with false positive results as seen in acetone breath in patients with diabetes mellitus.11 Controversy also abounds with respect to breath analysers with some authors suggesting their unreliability and proneness to false positive results due to their tendency to identify substances containing a similar molecular structure to ethanol 12 while others attest to their reliability.13
This study has shown that a positive blood alcohol level is associated with increased injury severity and increased length of hospital stay. However, subgroup analysis demonstrates that, whereas blood alcohol positivity was associated with longer length of stays, it may not be dependent on the actual blood alcohol concentration. Although patients with positive blood alcohol tended to require the use of more hospital resources, this was not statistically significant. Numbers were small in this study and it is possible that these figures may change and statistical significance may or may not be reached. Nevertheless, the bottom line is that trauma in alcohol-positive patients is associated with grave outcome.
The power imbalance between industry and health groups is a key reason for the continuing neglect of alcohol as a global health issue.14 The reasons given for this neglect include the absence of clarity on the alcohol control message, the political context that gives priority to an individual's responsibility for health, and the close connection of alcohol with many aspects of social and cultural norms.10
In South Africa, alcohol abuse costs the country at least R9 billion a year.4 Pedestrian trauma alone costs $83 million per year whilst motor vehicle collisions costs the country $1.5 billion per year, of which 50% are alcohol related.4 In the United States, medical insurance companies can deny coverage for injuries caused by alcohol use, shifting these expenses to trauma centres.15 Furthermore, 30% of general hospital admissions in South Africa have positive blood alcohol and the trauma units have prevalence rates of between 22 and 57%.16 The 47% reported in this study falls within this range. International figures range between 6% for the United States and 46% for Germany.1,15-18
The study by Parry showed that 73% of violence related injuries were linked to alcohol in parts of the country and that 46% of motor vehicle-related injuries were alcohol induced.16 The present study has demonstrated a significantly higher ISS for alcohol positive patients compared to their negative counterparts, an observation made by others.19
The present study is supported by Swearingen et al. who demonstrated an association between positive BAC and a significantly increased resource utilization, length of stay, total ICU days and worsened outcomes.19 Furthermore, O'Keeffe et al. in 2013 demonstrated that blood alcohol positive patients were twice as likely to be admitted compared to alcohol negative patients, and tended to require more monitoring, diagnostic tests and procedures, as well as longer emergency department length of stay.15 These findings mimic the present study in which alcohol positive patients were more likely to be admitted to the ICU, and had a longer hospital stay. A larger number of alcohol positive patients tended to require specialist referral and emergency surgery although this was not statistically significant.
The risk of traffic accidents, fires, and mortality are significantly higher in intoxicated individuals.1 The fact that the prevalence rates of BAC positive patients in trauma units have remained constant, despite legislative efforts, requires more drastic measures in order to curb alcohol use and the resultant transport and violence-related injuries.
Interventions by the South African government to reduce alcohol intake have somewhat succeeded in reducing the risk of alcohol-related trauma.20 Given the prevalence of alcohol positivity in trauma centres coupled with the resultant grave outcomes noted above, we believe that screening, alcohol-reducing intervention, and counselling for alcohol problems should be routine.20,21 These steps have been shown to offer a cost benefit to the health sector in the world literature.21
We are in agreement with Parry et al. that alcohol misuse has huge implications for public health policy, such as the need to develop protocols for the management of alcohol-positive patients in trauma units and to target prevention programs at heavy drinking by young people.16
The South African Government has adopted strategies to curb the use of alcohol by employing methods such as (i) labelling messages to consumers which occupy at least 12.5% of the container label, (ii) prohibition of any health benefit claims, and (iii) warnings that excessive alcohol consumption could result in brain damage and death.10 Steps to prevent undue exposure to drugs and alcohol by the International Commission for the Prevention of Alcoholism and Drug Dependency in South Africa (ICPA in SA) are welcome.10 The National Liquor Act of 2003 encourages responsible drinking to reduce the social and economic costs of alcohol abuse and restricts advertising on alcohol consumption.22 In addition, the South African Department of Health has published the MiniDrug MasterPlan 23 which stipulates that "Individuals who present at trauma units with alcohol or drug-related injuries, should be screened and where indicated receive brief interventions and/or appropriate referrals to treatment". We are in agreement with others that focus should now shift to making resources available for implementing intervention strategies8 and that screening by blood alcohol concentration (BAC) measurement and counselling may decrease the incidence and consequences of trauma.1
The study does have limitations. The sample size was small with only 100 patients. The funding of the outsourcing of the test to a private laboratory was by the investigators and impacted on the sample size. A further study of resource usage and costs performed in larger numbers on major trauma patients will strengthen the findings of this study.
In conclusion, the prevalence of positive alcohol blood levels at this tertiary trauma unit was 47%. Positive blood alcohol is associated with high ISS and longer hospital stays. Interventions are desperately required at various levels to curb this problem. Blood alcohol levels should be routinely collected at all trauma units. The Department of Health can play an important facilitator role to have alcohol level tested at all trauma units in KwaZulu-Natal and subsequently countrywide. No patients should be discharged until the blood alcohol level is known. There is a need for community-based education with regards to alcohol contribution to trauma. We further make a recommendation to the policy makers for the reduction of the legal alcohol limit to zero in order to further curb alcohol usage and enforce sobriety during all interactions including driving, road use and personal communication.
Acknowledgements
We would like to thank Dr Knobleugh (Ampath Laboratories) and associated staff for their assistance with calculating the blood alcohol levels and Prof B Sartorius for his statistical input.
Competing interests
The authors declare that they have no competing interests.
REFERENCES
1. Yoonhee C, Kooyoung J, Eunkyung E, et al. The relationship between alcohol consumption and injury in ED trauma patients. Am J Emerg Med. 2009;27(8):956-60. [ Links ]
2. Cherpitel CJ. Alcohol and injuries: a review of international emergency room studies. Addiction. 1993;88(7):923-37. [ Links ]
3. Gentilello LM, Duggan P, Drummond D, et al. Major injury as a unique opportunity to initiate treatment in the alcoholic. Am J Surg. 1988;156(6):558-61. [ Links ]
4. Parry C. Alcohol use in South Africa. Tygerberg, South Africa: Medical Research Council, 1999. [ Links ]
5. Government SA. National Road Traffic Act 93 of 1996 as Amended (National Road Traffic Amendment Bill, 2015). In: Transport Do, ed. Pretoria: SA Government; 2015. p. 1-64. [ Links ]
6. Baker SP, O'Neill B, Haddon Jr W, Long WB. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma Acute Care Surg. 1974;14(3):187-96. [ Links ]
7. Rehm J, Mathers C, Popova S, Thavorncharoensap M, Teerawattananon Y, Patra J. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet. 2009;373(9682):2223-33. [ Links ]
8. Schneider M, Norman R, Parry C, Bradshaw D, Pluddemann A, Collaboration SACRA. Estimating the burden of disease attributable to alcohol use in South Africa in 2000. S Afr Med J. 2007;97(8):664-72. [ Links ]
9. Peltzer K, Davids A, Njuho P. Alcohol use and problem drinking in South Africa: findings from a national population-based survey. Afr J Psych. 2011;14(1). [ Links ]
10. Strachan K. A profile of alcohol in South Africa. In: Clarke E, ed. Health Systems Trust Update. Durban, South Africa: Department of Health; 1999:5-12. [ Links ]
11. Porter W. Clinical Toxicology. In: Burtis C, Ashwod E, Bruns D, SAwyer B, eds. Tietz Fundamentals of Clinical Chemistry. 6 ed. Louisville, Missouri: Saunders; 2008:562-602. [ Links ]
12. Spector NH. Alcohol breath tests: Gross errors in current methods of measuring alveolar gas concentrations. Science. 1971;172(3978):57-9. [ Links ]
13. Bates ME, Brick J, White HR. The correspondence between saliva and breath estimates of blood alcohol concentration: advantages and limitations of the saliva method. J Studies Alcohol. 1993;54(1):17-22. [ Links ]
14. Shiffman J, Smith S. Generation of political priority for global health initiatives: a framework and case study of maternal mortality. Lancet. 2007;370(9595):1370-9. [ Links ]
15. O'Keeffe T, Rhee P, Shafi S, Friese RS, Gentilello LM. Alcohol use increases diagnostic testing, procedures, charges, and the risk of hospital admission: a population-based study of injured patients in the emergency department. Am J Surg. 2013;206(1):16-22. [ Links ]
16. Parry CD, Bhana A, Myers B, et al. Alcohol use in South Africa: Findings from the South African community epidemiology network on drug use (SACENDU) project. J Studies Alcohol. 2002;63(4):430-5. [ Links ]
17. Gazal-Carvalho C, Carlini-Cotrim B, Silva OA, Sauaia N. Blood alcohol content prevalence among trauma patients seen at a level 1 trauma center. Revista de Saude Publica. 2002;36(1):47-54. [ Links ]
18. Stübig T, Petri M, Zeckey C, et al. Alcohol intoxication in road traffic accidents leads to higher impact speed difference, higher ISS and MAIS, and higher preclinical mortality. Alcohol. 2012;46(7):681-6. [ Links ]
19. Swearingen A, Ghaemmaghami V, Loftus T, et al. Extreme blood alcohol level is associated with increased resource use in trauma patients. Am Surg. 2010;76(1):20-4. [ Links ]
20. Gentilello LM, Rivara FP, Donovan DM, et al. Alcohol interventions in a trauma center as a means of reducing the risk of injury recurrence. Ann Surg. 1999;230(4):473. [ Links ]
21. Gentilello LM, Ebel BE, Wickizer TM, Salkever DS, Rivara FP. Alcohol interventions for trauma patients treated in emergency departments and hospitals: a cost benefit analysis. Ann Surg. 2005;241(4):541-50. [ Links ]
22. South African Government. National Liquor Act 59 of 2003. Department of Trade and Industry, Pretoria, South Africa 2003. [ Links ]
23. South African Government. MiniDrug MasterPlan. Department of Health, Pretoria 2014. [ Links ]
 Correspondence:
Correspondence:
Prof TE Madiba
madiba@ukzn.ac.za


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}