










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.55 n.4 Cape Town Nov. 2017
TRAUMA
Rib fracture fixation in a South African public trauma service
G V OosthuizenI; J De WetII; J L BruceI; D L ClarkeI
IPietermaritzburg Metropolitan Trauma Service, University of KwaZulu Natal, Pietermaritzburg, South Africa
IIDepartment of Orthopaedics, Edendale Hospital, University of KwaZulu Natal, Pietermaritzburg, South Africa
ABSTRACT
BACKGROUND: Rib fractures and flail chests have traditionally been treated nonoperatively. Current literature suggests that it is not only safe and feasible but also desirable to perform fixation of severe rib fractures. Our unit in the Pietermaritzburg public sector adopted rib fracture fixation in 2014 and in this audit we assess its feasibility in our setting.
METHODS AND RESULTS: We audited our first nine cases of rib fracture fixation performed to date, of which seven were males. The age range was 29 to 67 years. All patients had multiple rib fractures with severe displacement; one had bilateral flail segments and one had severely displaced unilateral single fractures without flail; all others had unilateral flail chests. Time from injury to operation ranged from 3 to 20 days. Of six ventilator dependent patients, all but one were liberated from the ventilator within 3 days after fixation (1-3 days). The remaining patient remained ventilator dependent for 10 days while recovering from traumatic brain injury. This patient aside, all were discharged from ICU within 5 days. Patients with no other significant injuries were discharged from hospital within five to eight days; all being mobile within five days. Procedure-related complications included accidental pleural breach during rib mobilization necessitating intercostal drain placement (2 patients) and superficial wound infection (1 patient). All patients were discharged well.
CONCLUSION: Rib fracture fixation is safe and feasible in our unit and is feasible in the South African public sector.
Introduction
Nonoperative management strategies have been suggested for the management of flail chest since the 1950s and most trauma surgeons still follow this approach today.1-4 However, follow-up studies on patients with rib fractures which have been managed nonoperatively have demostrated a significant incidence of chronic pain and disability.5 This results in a significantly decreased quality of life with only 71% of victims ever returning to any form of work.6 Dating back to the 1960s, various authors have attempted operative management of flail chest using a variety of techniques such as curved struts, intramedullary nails, wires, Kirschner wires, staples, and bone grafts.7-8 More recent literature has confirmed the safety and efficacy of modern rib fracture fixation techniques.9-12 In our unit (Pietermaritzburg Metropolitan Trauma Service), we admit approximately 2 500 trauma patients annually, among whom only approximately 10 present with flail chests or severely displaced rib fractures and associated mechanical breathing difficulties. In response to the growing body of evidence showing safety and benefit of modern rib fracture fixation, we adopted the technique in 2014. This retrospective audit reviews our experience with the technique over the last three years and goes on to demonstrate the feasibility of rib fracture fixation in the South African public sector.
Methods
A retrospective audit was performed of all cases of rib fracture fixation performed between April 2014 and March 2017.
Technique
We adopted rib fracture fixation in 2014. The first author was formally trained to perform the procedure by an experienced team based in Sweden. Further practice was guided by literature.13 Our initial indication for rib fracture fixation was major rib cage deformity with anticipated difficulty in mechanical breathing.
Currently our indications are in line with those suggested by Pieracci et al from Denver14 and essentially encompass three categories: acute respiratory insufficiency despite optimal medical therapy, uncontrolled pain despite optimal medical therapy, and anticipated chronic pain or impaired pulmonary mechanics. The same Denver group performed a randomised controlled trial (RCT) in 201512 in which they showed that patients with the mentioned indications undergoing rib fracture fixation within 3 days had significant decreases in respiratory failure, duration of mechanical ventilation, and need for tracheostomy, as well as significantly better daily incentive spirometry readings.
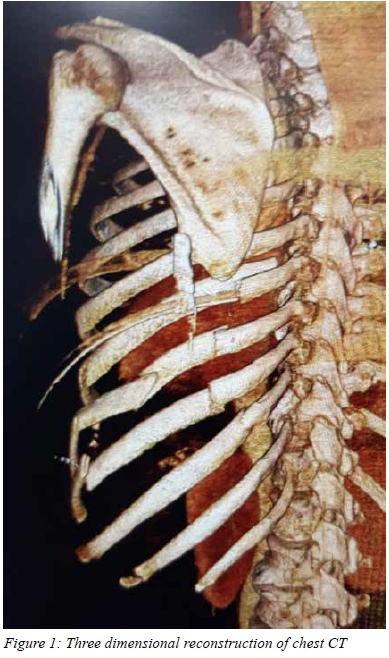
In our unit, all patients with multiple rib fractures and/or flail chest undergo CT of the chest with 3D reconstruction,15 followed by multidisciplinary discussion between trauma surgery, orthopaedics and intensive care. When all are in agreement for the need of the procedure and the patient is agreeable, cash flow approval is secured, the relevant company representative is contacted to provide the plating set, and the 3D reconstructed CT is used for planning the incisions (Figure 1).
Most patients tend to have a combination of anterior and posterior fractures, so that the lateral position is sufficient for most, with a curvilinear incision similar to that used for posterolateral thoracotomy. Skin and subcutaneous tissue flaps are raised and a minimally invasive/muscle-splitting technique is employed to access the rib fractures (Figure 2). For securing plates deep to the scapula, we employ either a trans-scapular or a subscapular technique. We have used two different sets (Matrix Rib Fixation System, DePuy Synthes, and Ribfix Blu, Zimmer Biomet) - there is little to choose between the sets in terms of ease of use and results. We use prophylactic cefazolin and leave a suction drain in the vicinity of the plates for two to three days postoperatively. Patients tend to be mobile from day one, if they are not ventilated. Potential complications include wound infection, osteomyelitis, plate migration, and nerve injury.16 While we believe that this procedure should form part of every trauma surgeon's armamentarium, it is probably advisable to seek the assistance of an experienced orthopaedic surgeon for every procedure.

Results
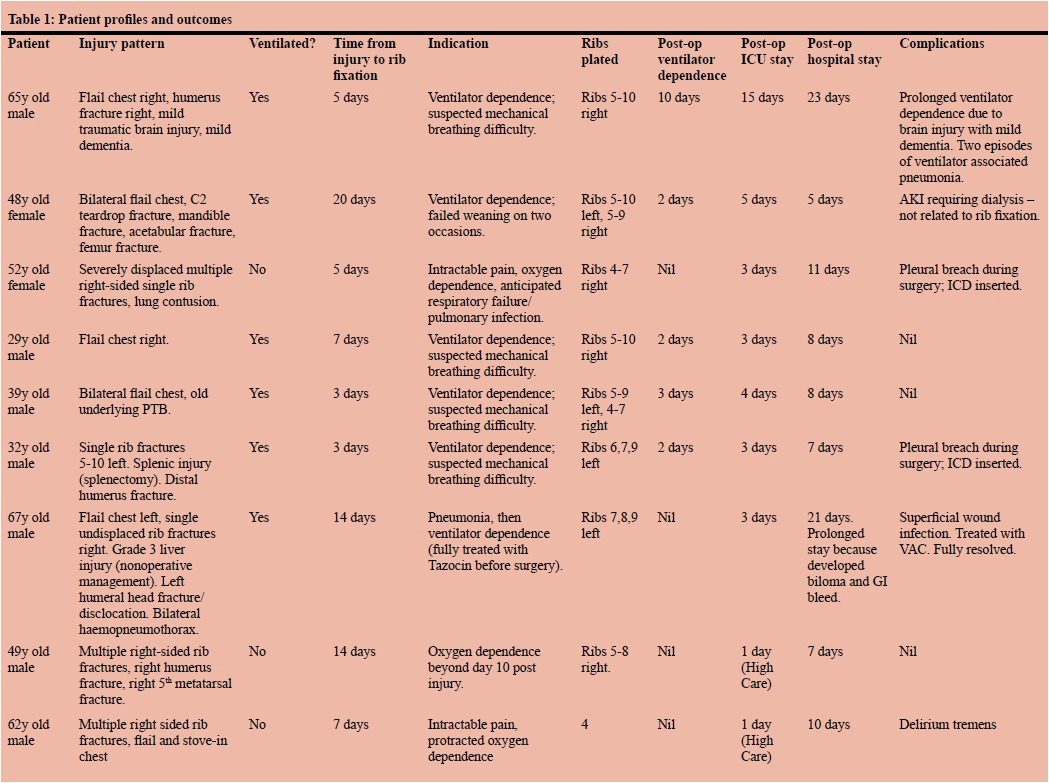
Nine patients underwent surgical rib fracture fixation, of which seven were male. Patient profiles and outcomes are tabulated in Table 1. The age range was 29 to 67 years. All patients had multiple rib fractures with severe displacement; one had bilateral flail segments and one had severely displaced unilateral single fractures without flail; all others had unilateral flail chests. Six patients were ventilator dependent. Time from injury to operation ranged from 3 to 20 days. We used the following rib fixation sets: Matrix Rib Fixation System, DePuy Synthes (3 patients), and Ribfix Blu, Zimmer Biomet (6 patients). All displaced rib fractures were plated; on flail segments both anterior and posterior fractures were plated, most commonly with one long plate, less commonly with two separate plates. Initially muscle cutting, but later muscle sparing techniques were employed.
Of the six ventilator dependent patients, all but one were extubated within 3 days. The remaining patient remained ventilator dependent for 10 days whilst recovering from a traumatic brain injury. This patient remained in ICU for 15 days, while the others were all discharged from ICU within 5 days. Postoperative length of stay ranged from 7 to 23 days. Five patients with no other significant injuries were discharged within five to eight days, all having been mobile within five days. Procedure-related complications included accidental pleural breach during rib mobilsation necessitating intercostal drain placement (2 patients) and superficial wound infection (1 patient; successfully treated with VAC dressing). All patients were discharged well.
Discussion
Just under a decade ago in 2009 a survey undertaken among trauma surgeons, orthopaedic surgeons, and thoracic surgeons17 found that most of these professionals believed that nonoperative management was sufficient for flail chest. Since then that attitude seems to have changed towards a more operative approach and this has been supported by a number of RCTs. An RCT from 20029 found that patients with flail chests, intubated and ventilated in the emergency department and undergoing rib fracture fixation within 14 days had a significantly decreased duration of mechanical ventilation, incidence of pneumonia, need for tracheotomy, length of ICU stay, and total medical expense. In addition, a year after repair, respiratory functions were superior in the group that underwent fixation, and symptoms such as chest tightness, chest cage pain, and dyspnoea on effort were significantly decreased as compared to the nonoperatively managed group. Furthermore, return to normal employment was significantly higher in the operative group. A further RCT from 200510 found that patients with flail chest undergoing operative repair within 24-36 hours had significantly decreased duration of mechanical ventilation, incidence of pneumonia, length of ICU stay, length of hospital stay, and chest wall deformity. In addition, respiratory functions were superior to nonoperatively managed patients at 2 months follow-up. A third RCT published in 201311 showed that patients with a flail chest and who were being ventilated with no prospect of weaning within 48 hours, who underwent rib fracture fixation, had significant decreases in duration of mechanical ventilation, incidence of pneumonia, need for tracheostomy, length of ICU stay, and hospital costs. Several systematic reviews and meta-analyses have confirmed superior outcomes for operatively treated patients.18-23
Our experience with this procedure is in agreement with the findings of the abovementioned RCTs. Rib fracture fixation is technically easy to perform and results in dramatic improvement of respiratory function. This is evidenced by the expeditious weaning and extubation of almost all the patients in this series. Our overall impressions are that early operation is ideal, patient selection is critical, and that patients should be fit for discharge within one week of operation, unless there are other reasons for ongoing hospitalisation.
Limitations
It costs in the order of 10 000 ZAR to plate each rib (cost of plates and screws), and generally each patient requires between 4 to 10 rib fixations. This is a major limitation especially in a resource constrained environment. The cost of the procedure needs to be weighed against the cost saved in terms of ICU occupancy and hospital stay, and detailed cost analyses must be undertaken.
Conflict of interest
We have no conflicts of interest.
Ethics approval
This was an audit conducted from data captured in our Hybrid Electronic Medical Registry (HEMR). Ethics approval for this study and for maintenance of the registry was obtained from the Biomedical Research Ethics Committee (BREC) of the University of KwaZulu-Natal (reference: BE 207/09).
REFERENCES
1. Pettiford BL, Luketich JD, Landreneau RJ. The management of flail chest. Thorac Surg Clin. 2007;17(1):25-33. [ Links ]
2. Vana PG, Neubauer DC, Luchette FA. Contemporary management of flail chest. Am Surg. 2014;80(6):527-35. [ Links ]
3. Nishiumi N, Fujimori S, Katoh N, Iwasaki M, Inokuchi S, Inoue H. Treatment with internal pneumatic stabilization for anterior flail chest. Tokai J Exp Clin Med. 2007;32(4):126-30. [ Links ]
4. Gunduz M, Unlugenc H, Ozalevli M, Inanoglu K, Akman H. A comparative study of continuous positive airway pressure (CPAP) and intermittent positive pressure ventilation (IPPV) in patients with flail chest. Emerg Med J. 2005;22(5):325-9. [ Links ]
5. Gordy S, Fabricant L, Ham B, Mullins R, Mayberry J. The contribution of rib fractures to chronic pain and disability. Am J Surg. 2014;207(5):659-62. doi: 10.1016/j.amjsurg.2013.12.012 [ Links ]
6. Marasco S, Lee G, Summerhayes R, Fitzgerald M, Bailey M. Quality of life after major trauma with multiple rib fractures. Injury. 2015;46(1):61-5. doi: 10.1016/j.injury.2014.06.014 [ Links ]
7. Paris F, Tarazona V, Blasco E, Cantó A, Casillas M, Pastor J, et al. Surgical stabilization of traumatic flail chest. Thorax. 1975;30(5):521-7. [ Links ]
8. Beltrami V, Martinelli G, Giansante P, Gentile K. An original technique for surgical stabilisation of traumatic flail chest. Thorax, 1978, 33, 528-9. [ Links ]
9. Tanaka H, Yukioka T, Yamaguti Y, Shimizu S, Goto H, Matsuda H, et al. Surgical stabilization of internal pneumatic stabilization? A prospective randomized study of management of severe flail chest patients. J Trauma. 2002;52(4):727-32. [ Links ]
10. Granetzny A, Abd El-Aal M, Emam E, Shalaby A, Boseila A. Surgical versus conservative treatment of flail chest. Evaluation of the pulmonary status. Interact Cardiovasc Thorac Surg. 2005;4(6):583-7. [ Links ]
11. Marasco SF, Davies AR, Cooper J, Varma D, Bennett V, Nevill R, et al. Prospective randomized controlled trial of operative rib fixation in traumatic flail chest. J Am Coll Surg. 2013;216(5):924-32. doi: 10.1016/j.jamcollsurg.2012.12.024 [ Links ]
12. Pieracci FM, Lin Y, Rodil M, Synder M, Herbert B, Tran DK, et al. A prospective, controlled clinical evaluation of surgical stabilization of severe rib fractures. J Trauma Acute Care Surg. 2016;80(2):187-94. doi: 10.1097/TA.0000000000000925 [ Links ]
13. Marasco S, Saxena P. Surgical rib fixation - technical aspects. Injury. 2015;46(5):929-32. doi: 10.1016/j.injury.2014.12.021 [ Links ]
14. Pieracci FM, Rodil M, Stovall RT, Johnson JL, Biffl WL, Mauffrey C, et al. Surgical stabilization of severe rib fractures. J Trauma Acute Care Surg. 2015;78(4):883-7. doi: 10.1097/TA.0000000000000581 [ Links ]
15. Pulley BR, Taylor BC, Fowler TT, Dominguez N, Trinh TQ. Utility of three-dimensional computed tomography for the surgical management of rib fractures. J Trauma Acute Care Surg. 2015;78(3):530-4. doi: 10.1097/TA.0000000000000563 [ Links ]
16. Sarani B, Schulte L, Diaz JJ. Pitfalls associated with open reduction and internal fixation of fractured ribs. Injury. 2015;46(12):2335-40. doi: 10.1016/j.injury.2015.10.022 [ Links ]
17. Mayberry JC, Ham LB, Schipper PH, Ellis TJ, Mullins RJ. Surveyed opinion of American trauma, orthopedic, and thoracic surgeons on rib and sternal fracture repair. J Trauma. 2009;66(3):875-9. doi: 10.1097/TA.0b013e318190c3d3 [ Links ]
18. Swart E, Laratta J, Slobogean G, Mehta S. Operative Treatment of Rib Fractures in Flail Chest Injuries: A Meta-analysis and Cost-Effectiveness Analysis. J Orthop Trauma. 2017;31(2):64-70. doi: 10.1097/BOT.0000000000000750 [ Links ]
19. Schuurmans J, Goslings JC, Schepers T. Operative management versus non-operative management of rib fractures in flail chest injuries: a systematic review. Eur J Trauma Emerg Surg. 2016 Aug 29. [Epub ahead of print] [ Links ]
20. Coughlin TA, Ng JW, Rollins KE, Forward DP, Ollivere BJ. Management of rib fractures in traumatic flail chest: a metaanalysis of randomised controlled trials. Bone Joint J. 2016;98-B(8):1119-25. doi: 10.1302/0301-620X.98B8.37282 [ Links ]
21. Cataneo AJ, Cataneo DC, de Oliveira FH, Arruda KA, El Dib R, de Oliveira Carvalho PE. Surgical versus nonsurgical interventions for flail chest. Cochrane Database Syst Rev. 29 Jul 2015;(7):CD009919. doi: 10.1002/14651858.CD009919.pub2 [ Links ]
22. Leinicke JA1, Elmore L, Freeman BD, Colditz GA. Operative management of rib fractures in the setting of flail chest: a systematic review and meta-analysis. Ann Surg. 2013;258(6):914-21. doi: 10.1097/SLA.0b013e3182895bb0 [ Links ]
23. Slobogean GP, MacPherson CA, Sun T, Pelletier ME, Hameed SM. Surgical fixation vs nonoperative management of flail chest: a meta-analysis. J Am Coll Surg. 2013;216(2):302-11.e1. doi: 10.1016/j.jamcollsurg.2012.10.010 [ Links ]
 Correspondence:
Correspondence:
G V Oosthuizen
george.oost@gmail.com


{kind=link}