










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.55 n.3 Cape Town Sep. 2017
GENERAL SURGERY
Predictors of emergency colectomy in patients admitted with acute severe ulcerative colitis
N N Mokhele; S R Thomson; G A Watermeyer
Division of Gastroenterology, Department of Medicine, Groote Schuur Hospital and University of Cape Town
ABSTRACT
BACKGROUND: Acute Severe Ulcerative Colitis (ASUC) is a life-threatening condition which requires urgent and aggressive medical therapy to reduce mortality, morbidity and avoid surgery. To facilitate this process, it is essential to identify patients at high risk of poor outcomes and emergency colectomy. Numerous such risk factors have been described in Western literature, however there is no local data addressing this issue. As such it is unclear if these predictors are applicable in our setting. The aim of this study is thus to identify risk factors for emergency colectomy in patients admitted to Groote Schuur Hospital with ASUC.
METHODS: A retrospective cohort study of 98 patients admitted with ASUC between January 2003 and January 2013 was performed. Clinical, demographic, laboratory and endoscopic factors on admission and 3 days thereafter were analysed as predictors of colectomy by univariate and multivariate analysis.
RESULTS: Twenty-five percent of the cohort underwent emergency colectomy. On univariate analysis, factors predicting colectomy on admission were exposure to oral corticosteroids (p=0.01), megacolon (p=0.049) or mucosal islands (p=0.04) on abdominal X-ray, and a short duration from UC diagnosis until presentation with ASUC (p=0.04). The only variable that was significantly associated with colectomy on day 3 was serum albumin (p=0.01). This was also the only variable to remain significant on multivariate analysis (OR 0.79, 95% CI 0.65-0.97, p=0.01.
CONCLUSION: ASUC is a medical emergency and predicting colectomy risk aids in therapeutic management. The only variable significantly associated with the need for surgery in our study was hypoalbuminaemia on day 3. Given the small study numbers a larger prospective study would be of value.
Introduction
Ulcerative colitis (UC) is the most common form of Inflammatory Bowel Disease (IBD). It is characterised by a relapsing and remitting course. Most episodes of active UC are mild to moderate in severity and can be managed as outpatients, however about 15% will have an acute severe flare of their disease in their lifetime, requiring admission.1 Acute severe UC (ASUC) is best defined using Truelove and Witts criteria by the presence of > 6 bloody stools per day with any of the following 4 criteria: a tachycardia (> 90 bpm), fever (> 37.8 °C), anaemia (haemoglobin < 10.5 g/dl), an elevated erythrocyte sedimentation rate (ESR) or C-reactive protein (CRP) (> 30 mm/h).2
ASUC is a medical emergency which carries a high risk of colectomy. Fortunately, the majority of cases respond rapidly to intravenous corticosteroids, which were first used as therapy in 1955. This simple intervention - together with correction of fluid and electrolyte abnormalities, treatment of concurrent infections, close monitoring by a multidisciplinary team and timely colectomy - has significantly reduced mortality rates to less than 1% in specialist units.3
In order to optimise management of this life-threatening condition, it is important to identify patients at presentation who will be at high risk of complications and may require colectomy; these individuals would then receive urgent and aggressive therapy with intravenous corticosteroids. Multiple predictors of severity in ASUC have been described. These include stool frequency, fever, tachycardia, disease extent, young age, serum albumin, haemoglobin, CRP, and extensive deep ulceration on endoscopy.3-6 In addition, megacolon and mucosal islands on plain abdominal X-ray have been described as predictors of colectomy in ASUC, conferring a 75% risk of surgery.4 Nevertheless, 30% of patients will not respond to corticosteroids and it is essential to identify these patients early so as not to prolong ineffective therapy but rather initiate salvage therapies in the form of cyclosporine or infliximab, or alternatively perform colectomy.5
Several scoring systems have been proposed to identify corticosteroid failures; the one most commonly used is the Oxford Index, whereby a stool frequency exceeding 8/day or 3-8/day plus a CRP > 45 mg/dl on the third day of corticosteroid therapy is sufficient evidence of corticosteroid failure and should prompt rescue therapy.2 The aforementioned predictors of colectomy (on admission and on day 3 of corticosteroid therapy) have been identified from cohorts in other regions of the world, mostly USA and Europe. There is no data from South Africa and it is thus unclear whether they are of value in our population. The aim of this study is thus to evaluate the role of these predictors of emergency colectomy in our IBD cohort and reflect on outcomes of ASUC in our setting.
Methods
A retrospective review of folders of all patients admitted to Groote Schuur Hospital, (Cape Town, South Africa) with a diagnosis of ASUC. The study period was from the 1 January 2003 to 31 December 2013. This study received approval from the UCT Human Research Ethics Committee.
Definitions:
ASUC was defined using the Truelove and Witts criteria: that is frequency of six or more bloody stools per day together with any one of the following criteria:
• Tachycardia (> 90 bpm)
• Temperature greater than 37.8 °C
• Anaemia (haemoglobin < 10.5 g/dl)
• An elevated ESR (> 30 mm/h) or CRP (> 30)
Corticosteroid failure was defined on day 3 of intravenous steroids by the presence of either of the following Oxford Index criteria:
• Stool frequency exceeding 8 stools per day
• 3-8 stools per day together with a CRP > 45
Inclusion criteria for the study:
• Patients admitted with a clinical diagnosis of ASUC satisfying Truelove and Witts criteria
• Patients who had undergone a colectomy, with a confirmed clinical and histological diagnosis of ASUC.
Patients with a revised secondary diagnosis within ninety days were excluded.
Patients were identified from inpatient admission records, surgical files, as well as an established IBD database. All patients admitted to a medical ward were treated with intravenous corticosteroids at standard doses. Data collected included baseline demographics (age, gender, family history, ethnicity, smoking status, duration of UC prior to ASUC diagnosis, time from diagnosis to presentation, and medication exposure on admission). Clinical, biochemical, laboratory variables, radiological and sigmoidoscopy findings on admission and on day 3 of intravenous corticosteroids were also extracted, as were indications for colectomy and 90 day outcomes. Outcome measures assessed were death within 90 days of presentation, colectomy free survival at 90 days and surgical complications.
Statistical analysis
The distribution of all continuous variables was evaluated and expressed as medians and interquartile ranges (IQRs) or means ± standard deviations (SD) as appropriate. Statistical analysis employed Chi2, Fishers exact, Student t-test, Wilcoxon rank sum test or Kruskal-Wallis testing as appropriate. Those variables with P values below 0.10 were further tested in a series of logistic multivariate regression models. The analysis was performed using STATA version 11 (StataCorp. 2009. Stata Statistical Software: Release 11. College Station, TX: StataCorp LP).
Results
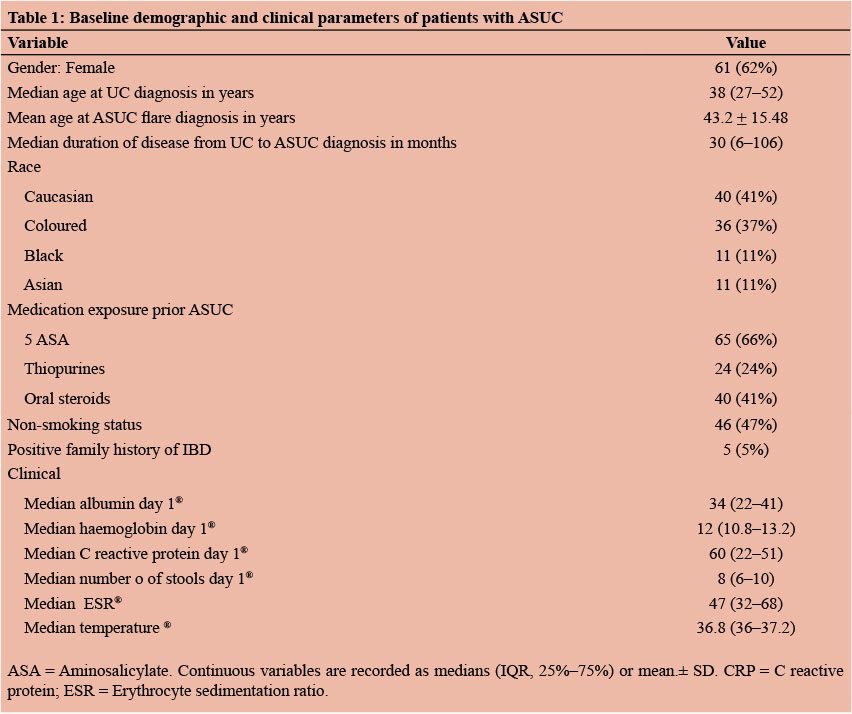
Ninety-eight (98) patients with ASUC were eligible for study inclusion. Sixty four percent (64%) were female. The mean age at first diagnosis of UC was 39 years and the mean age at the time of the ASUC flare was 43 years; only 47% were older than 40 years of age at the time of the attack. The mean duration between diagnosis and admission for ASUC was 61 months. For 17% this was the first presentation of their disease. All the patients had extensive colitis. Forty-one percent (41%) of the cohort were Caucasian, 37% Coloured, 11% Asian and 11% Black. With regards to medication use at the time of admission: 76% were using 5-aminosalicylates (5-ASAs) and 26% thiopurines; none were receiving maintenance biologics. Only 5% of patients had a positive family history of IBD. Overall 47% were non-smokers. These baseline demographics are presented in Table 1. On initial work-up only 1 patient (who did not require colectomy) had concurrent Clostridium difficile infection and was treated with metronidazole with good effect. No cases of cytomegalovirus were detected.
Twenty five (25) of the 98 patients (25%) underwent a colectomy during the study period, 64% were female which was similar to patients who did not require surgery (Table 2). Eighty percent (80%) of patients had their emergency colectomy within 15 days of admission; only half of these were operated on within 7 days. Thirty-eight percent (38%) of patients had complications within 90 days post admission which included sepsis (pneumonia, wound sepsis). There were no deaths within the 90 day follow-up period. Of patients undergoing colectomy 52% were of Caucasian ethnicity, 40% were Coloured, and 8% Asian. None of the black patients required surgery. There was no significant association between colectomy and ethnicity. The mean age of patients at colectomy was 39 years which was not significantly different from those who did not require colectomy. The group of patients undergoing surgery for ASUC had a significantly shorter duration of disease than those in whom colectomy was avoided; 16 months and 41 months respectively (p=0.04).
On univariate analysis, non-smoking status was not associated with an increased risk of colectomy, nor was a positive family history of IBD or exposure to 5-ASAs or thiopurines (Table 2). In contrast, patients requiring colectomy were significantly more likely to have received treatment with oral corticosteroids than those who avoided surgery (p=0.01). None of the patients were on maintenance Infliximab at the time of ASUC admission, however 4 patients received Infliximab as rescue therapy and all of them avoided colectomy. On univariate analysis, there was no significant difference with regards to any of the baseline laboratory or clinical variables (median number of stools per day, body temperature, haemoglobin, serum albumin, or CRP) when comparing patients requiring colectomy with those who did not (Table 3). In contrast, radiologic evidence of megacolon or mucosal islands on abdominal X-ray were significantly more likely to be present in subjects requiring surgery than in those who did not (32% and 40% respectively).
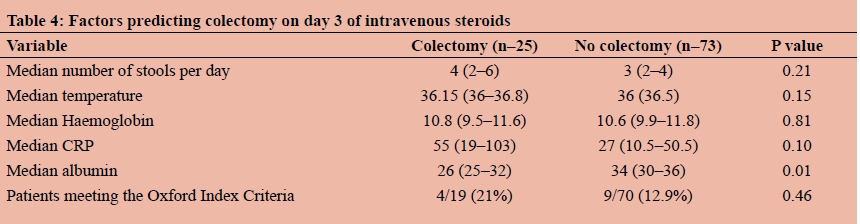
Analysis of day 3 data showed that serum albumin was significantly associated with the need for colectomy (p=0.01). In contrast, all the other variables analysed at this time point (haemoglobin, temperature, and CRP) did not correlate significantly with the risk of colectomy (Table 4). Furthermore, patients meeting the Oxford Index criteria for corticosteroid failure on day 3 were no more likely to require colectomy than those who did not. On multivariate logistic regression, only serum albumin on day 3 was significantly associated with colectomy (OR 0.79, 95% CI 0.65-0.97, p=0.003).
Discussion
Acute severe ulcerative colitis is a medical emergency because of the risk of colonic perforation. Prompt recognition and timely medical or surgical intervention within the setting of a multidisciplinary team is crucial to reduce morbidity and mortality.1 In order to optimise care and facilitate aggressive management strategies, there is an urgent need to identify patients at very high risk for colectomy. As a consequence, the role of prognostic factors in patients with ASUC has been the subject of much interest.
Multiple predictors of severity have been described. Among objective clinical features, bloody stool frequency, increased body temperature and tachycardia are good predictors of severity and outcome.1 In a retrospective study of 166 patients, a stool frequency of more than 12 per day conferred a 55% risk of colectomy.2 Laboratory markers have also been studied extensively with varying degrees of success. The widely used acute phase reactant CRP has established value in ASUC in both adults and children.1 Serum albumin may also be predictive; in a retrospective study of 189 admissions hypoalbuminaemia (serum albumin less than 30 g/l) on the first day of admission was associated with a 42% risk of colectomy.4 However, results from multiple prospective studies have shown less convincing results.
Radiological findings, which include megacolon (transverse colon dilatation of > 5.5 cm), thumb printing (suggestive of mucosal oedema), the presence of mucosal islands and features of a small bowel ileus, are also predictors of severity in UC.2 Megacolon and mucosal islands on plain abdominal X-ray have been shown to confer a 75% risk of colectomy.4 Disease extent is also an important predictor of the need for surgical intervention; patients with extensive colitis have a risk 4 times higher than those with limited UC. Deep ulceration on endoscopy is also an ominous sign in ASUC; 93% will require surgery.6,7 Patients who present with a disease flare and any of these risk factors require immediate admission and urgent intervention.
Intravenous corticosteroids are the mainstay of therapy. Nevertheless, 30% of patients will fail to respond to corticosteroids and it is essential to identify these patients early so as not to prolong ineffective therapy but rather initiate salvage therapies in the form of cyclosporine or infliximab, or alternatively perform colectomy.2 Colectomy is a lifesaving intervention and the ability to predict the need for surgery and its timing is key to decreasing morbidity and surgical complications. Response to steroids should be assessed at day 3 of admission and partial or non-responders considered for rescue medical therapy or surgery. Several scoring systems have been proposed to identify corticosteroid failures; the one most commonly used is the Oxford Index, whereby a stool frequency exceeding 8/day or 3-8/day plus a CRP > 45 mg/ dl on the third day of corticosteroid therapy is considered sufficient evidence of corticosteroid failure and should prompt rescue therapy.2 Colectomy is indicated from 4-7 days after rescue therapy in non-responders. Prolonged medical therapy in refractory systemic ill patients results in poor outcomes, if surgery is delayed.8
Our study evaluated all of these aforementioned risk factors and has identified several which significantly predict colectomy during admission for ASUC. First, a shorter duration of disease conferred a higher risk of subsequent surgery than patients with a longer duration of disease. This is in keeping with other publications which show that most severe attacks of UC occur within 3 months of diagnosis.6 In our study the use of thiopurines and 5-ASAs did not impact on colectomy rates. In contrast (and not surprisingly), patients who were already on oral steroids on admission were more likely to undergo colectomy. This has been described previously and oral corticosteroids are a well described risk factor for colectomy in ASUC.9 It is common practise in our institution to admit patients who have failed to respond to oral steroids and give them a trial of intravenous therapy. These individuals likely have more severe UC and have already shown themselves to be (at least partially) steroid refractory. As such, they would inherently be at greater risk of needing emergency surgery.9,10
All other baseline demographics were not significantly associated with the risk of colectomy. Interestingly, most of the ASUC patients were female. This is not in keeping with international literature which reports a male predominance, with a male to female ratio of 36:16.11,12 Of interest is the 0% colectomy rate in the black population; this likely reflects the small numbers included but merits further evaluation. With regards to baseline laboratory investigations, none were shown to increase the risk of colectomy. This is at odds with what is reported in the literature where the risk of colectomy increases as more Truelove and Witts criteria are fulfilled.13 As such, it appears logical that baseline haemoglobin and CRP levels would be of value. Similarly a low serum albumin on presentation is a well described predictor of the need for surgery.14 Serum albumin levels on admission did not predict colectomy in our study, however hypoalbuminaemia on day 3 was significantly associated with an increased need for surgery. This was the only variable that remained statistically significant on multivariate analysis and likely reflects ongoing, severe inflammation which has failed to respond to corticosteroids and which should prompt escalation of therapy.
There are some other interesting observations which have emerged from this study. The first is the 100% success rate of infliximab in patients failing corticosteroids. Although numbers were small, this suggests that appropriate patients are being selected. Another observation which is somewhat disturbing is that 40% of patients had their colectomy between 8 and 15 days of admission. It is unclear why surgery was delayed in these individuals but this could explain the high incidence of post-operative complications. It is well described in the literature that delaying surgery is associated with higher morbidity and mortality in ASUC.8
This study has several weaknesses, mostly as a consequence of its retrospective design. Due to inconsistent documentation of admission data in both medical and surgical wards, it is likely that some cases of ASUC would have been overlooked. However, this data is likely missing at random and should not impact study results to any great extent. This is supported by our colectomy rate of 25 % which is in keeping with that reported in the world literature. 15 A second study weakness is the relatively small numbers of study subjects. This could have led to a Type 11 error which could explain the lack of significance of many of the variables analysed on presentation and on day 3 (notably the Oxford index of severity). A prospective cohort is highly recommended.
Conclusion
ASUC is a medical emergency. Predicting which patients will likely require colectomy is a very valuable tool in guiding therapeutic management. In our study, the only variable significantly associated with colectomy was hypoalbuminaemia on day 3. However, given the small study numbers a larger prospective study would be of value in identifying additional risk factors.
REFERENCES
1. Doherty GA, Cheifetz AS. Management of acute severe ulcerative colitis. Expert Rev Gastroenterol Hepatol. 2009;3(4):395-405. doi:10.1586/egh.09.24 [ Links ]
2. Travis SP, Farrant JM, Ricketts C, et al. Predicting outcome in severe ulcerative colitis. Gut. 1996;38(6):905-910. doi: 10.1136/gut.38.6.905 [ Links ]
3. Macken L, Blaker PA. Management of acute severe ulcerative colitis. Clin Med (Northfield Il). 2015;15(5):473-476. doi: 10.1136/gut.2009.192765 [ Links ]
4. Lennard-Jones JE, Ritchie JK, Hilder W, et al. Assessment of severity in colitis: a preliminary study. Gut. 1975;16(8):579-584. doi: 10.1136/gut16.8.579 [ Links ]
5. Mowat C, Cole A, Windsor A, Ahmad T, et al. Guidelines for the management of inflammatory bowel disease in adults. Gut. 2011;60(5):571-607. doi: 10.1136/gut.2010.224154 [ Links ]
6. Solberg IC, Lygren I, Jahnsen J, et al. Clinical course during the first 10 years of ulcerative colitis: results from a population-based inception cohort (IBSEN Study). Scand J Gastroenterol. 2009;44(4):431-40. doi: 10.1080/00365520802600961 [ Links ]
7. Daperno M, Sostegni R, Scaglione N, et al. Outcome of a conservative approach in severe ulcerative colitis. Dig Liver Dis. 2004;36(1):21-8. doi: 10.1016/j.dld.2003.04.001 [ Links ]
8. Randall J, Singh B, Warren BF, et al. Delayed surgery for acute severe colitis is associated with increased risk of postoperative complications. Br J Surg. 2010;97(3):404-9. doi: 10.1002/ bjs.6874 [ Links ]
9. Lindgren SC, Flood LM, Kilander AF, et al. Early predictors of glucocorticosteroid treatment failure in severe and moderately severe attacks of ulcerative colitis. Eur J Gastroenterol Hepatol. 1998;10(10):831-6. [ Links ]
10. Kuriyama M, Kato J, Fujimoto T, et al. Risk factors and indications for colectomy in ulcerative colitis patients are different according to patient's clinical background. Dis Colon Rectum. 2006;49(9):1307-15. doi: 10.1007/s10350-006-0574-6 [ Links ]
11. Gibson DJ, Rafter N, Keegan D, et al. Predictors of colectomy in hospitalised patients with acute severe colitis. Gut. ;62(2):A36-A37. doi: 10.1136/gutjnl-2013-305143.88 [ Links ]
12. Subramaniam K, Richardson A, Dodd J, et al. Early predictors of colectomy and long-term maintenance of remission in ulcerative colitis patients treated using anti-tumour necrosis factor therapy. Intern Med J. 2014;49(9):1307-15. doi: 10.1111/ imj.12397 [ Links ]
13. Truelove SC, Witts LJ. Cortisone in ulcerative colitis; final report on a therapeutic trial. Br Med J. 1955;2(4947):1041-8. doi: 10.1159/000199983 [ Links ]
14. Ho GT, Mowat C, Goddard CJR, et al. Predicting the outcome of severe ulcerative colitis: development of a novel risk score to aid early selection of patients for second-line medical therapy or surgery. Aliment Pharmacol Ther. 2004;19(10):1079-87. doi: 10.1111/j.1365-2036.2004.01945.x [ Links ]
15. Aratari A, Papi C, Clemente V, et al. Colectomy rate in acute severe ulcerative colitis in the infliximab era. Dig Liver Dis. 2008;40(10):821-6. doi: 10.1016/j,dld.2008.03.014 [ Links ]


{kind=link}
{kind=link}
{kind=link}
{kind=link}