










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Surgery
versión On-line ISSN 2078-5151
versión impresa ISSN 0038-2361
S. Afr. j. surg. vol.55 no.3 Cape Town sep. 2017
GENERAL SURGERY
What is the diagnostic yield of colonoscopy in patients with a referral diagnosis of constipation in South Africa?
M MjoliI, II; V GovindasamyI, II; T E MadibaII, III
IDepartment of Surgery, Greys Hospital, Pietermaritzburg, South Africa
IIDepartment of Surgery, University of KwaZulu-Natal, Durban, South Africa
IIIGastrointestinal Cancer Reserch Centre, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: Constipation is a common problem for referral to surgical and colorectal units. Its association with colorectal cancer is controversial. Some authors have found an increased incidence while others have not. The aim of this study is to investigate the incidence of colorectal cancer (CRC) and other significant colonoscopic pathologies in patients undergoing colonoscopy for constipation.
METHODS: All colonoscopy reports for constipation were retrieved from our database from January 2011 to 30 June 2014. Data extracted included demographics, colonoscopic findings and adequacy of bowel preparation. Exclusion criteria included patients with other symptoms known to be associated with colonic neoplasia such as lower GIT bleeding, loss of weight, patients with associated anaemia, those with abnormalities on imaging, patients with personal or family history of colorectal cancers or colorectal polyps and patients with inflammatory bowel disease. The primary outcome was the presence of neoplasia at colonoscopy and the secondary outcomes were other colonoscopy findings.
RESULTS: A total of 985 colonoscopies were performed from January 2011 to June 2014 of which 144 were done for a referral diagnosis of constipation. Eighty eight (61.1%) were female. Their mean age was 58.6 + 13.8 years (range 19-95 years). There were 61 (42.4%) African patients, 38 (26.4%) White, 33 (22.9%) Asians and 12 (8.3%) Coloured patients. Eighty seven (60.4%) patients had a normal colonoscopy, 20 (13.9%) diverticular disease, 14 (9.7%) polyps of which 6 (4.2%) were neoplastic, and 9 (6.3%) had colorectal cancer.
CONCLUSIONS: Constipation is associated with CRC. The presence of constipation should be a criterion for colonoscopy regardless of age or any other associated clinical features.
Keywords: Constipation, Colonoscopy, colorectal cancer, adenoma, colorectal polyp.
Introduction
Constipation is a common referral diagnosis to surgical and colorectal units and its prevalence and relationship to colorectal cancer (CRC) has not been studied in South Africa. The association of constipation and colorectal cancer is highly variable. Some reports have found an increased incidence of colorectal cancer in patients with constipation13 speculating that prolonged bowel transit exposes the colon mucosa to carcinogens in the stool and leads to increased risk of developing neoplasia.4 Other studies have not shown this increased incidence.58 whilst some studies have found an association between loose stool and an increased CRC risk.9
Locally, colonoscopy is used to investigate patients with a referral diagnosis without any selection criteria or guidelines.
This study aims to investigate the incidence of CRC and other significant pathological findings at colonoscopy in patients referred for constipation as the only clinical feature.
Methods
All colonoscopy reports for patients who underwent a colonoscopy for constipation were retrieved from our prospective electronic database. The period of this study was from January 2011 to 30 June 2014. All colonoscopies were performed by 3 surgeons: a colorectal surgeon, a general surgeon with a colorectal interest and a colorectal fellow. All three surgeons did roughly the same number of colonoscopies. Exclusion criteria included patients with other symptoms known to be associated with colonic neoplasia such as lower GIT bleeding, loss of weight, patients with associated anaemia, those with abnormalities on imaging, patients with personal or family history of colorectal cancers or colorectal polyps and patients with inflammatory bowel disease.
Data extracted included demographics, adequacy of bowel preparation, and colonoscopic findings. The patient's race was classified as African, White, Asian and Coloured (mixed race) according to the South African Population Registration Act.10 The race of the patient was determined by the health professional during the consultation. This was both by self-declaration and assessment by the health professional. The terminology used is that described in the South African Population Registry, i.e. White, Indian, Coloured and Black, rather than Caucasian, African, Asian and Mixed. The primary outcome was the presence of neoplasia at colonoscopy. Secondary outcomes were other colonoscopic findings including a normal colonoscopy.
Results
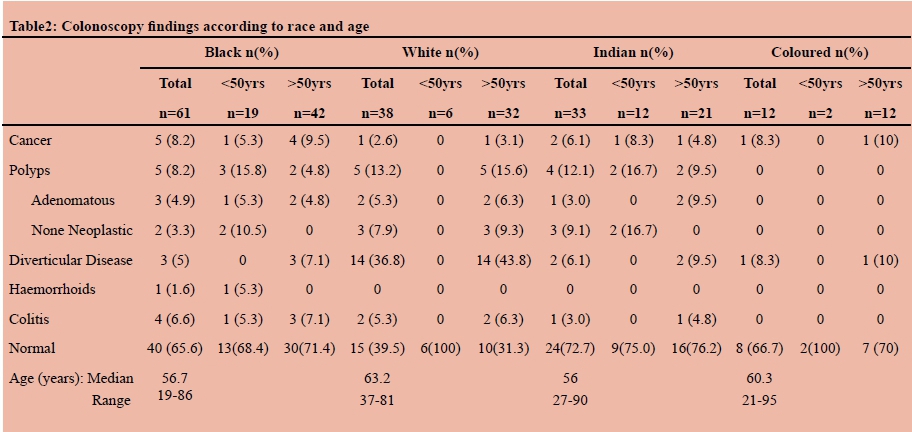
There were 985 patients from January 2011 to June 2014 who underwent colonoscopy. Of these 144, of mean age 58.6 + 13.8 years, were referred for a diagnosis of constipation and they form the basis of this study. Eighty eight (61.1%) werefemale (M:F ratio 1:1.6). There were 61 (42.4%) African, 38 (26.4%) White, 33 (22.9%) Asian and 12 (8.3%) Coloured patients. The median ages (range) were 57 (19-86 years) for African, 63 (37-81) for Whites, 56 (27-90) for Indians and 60 (21-95) for Coloureds. Thirty nine (27.1%) were below the age of 50 years and 105 (72.9%) older than 50 years.
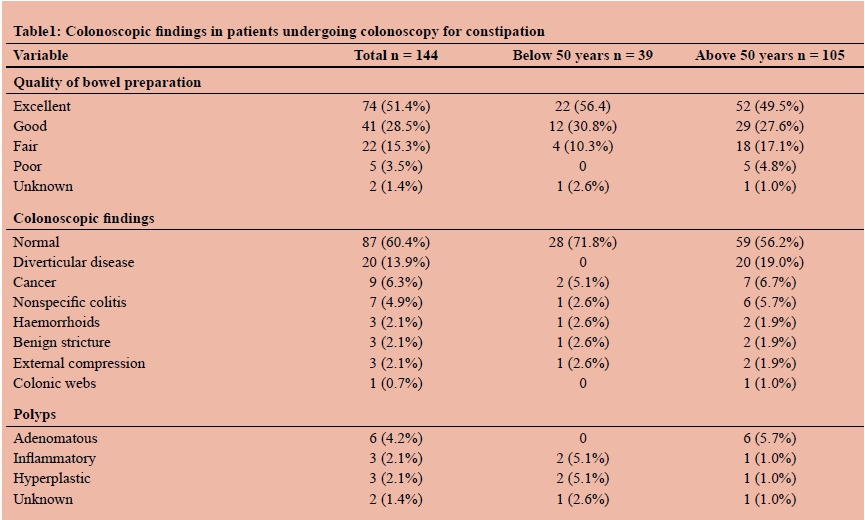
Eighty seven patients had a normal colonoscopy. The colonoscopic findings are shown in Table 1 and Table 2. The quality of colonoscopy preparation was ranked excellent in the majority of cases. The most common findings at colonoscopy were diverticular disease (20) polyps (14) and colorectal cancer (9). Adenomatous polyps were seen only in patients > 50 years of age. CRC was found in both patients of age < 50 years and > 50 years and was seen in all population groups. The most commonly observed non-neoplastic condition was diverticular disease, seen in only older patients.
Discussion
Colonoscopy has been shown to be the method of choice to screen and detect early colorectal cancer (CRC).9 Although alteration in bowel habits is one of the important manifestations of this disease, the association of constipation and colorectal cancer remains controversial. Even though the evidence is scanty, constipation has been shown to be uncommon in Africa. A Nigerian study showed the prevalence of constipation to be low.11 In rural Nigeria it was 0.8%, while in urban Nigeria it was 2.8%.11 The worldwide prevalence of constipation is estimated to be 14% in first world countries.12 High risk groups include the elderly with incidence ranging from 40% to 74%.13,14 Many studies show that constipation is poorly predictive of colorectal cancer.5-8,15 Even in low prevalence regions such as ours, constipation has been shown to be a poor predictor of colorectal cancer.16
The proportion of patients with adenomatous polyps was 4.2%. This is lower than the 5.5-19.6% reported in the literature.7,15 However, when patients > 50 years of age are considered, the figure of 5.7% approaches that reported in the literature. Angelo and Dreyer17 observed in 2001 that adenomatous polyps among Africans, previously considered rare, were seen more frequently than a decade earlier and were occurring in proportions similar to that seen in their White counterparts. The incidence of adenomatous polyps between African and White patients is similar in this study with 4.9% and 5.3% respectively. In the White population, adenomatous polyps occur exclusively in the older than 50-years age group, whereas in the African population they occur in both the younger and older age groups. The increase in the prevalence of adenomatous polyps seen among Africans as reported by Angelo17 and confirmed in our study suggest that colonoscopy for constipation may be as relevant in Africans as it is in the White population group.
The CRC prevalence of 6.3% in this series was much higher than the 0-1.7% reported in the literature.7,15 African studies have shown a low but increasing incidence of CRC in African patients in South Africa and Africa.1820 This increase is expected to continue in the future. This can be presumed by the fact that Africans residing in high incidence areas such as America have a much higher incidence than Africans in Africa.18,21 In fact, the incidence of CRC in African Americans is higher than that of White Americans.22
Africa and South-Central Asia have the lowest incidence of colorectal cancer in the world and the highest rates are seen in Australia and New Zealand where they may be up to 45.7/100 000 population.23 Though the incidence of CRC is not well studied in Africa, it is estimated to be 4.04 per 100 000 population in Sub-Saharan Africa.24 South Africa, which presumably has the most reliable cancer registries in Sub-Saharan Africa, has an even lower incidence of 3.7 per 100 000.24,25 In such low incidence areas, the selection of symptomatic patients, such as those with constipation, could be used to increase the diagnostic yield for CRC. Furthermore, the prevalence of CRC detected at colonoscopy in patients referred for constipation was similar in both patients younger than 50 years and those older than 50 years at 5.1% and 6.7% respectively. Intuitively one would expect a higher incidence in the older age group. This paradox is, however, not surprising since local evidence and other African studies suggest a higher proportion of young patients with CRC.26-29
Young African patients seem to have a higher risk of CRC even when compared to African Americans.21 There are concerns regarding the accuracy of CRC data emanating from registries in South Africa and the rest of Africa with some authorities suggesting that the low incidence may be exaggerated by under-reporting and missed diagnosis, under-diagnosis due to poor access to health care centres or may be influenced by the low life expectancy reported in Africa.25 Despite these concerns we think that the low incidence of colorectal cancer is accurate as these findings have been shown consistently over the past two to three decades.20,24,26,27,30,31 Though the incidence remains low, an increasing prevalence has been noted locally and in other African countries during this same period.17,19,20 Some authors have attributed this increase to one or a combination of factors, including change in dietary habits (to western diet), increased awareness of the population to cancer, increasing lifespan, increased accessibility of health services, and improved socioeconomic status.19 This increasing prevalence needs to be verified by more studies.
An interesting subject in the literature of CRC is the comparison between African patients and other races, especially Whites. In this study, the number of patients is too low to make such comparisons. In South Africa, there are no studies comparing CRC in all the different race groups and only a few studies compare Africans to White patients.1718,24,28,29,32 Segal et al. have shown that in South Africa, CRC is different among African and White patients. They noted that CRC among White patients was similar to that seen in western countries with respect to incidence' distribution, sex ratio, and synchronous lesions; in the African population' CRC was uncommon and presented late with advanced disease, with absence of synchronous adenomatous polyps and cancers and absence of diverticular disease, and was associated with a high fibre and low meat and fat diet.32 Because of these differences, they postulated that the pathogenesis of CRC in Black and White South African patients was likely to be different.32 Anderson et al. also recognized these differences and identified that there is a need for further studies to understand these racial variations.18 The racial distribution in this study is different to what would be expected for the provincial racial distribution. According to the 2013 mid-year population estimates, Africans represent 80% of the KwaZulu-Natal province, followed by Indians, Whites and Coloureds at 8%, 4% and 2.5% respectively.23 In this study, the racial distribution was 42.4%, 22.9%, 26.4% and 8.3% respectively. The African representation is half of the expected representation and Indians, Whites and Coloured have a higher representation with a factor of 2.9, 6.6 and 4.9 respectively. This probably shows that constipation is low in Africans and higher in Indians, Whites and Coloureds. This is probably related to the dietary habits, but may also be related to their perception of their bowel habits and attitudes towards seeking medical advice for their perceived constipation.
International guidelines do not recommend the use of colonoscopy for the investigation of constipation unless it is of recent onset or associated with other symptoms of CRC, i.e. blood in stool, weight loss, anaemia, family history of CRC.33,34 Lambert et al. go as far as to suggest that developing countries, where the incidence of CRC is low, should not even have a screening programme because the risk of CRC is so low.35
Despite these recommendations there are numerous reports of CRC occurring in the young and unsuspected patients with constipation.36-38 Such case reports make it difficult not to investigate patients presenting with constipation with a colonoscopy. Our own case series suggests that constipation is an important manifestation of CRC or at least an association. We therefore do not share the view that does not recommend colonoscopy in patients with constipation. The prevalence of 17.9% of neoplastic pathology with a 6.5% incidence of CRC in this series cannot be ignored. We agree with Lambert et al. that populations with a low incidence of CRC do not warrant a colonoscopy for a screening program for CRC. However, we do not agree with their other recommendations that colonoscopy should not be used to assess constipations. We believe that patients should have a colonoscopy to assess colorectal symptoms including constipation. We would advise that patients with constipation have a colonoscopy or some other form of screening for colorectal cancer.
The most commonly detected benign disease in this series was diverticular disease at 13.9%, but it was still lower than the 33.6% reported by others.7 The fact that it was seen only in the older age group is not surprising as this is a disease of increasing age and with constipation as one of its clinical features. It was also of interest that diverticular disease was more commonly seen in White patients.
There are several limitations to our study. It is a retrospective study and the sample size is small. Criteria for constipation were not clearly defined. Quality markers for colonoscopy, such as caecal intubation rate and duration of withdrawal, were not documented. A detailed enquiry regarding the risk of CRC was not taken. A possibility exists that a higher porotion of lesions may be missed by a fellow who is in training. However, fellows in our institution are experienced as they have been qualified as general surgeons for some time before entering the colorectal fellowship program. Any further planned studies on this topic should consider these factors.
In conclusion, the prevalence of CRC in patients with constipation is significant. Until further prospective trials are available in our patient population, constipation should be treated as an indication for colonoscopy regardless of age or any other clinical features.
Conflict of Interest
None
REFERENCES
1. Watanabe T, Nakaya N, Kurashima K, Kuriyama S, Tsubono Y, Tsuji I. Constipation, laxative use and risk of colorectal cancer: The Miyagi Cohort Study. Eur J Cancer. 2004;40(14):2109-15. [ Links ]
2. Tashiro N, Budhathoki S, Ohnaka K, Toyomura K, Kono S, Ueki T, et al. Constipation and colorectal cancer risk: the Fukuoka Colorectal Cancer Study. Asian Pac J Cancer Prev. 2011;12(8):2025-30. [ Links ]
3. Guerin A, Mody R, Fok B, Lasch KL, Zhou Z, Wu EQ, et al. Risk of developing colorectal cancer and benign colorectal neoplasm in patients with chronic constipation. Aliment Pharmacol Ther. 2014;40(1):83-92. [ Links ]
4. Cummings JH, Bingham SA, Heaton KW, Eastwood MA. Fecal weight, colon cancer risk, and dietary intake of nonstarch polysaccharides (dietary fiber). Gastroenterology. 1992;103(6):1783-9. [ Links ]
5. Adelstein BA, Macaskill P, Chan SF, Katelaris PH, Irwig L. Most bowel cancer symptoms do not indicate colorectal cancer and polyps: a systematic review. BMC gastroenterol. 2011;11:65. [ Links ]
6. Astin M, Griffin T, Neal RD, Rose P, Hamilton W. The diagnostic value of symptoms for olorectal cancer in primary care: a systematic review. Br J Gen Pract. 2011;61(586):e231-43. [ Links ]
7. Obusez EC, Lian L, Kariv R, Burke CA, Shen B. Diagnostic yield of colonoscopy for constipation as the sole indication. Colorectal Dis. 2012;14(5):585-91. [ Links ]
8. Power AM, Talley NJ, Ford AC. Association between constipation and colorectal cancer: systematic review and meta-analysis of observational studies. Am J Gastroenterol. 2013;108(6):894-903; quiz 4. [ Links ]
9. Park JY, Mitrou PN, Luben R, Khaw KT, Bingham SA. Is bowel habit linked to colorectal cancer? Results from the EPIC- Norfolk study. Eur. J. Cancer. 2009;45(1):139-45. [ Links ]
10. Interior Mot. Population Registration Act, 1950 Wikipedia7 July 1950 [cited 2014 31/10/2014]. Available from: http://en.wikipedia.org/wiki/Population_Registration_Act,_1950. [ Links ]
11. Daniyam CA, Malu AO, Okeke EN, Lawal OO. Bowel habits of urban and rural populations on the Jos, Plateau, Nigeria. West Afr J Med. 2011;30(3):182-7. [ Links ]
12. Suares NC, Ford AC. Prevalence of, and risk factors for, chronic idiopathic constipation in the community: systematic review and meta-analysis. Am J Gastroenterol. 2011;106(9):1582-91; quiz 1, 92. [ Links ]
13. Rao SS, Go JT. Update on the management of constipation in the elderly: new treatment options. Clin Interv Aging. 2010;5:163-71. [ Links ]
14. Talley NJ, Fleming KC, Evans JM, O'Keefe EA, Weaver AL, Zinsmeister AR, et al. Constipation in an elderly community: a study of prevalence and potential risk factors. Am J Gastroenterol. 1996;91(1):19-25. [ Links ]
15. Pepin C, Ladabaum U. The yield of lower endoscopy in patients with constipation: survey of a university hospital, a public county hospital, and a Veterans Administration medical center. Gastrointest Endosc. 2002;56(3):325-32. [ Links ]
16. Gupta M, Holub J, Knigge K, Eissen G. Constipation is not associated with an increased rate of findings on colonoscopy: result from a national endoscopy consortium. Endoscopy. 2010;42(3). [ Links ]
17. Angelo N, Dryer L. Colorectal Carcinoma - A new threat to black pateints? A retrospective analysis of colorectal carcinoma received by the institute for pathology, University of Pretoria. SAMJ. 2001;91:689-93. [ Links ]
18. Anderson W, Umar A, Brawley O. Colorectal carcinoma in black and white race. Cancer Metast Rev. 2003;22:67-82. [ Links ]
19. Iliyasu Y, Ladipo JK, Akang EE, Adebamowo CA, Ajao OG, Aghadiuno PU. A twenty-year review of malignant colorectal neoplasms at University College Hospital, Ibadan, Nigeria. Dis Colon Rectum. 1996;39(5):536-40. [ Links ]
20. Saidi H, Nyaim EO, Githaiga JW, Karuri D. CRC surgery trends in Kenya, 1993-2005. World J Surg. 2008;32(2):217-23. [ Links ]
21. Olufemi Williams A, Chung E, Agbata A, Jackson M. Intestinal polyps in American Negroes and Nigerian Africans. Br J Cancer. 1975;31:485. [ Links ]
22. Ahnen D, Macrae F. Colorectal cancer: Epidemiology, risk factors and protective factors: Uptodate; 2014 [updated 30/09/2014; cited 2014 05/11/2014]. Available from: http://www.uptodate.com/contents/colorectal-cancer-epidemiology-risk-factors-and-protective-factors?source=search_result&search=COLORECTAL+CANCER& selectedTitle=3%7E150. [ Links ]
23. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69-90. [ Links ]
24. Graham A, Adeloye D, Grant L, Theodoratou E, Campbell H. Estimating the incidence of colorectal cancer in Sub-Saharan Africa: A systematic analysis. J Glob Health. 2012;2(2):020404. [ Links ]
25. Wentink MQ, Rakers M, Stupart DA, Algar U, Ramesar R, Goldberg PA. Incidence and histological features of colorectal cancer in the Northern Cape Province, South Africa. SAJS. 2010;48(4):109-13. [ Links ]
26. Abdulkareem FB, Abudu EK, Awolola NA, Elesha SO, Rotimi O, Akinde OR, et al. Colorectal carcinoma in Lagos and Sagamu, Southwest Nigeria: a histopathological review. World J Gastroenterol. 2008;14(42):6531-5. [ Links ]
27. Abou-Zeid AA, Khafagy W, Marzouk DM, Alaa A, Mostafa I, Ela MA. Colorectal cancer in Egypt. Dis Colon Rectum. 2002;45(9):1255-60. [ Links ]
28. Moolla Z, Madiba TE. Trends in demographics and management of obstructing colorectal cancer. World J Surg. 2014;38(9):2466-70. [ Links ]
29. Zulu B, Madiba TE. Colorectal cancer in KwaZulu-Natal: an established disease with a variable clinicopathological spectrum. SAJS. 2011;49(2):92-3. [ Links ]
30. Holcombe C, Babayo U. The pattern of malignant disease in north east Nigeria. Trop Geogr Med. 1991;43(1-2):189-92. [ Links ]
31. El Mistiri M, Verdecchia A, Rashid I, El Sahli N, El Mangush M, Federico M. Cancer incidence in eastern Libya: the first report from the Benghazi Cancer Registry, 2003. Int J Cancer. 2007;120(2):392-7. [ Links ]
32. Segal I, Cooke S, Hamilton D, Tim L. Polyps and colorectal cancer in South African Blacks. Gut. 1981;22:653-7. [ Links ]
33. Ternent CA, Bastawrous AL, Morin NA, Ellis CN, Hyman NH, Buie WD. Practice parameters for the evaluation and management of constipation. Dis Colon Rectum. 2007;50(12):2013-22. [ Links ]
34. Levin B, Lieberman DA, McFarland B, Smith RA, Brooks D, Andrews KS, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US MultiSociety Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin. 2008;58(3):130-60. [ Links ]
35. Lambert R, Sauvaget C, Sankaranarayanan R. Mass screening for colorectal cancer is not justified in most developing countries. Int J Cancer. 2009;125(2):253-6. [ Links ]
36. Schussele Filliettaz S, Gonvers JJ, Peytremann-Bridevaux I, Arditi C, Delvaux M, Numans ME, et al. Appropriateness of colonoscopy in Europe (EPAGE II). Functional bowel disorders: pain, constipation and bloating. Endoscopy. 2009;41(3):234-9. [ Links ]
37. Triadafilopoulos G, Lombard CM. Multiple rectal polyps in a young woman with constipation. Dig Dis Sci. 2010;55(4):890-4. [ Links ]
38. Muley P, Mhapsekar RV, Kumar RM. Constipation in children -is it always benign? Colorectal Dis. 2012;14(5):e272-3. [ Links ]
 Correspondence:
Correspondence:
Monde Dennis Mjoli
mmjoli@yahoo.com


{kind=link}
{kind=link}