










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.55 n.1 Cape Town Mar. 2017
LETTERS TO THE EDITOR
S ChowdhuryI; P NavsariaII; S EduII; A J NicolII
IDepartment of Surgery, University of Cape Town
IIGroote Schuur Hospital Trauma Centre, University of Cape Town
We would like to thank Dr Hodkinson and colleagues for their interest and comments on our paper.1 We did not mention in our article that response time (RT) should be used as the sole indicator to assess the effectiveness of emergency medical services (EMS), but rather as an indicator of EMS performance. We agree that the measurement of the efficiency of any service is a complex and multifactorial issue.
Dr Hodkinson indicates that we have ignored the greatly increased injury to theatre time, and time between arrival of the patient at the Groote Schuur Hospital Trauma Centre (GSHTC) and theatre. We disagree with their remarks that we concluded by implicating EMS response time although it was by far the shortest and most significant time frame (32 minutes) difference between the complications vs non-complications groups involved (P < 0.01). Thirty two minutes is enough to make a bleeding trauma patient unstable and to have a worse outcome if the patient is left unattended at the scene. Every minute is critical for bleeding trauma patients.
If they look at our results carefully, we mentioned that the median delay from the injury to the theatre was also a significant factor in the development of complications (P = 0.02) but the delay from the arrival to GSHTC to the theatre did not show a significant difference between both groups of patients (P = 0.27). We explained these findings in the discussion section.
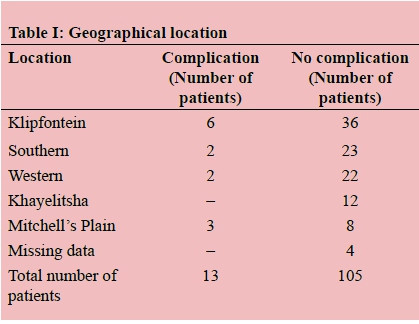
Dr Hodkinson claims that there was no consideration of the geographic location of cases, the initial incident description, call prioritisation, the workload of EMS at the time of the case received, or indeed the workload of the GSHTC and its care process, although we explicitly mentioned in the methods section that the geographical area was considered. We removed the findings from the results section during editing to shorten the article. The geographic location is presented in Table I.
We know that trauma is a significant burden in South Africa and adds a huge workload to our EMS system. We have no doubt that the Cape Town EMS is the best-resourced and most efficient EMS in the public sector on the continent. Instead of blaming EMS we made a recommendation in our article to government and private entrepreneurs to increase the prehospital personnel as well as improve logistics to meet current international standards.
Research on South African prehospital setting is urgently needed as there are scant published data. We recognise the good work that EMS does in South Africa but we require robust evidence-based research so that resources are prioritised in interventions that are shown to be effective.

