










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.55 no.1 Cape Town Mar. 2017
ONCOLOGY
Breast Cancer and HIV: a South African perspective and a critical review of the literature
P ReddyI; S EbrahimI; B SinghI; S RamklassII; I BuccimazzaIII
IDepartment. of Surgery, Nelson R. Mandela School of Medicine. University of Kwa-Zulu Natal
IISchool of Clinical Medicine. University of Kwa-Zulu Natal
IIIDepartment of Specialized Surgery. Inkosi-Albert Luthuli Central Hospital
ABSTRACT
BACKGROUND: The diagnosis of breast cancer and concurrent HIV in South Africa is common. The limited current evidence on this subject suggests that the patients thus afflicted appear to be younger, have a more advanced stage of breast cancer, have a higher treatment related complications and poorer outcomes. This paper reviews the literature related to HIV and breast cancer, with a view to improving the standard and quality of care of HIV positive breast cancer patients.
METHODS: Pubmed, EBSCOhost, Google scholar and Science Direct electronic databases were searched from 2001 and 2015. using the terms ('HIV' OR 'human immunodeficiency virus' OR 'AIDS' OR 'Acquired Immunodeficiency Syndrome') and 'breast cancer' or 'breast carcinoma' to identify all publications related to HIV and breast cancer. Titles and abstracts were evaluated for eligibility and appropriate full text articles obtained. The data extraction variables included the type of study, year of publication, study setting, participants, sample size, outcome measures and main findings.
RESULTS: Only five studies fulfilled the criteria, in respect of the aforementioned maladies, with twenty or more participants in each study. Evidence suggested that breast cancers develop at a much younger age in the HIV positive patient compared to the HIV negative patients, with more aggressive appearing tumour biology. Overall, it appears that HIV positive patients experienced a higher cancer-specific mortality than HIV negative patients, and this is independent of the stage of the cancer or the cancer therapy received, further the relationship between the HIV syndrome and breast cancer is currently marginal and inconclusive, and hence requires further investigation.
CONCLUSION: The prescription and administration of chemotherapy is a challenge, with potential complications impacting on the morbidity and mortality in HIV positive patients. Currently there are no reliable predictors of those at risk to complications from chemotherapy; however, being on ART appears to provide an acceptable safety profile. HIV positive patients are best managed in the context of a multi-disciplinary team in order to achieve favourable outcomes in the treatment of cancer. Well-designed prospective trials to assess the response to multimodal therapy, and the long-term outcomes of HIV positive patients with breast cancer are needed.
Introduction
HIV and breast cancer are both diseases which have a major impact on the global burden of disease for women and require a united effort from all levels of health-care and government to try to constrain it. According to the latest National Cancer Registry (NCR) report (2010) published in 2015, in South Africa, breast cancer is the leading type of cancer affecting South African women.1 The determination of accurate cancer statistics remains a challenge in sub-Saharan Africa largely due to the lack of resources to establish and maintain national cancer registries. It is therefore likely that there is underreporting and underestimation of the burden of cancers in this region. There is a suggestion that HIV-positive patients have an elevated average lifetime risk of developing cancer, when compared with their HIV-negative counterparts.2-4 Statistics show that more than 25 million people in sub-Saharan Africa have HIV infection; however, not much is known about the cancer risk in this group.5
AIDS-defining cancers (ADC), namely Kaposi's sarcoma, cervical cancer, primary central nervous system (CNS) lymphoma, non-Hodgkin's lymphoma, and AIDS-associated cancers (AAC), such as anal cancer, lung cancer, liver cancer, and Hodgkin's lymphoma, have been commonly described since the recognition of the HIV pandemic. In HIV-positive individuals, cancer, regardless of type, is associated with an increased morbidity and mortality.69 A possible reason for the aggressive clinical course and poorer prognosis in HIV-positive individuals may be due to the suppressed immune system and impaired immune surveillance.710-12
The introduction of antiretroviral therapy (ART) has led to a decreased morbidity and mortality amongst HIV-positive individuals. In developed countries, the majority of HIV infected individuals have mild to moderate immunosuppression. This is due to the relative ease of access to ART.2,3,13-15 There has been a dramatic decline in the incidence of Kaposi's sarcoma (KS), but rates of some other non-AIDS defining cancers (NADC) including liver cancer, lung cancer and anal cancer have increased, as individuals infected with HIV live longer.2,4,10,12,15-19 Furthermore, due to the use of highly active ART (HAART), we can expect to manage more patients with cancer as their advancing age brings them into the natural age risk for cancer development.9,10
The diagnosis of breast cancer and concurrent HIV is certainly not infrequent, and it appears that these patients are younger with advanced stages of the disease.20 Some studies have suggested that HIV-positive patients with breast cancer have a higher incidence of treatment-related complications with poorer outcomes.21-23
This paper reviews the literature related to HIV and breast cancer, with a view to improving the standard and quality of care of HIV-positive breast cancer patients, based on the recommendations in the currently published literature.
Methods
Ethical approval was obtained from the Biomedical Research Ethics Committee (BREC) of the University of Kwa-Zulu Natal. (BE002/14)
Pubmed, EBSCOhost, Google scholar and Science Direct electronic databases were searched to identify all relevant publications related to HIV and breast cancer between 2001 and 2015. Search terms consisted of ('HIV' OR 'human immunodeficiency virus' OR 'AIDS' OR 'Acquired Immunodeficiency Syndrome') and 'breast cancer' or 'breast carcinoma' as keywords or text, in the title or abstract. Only human studies with 20 or more participants were considered for inclusion. All types of epidemiologic studies published in English were eligible for inclusion. The titles and abstracts were evaluated for eligibility and appropriate full text articles obtained. The data extraction variables included the type of study, year of publication, study setting, participants, sample size, outcome measures and main findings. A meta-analysis was unsuitable due to the heterogeneity of the research designs and study variables. The studies were evaluated through content analysis.
Results
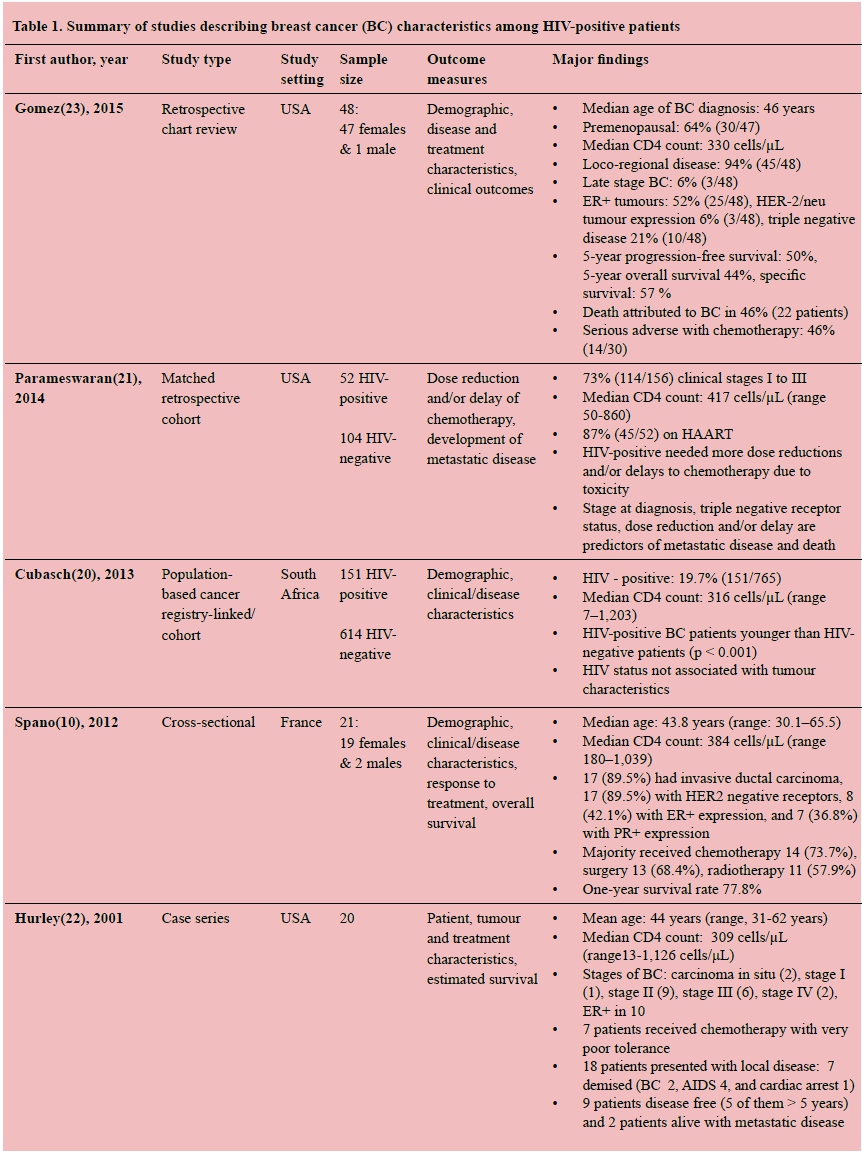
Summaries of included studies are shown in Table 1. Twenty-two publications were reviewed. Only five studies fulfilled the criteria, with twenty or more participants in each study. Seventeen studies were excluded due to small numbers included in the case series and cohort studies. There were no prospective studies looking specifically at the association between HIV and breast cancer. Most of the studies reviewed described characteristics of breast cancer and clinical outcomes among HIV-infected women with breast cancer.
Of the five papers included in the review, the largest series was published by Cubasch et al.20 This was a retrospective cohort study that compared HIV-positive black females with HIV-negative and HIV-naive (untested) black females. HIV-positive patients with breast cancer were statistically younger than HIV-negative patients (p < 0.001); however, there were no significant findings with regards to stage at presentation and tumour biology between the groups. Furthermore, CD4 cell count was not associated with the disease stage at the time of diagnosis or with the tumour biology. An important finding was that amongst the patients reported by Cubasch et al., HIV prevalence was similar to that of the source population (risk ratio [RR] 1.20, p = 0.13); thus the authors surmised that "HIV may not be related to breast cancer risk". However, evaluating HIV as a risk factor for breast cancer was not an objective of the study. An increase in adverse events in HIV-positive patients receiving chemotherapy, especially those with a low CD4 count, was noted.
The ONCOVIH study was a nationwide, multicentre cross-sectional study conducted across France and evaluated the number of new cancers diagnosed in HIV-infected patients.10,19 Six hundred and seventy-two malignancies were recorded in 668 patients; 21 patients were diagnosed with breast cancer. The findings of this study are summarised in Table 1. Hurley et al.22 conducted a retrospective chart review of 20 HIV-positive females with breast cancer at the University of Miami/Jackson Memorial Hospital. The results of this study are summarised in Table 1. This small series quantified patient and tumour characteristics and treatment outcomes among patients. The authors concluded that breast cancer in the HIV-infected patient follows a similar course to that seen in HIV-negative persons. A prospective cohort study would be necessary to establish if HIV seropositivity alters the clinical presentation, tumour biology and clinical outcome of breast cancer.
Similarly, the study by Gomez et al.23 was a retrospective audit of patients with HIV and breast cancer. The study described the clinical presentation, tolerance to therapy, therapy-related adverse events, and the clinical outcomes of patients. Forty-eight patient charts were reviewed. While most patients tolerated surgery, radiotherapy and endocrine therapy well, serious adverse events such as myelosuppression and neutropenic fever were reported in 14/30 (46%) of patients who received some form of chemotherapy.
Parameswaran et al.21 conducted a matched retrospective cohort study that included patients with all stages of breast cancer seen at their institution. A total of 52 HIV positive patients were diagnosed with breast cancer. A cohort of HIV-positive individuals with breast cancer was matched to HIV-negative controls. The outcomes evaluated were: chemotherapy dose reduction and/or delays, overall survival, and progression to metastatic disease. Authors concluded that HIV-positive females had more adverse events during breast cancer treatment, with more HIV-positive females requiring dose reductions and/or delays to chemotherapy (56% vs. 30%; p = 0.03) compared to their HIV negative counterparts. The reason for toxicity may be due to drug interactions between chemotherapy and ART.
No prospective work has been done comparing and analysing the clinic-pathological spectrum of breast cancer in HIV-positive and negative females, and those published works are mostly of small case series. The studies referred to present a heterogeneity of outcome measures, making it difficult to establish guidelines for the management of breast cancer in HIV-positive females. Most of the results are derived from studies of low power and hierarchy. The one common report pertains to the incidence of adverse events noted with patients receiving full-dose chemotherapy. Patients with HIV/AIDS and breast cancer will pose a major challenge for oncologists in trying to predict which patients will have severe complications and adverse events that may result in increased morbidity or mortality. Furthermore, the majority of the studies regarding HIV and breast cancer were published using data from Europe and the United States, which appear to have a different spectrum of disease to sub-Saharan Africa.
Discussion
HIV, together with breast cancer, poses a major burden on the health services and resources in South Africa, especially in the low socio-economic regions of the country.24 This is also a problem in the poorer sub-Saharan countries and in other developing countries worldwide.5,9,20,25-29
Breast cancer is a non-AIDS defining cancer (NADC). Breast cancer pathogenesis in HIV-positive patients, appears to be multifactorial, with the association between these two diseases remaining controversial. There is little known about the relationship, if any, between breast cancer and HIV. The general consensus is that there is no significant link between HIV and breast cancer.10,12,22,30-33
The study by Cubasch et al.20 suggests that HIV does not affect stage, grade, tumour sub-type, and survival of patients with breast cancer; however, this was not conclusive and further research into this group of patients was recommended. There is evidence which suggests that breast cancers occur earlier among HIV-positive patients compared to their HIV-negative counterparts, and with a more aggressive appearing tumour biology.6,20,32,34 On the other hand, some reports describe a protective role of HIV in breast cancer development, with either the virus or ART contributing to this potential protection.10,35,36 These interactions are not well understood. The publications reviewed were of small series and documented from low HIV prevalence regions. The interaction between HIV and the breast cancer lacks clear evidence of its association, and this requires further investigation.10,20,30,37
The therapies used in the treatment of breast cancer may be implicated in the interactions between these two diseases.
Studies have demonstrated beneficial effects of ART drugs in the treatment of breast cancer by inhibiting Breast Cancer Resistance Protein (BCRP) via protease inhibitors.38 There is also a suggestion that CCR5 antagonists may prevent metastasis of breast cancers. The HIV receptor CCR5, which is used as a portal of entry into the host cells, is also expressed in breast cancer cells, and this may contribute to local and systemic metastasis. The ART protease inhibitor Nelfinavir has been shown to have an effect on Her2/neu receptors and therefore may have an anti-tumorigenic effect.39
The effects of combined ART and oncological therapy for breast cancer, and their interactions with each other are not clearly documented. According to some authors, ART drugs may also potentially stimulate cancer growth.40 HIV-positive patients have a higher incidence of treatment related complications and subsequent delays. Both regimens on their own can be toxic and have detrimental effects on the patients being administered these drugs. Predicting the response to therapy is difficult and, due to the risks, therapy is often abandoned with the hope of treatment success and potential cure. Complications include hepatotoxicity, pancreatitis and bone marrow suppression. Neutropenia is another complication that leaves the patient prone to septicaemia, which is responsible for breaks or delays in treatment protocols that potentially render suboptimal therapy.10,21-23,41-43
The interpretation of the risk-benefit ratio when prescribing therapeutic chemotherapy protocols for breast cancer and concurrent HIV infection can be extremely challenging. It is suggested that concurrent ART and chemotherapy use is not associated with significant adverse events. Commencing HIV-positive patients with suppressed CD4 counts and those who have not been initiated on ART on chemotherapy may be associated with severe complications and with poorer clinical outcomes.22,23
Endocrine therapy is well tolerated by the patients with endocrine responsive (ER+/PR+) tumours. This appears to be a reasonable form of systemic therapy for patients, with endocrine responsive tumours, who are deemed unfit for chemotherapy or have had adverse events on the chemotherapy.21,23
Overall, it appears that HIV positive patients experienced a higher cancer-specific mortality than HIV-negative patients, and this is independent of the stage of the cancer or the cancer therapy received. The association between immunosuppression and tumour progression extent of the disease and the variety of therapies offered may explain this elevation in cancer-specific mortality among HIV-positive patients.44
Thus, breast cancer in HIV-positive females tends to present at a younger median age. The implication of this may warrant adjustments in the manner in which HIV-positive females are screened for breast cancer. The recommended protocols regarding screening for breast cancer may need to be commenced at an earlier age in the HIV-positive female. If we have to follow current population-based screening guidelines, in which screening is advised to commence at the age of 50, then we would find that most HIV-positive patients would have already presented with a clinically identified breast lesion. The appropriate imaging modality used to perform screening investigations in young patients is questionable. The sensitivity of mammography is decreased in younger patients due to their increased breast density, ultrasound is operator dependent, and Magnetic Resonance Imaging (MRI) of the breasts is probably the most sensitive, but comes at a substantial cost. Newer modalities such as automated whole breast ultrasound and contrast enhanced spectral mammography may be of value in these younger patients, but its use in screening has not been well established.
Most-certainly, in resource limited areas, there may be a place to educate patients and clinicians about being "breast-aware". Breast self-examination (BSE) and clinical breast examination (CBE) may need to be emphasised, and adequate technique in performing the examination needs to be taught to patients and clinicians alike. It is important for them to understand that even though benign breast diseases account for most "new lumps" under the younger female, one must have an index of suspicion for pathological disease in the HIV-positive female. Appropriate assessment of a new lump includes completion of the "triple assessment", which involves a thorough clinical examination, appropriate radiological investigation, and cytopathological confirmation of the finding. Early diagnosis and therapy should contribute to improved outcomes of breast cancer patients with HIV.
None of the publications include clear guidelines regarding the acceptable CD4 count required, the appropriate ART regimen, the timing of chemotherapy, the combined effects of chemotherapy and ART, etc., in newly diagnosed HIV-positive patients who have breast cancer. Prospective clinical trials are lacking and there is insufficient data to provide safe recommendations in HIV-positive females with breast cancer. It appears as though combined ART and chemotherapy is safely tolerated by most patients; however, dose adjustments, regimen changes and stop and re-initiation of ART protocols need to be considered in all HIV-positive patients with breast cancer.45 Currently, each case needs to be individualised regarding the appropriate combined therapy in the management of these complex patients.
The future of safe combined therapies in HIV positive patients with cancer may be in the combined use with immunotherapy.46 Exploration and research in the use of combined immunotherapy with chemotherapy, regarding improved tolerance of combined therapy and their potential outcome benefits, is exciting and we await the results of the current research being done.
There have been significant improvements in the efficacy and availability of ART in sub-Saharan Africa, with many HIV-positive patients now achieving improved survival, and HIV being reduced to a chronic type of illness. The added challenges of poverty, malnutrition and limited resources compromise the outcomes of HIV-positive patients with cancers, especially in sub-Saharan countries and other developing countries. In the future, with the aging of HIV-positive females, we are likely to see an increase in the development of NADCs such as breast cancer.
HIV testing should be mandatory in high HIV prevalence regions, so that ART may be commenced in newly diagnosed HIV positive patients, prior to surgical and oncological therapy, to improve their treatment-related morbidity, decrease their risk of treatment-related complications and improve their clinical outcomes.
Surgery, endocrine therapy, targeted therapy and radiation therapy appear to be well tolerated by HIV-positive patients with breast cancer. The prescription and administration of chemotherapy is a challenge, with potential complications impacting on the morbidity and mortality in HIV-positive patients. Currently there are no reliable predictors of those at risk to complications from chemotherapy; however, being on ART appears to provide an acceptable safety profile. The future may include the use of combined immunotherapy.
Conclusion
There is urgent need for prospective trials that address the issues of the optimal medical regimen for HIV management, the appropriate chemotherapy schedule and dosing regimen for the cancer, the safe combination of these therapies, the surgical therapies offered to HIV-positive patients, the appropriate management of complications and long-term follow-up to ensure the positive impact on reduced morbidity and overall survival. These studies will aid in the development of population-based guidelines for the management of breast cancer in the HIV-positive population.
For now, these decisions need to be individual-based, with the patient being part of the decision-making process. HIV-positive patients are best managed in the context of a multi-disciplinary team in order to achieve favourable outcomes in the treatment of cancer.
REFERENCES
1. National Cancer Registry (NCR) South Africa (2010). 2015. Available from: http://www.nioh.ac.za/?page=cancer_statistics&id=163 [ Links ]
2. Shiels MS, Pfeiffer RM, Gail MH, Hall HI, Jianmin L, Chaturvedi AK, et al. Cancer Burden in the HIV-infected Population in the United States. JNCI: J Natl Cancer Inst. 2011;103(9):753-62. [ Links ]
3. Layton JL, Castillo JJ. Non-AIDS Defining Cancers. Med Health R I. 2010;93(10):296-8. [ Links ]
4. Patel P, Hanson DL, Sullivan PS, Novak RM, Moorman AC, Tong TC, et al. Incidence of types of cancer among HIV- infected persons compared with the general population in the United States, 1992-2003. Ann Intern Med. 2008;148(10):728-36. [ Links ]
5. Mbulaiteye SM, Katabira ET, Wabinga H, Parkin DM, Virgo P, Ochai R, et al. Spectrum of cancers among HIV-infected persons in Africa: the Uganda AIDS-Cancer Registry Match Study. Int J Cancer. 2006;118(4):985-90. [ Links ]
6. Andrade AC, Luz PM, Veloso VG, Cardoso SW, Moreira RI, Grinsztejn B, et al. Breast cancer in a cohort of human immunodeficiency virus (HIV)-infected women from Rio de Janeiro, Brazil: a cases series report and an incidence rate estimate. Braz J Infect Dis. 2011;15(4):387-93. [ Links ]
7. Venkatesh KK, Saghayam S, Devaleenal B, Poongulali S, Flanigan TP, Mayer KH, et al. Spectrum of malignancies among HIVinfected patients in South India. Indian J Cancer. 2012;49(1):176-80. [ Links ]
8. Rabkin CS, Biggar RJ, Horm JW. Increasing incidence of cancers associated with the human immunodeficiency virus epidemic. Int J Cancer. 1991;47(5):692-6. [ Links ]
9. Biggar RJ, Chaturvedi AK, Bhatia K, Mbulaiteye SM. Cancer risk in persons with HIV/AIDS in India: a review and future directions for research. Infect Agent Cancer. 2009;4:1-8. [ Links ]
10. Spano J-P, Lanoy E, Mounier N, Katlama C, Costagliola D, Heard I. Breast cancer among HIV infected individuals from the ONCOVIH study, in France: Therapeutic implications. Eur J Cancer. 2012;48(18):3335-41. [ Links ]
11. Phelps RM, Smith DK, Heilig CM, Gardner LI, Carpenter CC, Klein RS, et al. Cancer incidence in women with or at risk for HIV. Int J Cancer . 2001;94(5):753-7. [ Links ]
12. Pantanowitz L, Dezube BJ. Evolving spectrum and incidence of non-AIDS-defining malignancies. Curr Opin HIV AIDS. 2009;4(1):27-34. [ Links ]
13. Goedert JJ, Schairer C, McNeel TS, Hessol NA, Rabkin CS, Engels EA. Risk of breast, ovary, and uterine corpus cancers among 85 268 women with AIDS. Br J Cancer. 2006;95(5):642-8. [ Links ]
14. Hogg RS, Heath KV, Yip B, Craib KJ, O'Shaughnessy MV, Schechter MT, et al. Improved survival among HIV-infected individuals following initiation of antiretroviral therapy. JAMA. 1998;279(6):450-4. [ Links ]
15. Engels EA, Pfeiffer RM, Goedert JJ, Virgo P, McNeel TS, Scoppa SM, et al. Trends in cancer risk among people with AIDS in the United States 1980-2002. AIDS (London, England). 2006;20(12):1645-54. [ Links ]
16. Tanon A, Jaquet A, Ekouevi DK, Akakpo J, Adoubi I, Diomande I, et al. The Spectrum of Cancers in West Africa: Associations with Human Immunodeficiency Virus. PloS One. 2012;7(10):1-8. [ Links ]
17. Calabresi A, Ferraresi A, Festa A, Scarcella C, Donato F, Vassallo F, et al. Incidence of AIDS-defining cancers and virus- related and non-virus-related non- AIDS-defining cancers among HIV-infected patients compared with the general population in a large health district of northern Italy, 1999-2009. HIV Med. 2013;14(8):481-90. [ Links ]
18. Engels EA, Biggar RJ, Hall HI, Cross H, Crutchfield A, Finch JL, et al. Cancer risk in people infected with human immunodeficiency virus in the United States. Int J Cancer. 2008;123(1):187-94. [ Links ]
19. Lanoy E, Spano J-P, Bonnet F, Guiguet M, Boué F, Cadranel J, et al. The spectrum of malignancies in HIV-infected patients in 2006 in France: the ONCOVIH study. Int J Cancer. 2011;129(2):467-75. [ Links ]
20. Cubasch H, Joffe M, Hanisch R, Schuz J, Neugut AI, Karstaedt A, et al. Breast cancer characteristics and HIV among 1,092 women in Soweto, South Africa. Breast Cancer Res Treat. 2013;140(1):177-86. [ Links ]
21. Parameswaran L, Taur Y, Shah MK, Traina TA, Seo SK. Tolerability of chemotherapy in HIV-infected women with breast cancer: are there prognostic implications? AIDS Patient Care STDS. 2014;28(7):358-64. [ Links ]
22. Hurley J, Franco S, Gomez-Fernandez C, Reis I, Velez P, Doliny P, et al. Breast Cancer and Human Immunodeficiency Virus: A Report of 20 Cases. Clin Breast Cancer. 2001;2(3):215-20. [ Links ]
23. Gomez A, Montero AJ, Hurley J. Clinical outcomes in breast cancer patients with HIV/AIDS: a retrospective study. Breast Cancer Res Treat. 2015;149(3):781-8. [ Links ]
24. Mayosi BM, Flisher AJ, Lalloo UG, Sitas F, Tollman SM, Bradshaw D. The burden of non-communicable diseases in South Africa. Lancet.374(9693):934-47. [ Links ]
25. Walker ARP. With recent changes in environmental factors among Africans in South Africa, how have cancer occurrences been affected? J R Soc Promot Health. 2002;122(3):148-55. [ Links ]
26. Somdyala NI, Bradshaw D, Gelderblom WC, Parkin DM. Cancer incidence in a rural population of South Africa, 1998-2002. Int J Cancer. 2010;127(10):2420-9. [ Links ]
27. Kiertiburanakul S, Likhitpongwit S, Ratanasiri S, Sungkanuparph S. Malignancies in HIV-infected Thai patients. Wiley-Blackwell; 2007. p. 322-3. [ Links ]
28. Swaminathan R, Lucas E, Sankaranarayanan R. Cancer survival in Africa, Asia, the Caribbean and Central America: database and attributes. IARC Sci Publ. 2011(162):23-31. [ Links ]
29. Bhikoo R, Srinivasa S, Tzu-Chieh Y, Moss D, Hill AG. Systematic Review of Breast Cancer Biology in Developing Countries (Part 1): Africa, the Middle East, Eastern Europe, Mexico, the Caribbean and South America. Cancers. 2011;3(2):2358-81. [ Links ]
30. Sarhan M, DePaz HA, Oluwole SFD. Breast Cancer in Women with Human Immunodeficiency Virus Infection: Pathological, Clinical, and Prognostic Implications. J Women's Health (15409996). 2010;19(12):2261-6. [ Links ]
31. Pantanowitz L, Sen S, Crisi GM, Makari-Judson G, Garb J, Skiest D. Spectrum of breast disease encountered in HIV- positive patients at a community teaching hospital. Breast. 2011;20(4):303-8. [ Links ]
32. 3Ruiz M, Davis H. Breast Cancer in HIV-Infected Patients: A Retrospective Single-Institution Study. J Int Assoc Physicians AIDS Care (Chicago, Ill: 2002). 2011;10(1):30-4. [ Links ]
33. Palan M, Shousha S, Krell J, Stebbing J. Breast Cancer in the Setting of HIV. Patholog Res Int. 2011;2011:925712-. [ Links ]
34. Calabresi A, Ferraresi A, Vavassori A, Castelli F, Quiros-Roldan E. Breast cancer among human immunodeficiency virus (HIV)- infected patients: the experience in Brescia, Northern Italy. Braz J Infec Dis. 2012;16(4):396-7. [ Links ]
35. Hessol NA, Napolitano LA, Smith D, Lie Y, Levine A, Young M, et al. HIV tropism and decreased risk of breast cancer. PloS One. 2010;5(12):e14349-e. [ Links ]
36. Stebbing J, Bower M. The anti-tumor effects of human immunodeficiency virus protease inhibitors: Ready for real time? Int J Cancer. 2011;128(1):1-2. [ Links ]
37. Hughes G, McKerr G, Allen J, Barnett Y. Are retroviruses involved in the aetiology of human breast cancer? Cancer Lett. 1996;103(2):219-25. [ Links ]
38. Gupta A, Zhang Y, Unadkat JD, Mao Q. HIV protease inhibitors are inhibitors but not substrates of the human breast cancer resistance protein (BCRP/ABCG2). The J Pharmacol Exp Ther. 2004;310(1):334-41. [ Links ]
39. Joong Sup S, Rao R, Beebe K, Neckers L, Hart I, Nahta R, et al. Selective Inhibition of HER2-Positive Breast Cancer Cells by the HIV Protease Inhibitor Nelfinavir. JNCI. 2012;104(20):1576-90. [ Links ]
40. Sikora MJ, Rae JM, Johnson MD, Desta Z. Efavirenz directly modulates the oestrogen receptor and induces breast cancer cell growth. HIV Med. 2010;11(9):603-7. [ Links ]
41. Klibanov OM, Clark-Vetri R. Oncologic Complications of Human Immunodeficiency Virus Infection: Changing Epidemiology, Treatments, and Special Considerations in the Era of Highly Active Antiretroviral Therapy. Pharmacotherapy. 2007;27(1):122-36. [ Links ]
42. García-Tejedor A, Devesa NR, Suárez-Pumariega P, del Barco S, Huerta MV. Breast cancer and HIV--the adverse effects chemotherapy. Breast J. 2007;13(6):622-3. [ Links ]
43. Mitsuyasu R. Oncological complications of human immunodeficiency virus disease and hematologic consequences of their treatment. Clin Infect Dis: An Official Publication Of The Infectious Diseases Society Of America. 1999;29(1):35-43. [ Links ]
44. Coghill AE, Shiels MS, Suneja G, Engels EA. Elevated Cancer- Specific Mortality Among HIV-Infected Patients in the United States. J Clin Oncol. 2015;33(21):2376-83. [ Links ]
45. Mayer KH, Torres HA, Mulanovich V. Management of HIV Infection in Patients With Cancer Receiving Chemotherapy. Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America. 2014;59(1):106-14. [ Links ]
46. Ding Z-C, Zhou G. Cytotoxic Chemotherapy and CD4+ Effector T Cells: An Emerging Alliance for Durable Antitumor Effects. Clin Dev Immunol. 2012;2012:12. [ Links ]
 Correspondence:
Correspondence:
Pramod Reddy
pramod6375@gmail.com


{kind=link}