










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Surgery
versión On-line ISSN 2078-5151
versión impresa ISSN 0038-2361
S. Afr. j. surg. vol.54 no.4 Cape Town nov. 2016
PLASTIC SURGERY
Management of acute complex traumatic wound with a dermal regeneration template: Case report
R R V Patel; M Giaquinto-Cillers; J Kotze; R S Hartnick; L W van der Merwe; E B Holford
Department: Plastic and Reconstructive Surgery & Burns, Kimberley Hospital Complex, Northern Cape Province
ABSTRACT
BACKGROUND: Acute complex traumatic wounds of the lower limbs are usually managed by a combination of multiple debridements, dressing changes, and specialized surgical procedures which may include tissue transfers for the reconstruction of the soft tissue injury. The recovery is lengthy, and the outcome dependent on the initial injury, the surgical procedures undertaken and rehabilitation programs with a multidisciplinary team.
METHODS: A nine-year-old male patient presented to Kimberly Hospital with an extensive soft tissue injury of the leg associated with a tibia fracture caused by a high velocity pedestrian vehicle accident.
RESULTS: A combination of proper wound care, "homemade" negative pressure wound therapy dressings, reduction of fracture and use of a dermal regeneration template over the fracture site, followed by skin grafting was used to manage the wound.
CONCLUSION: The final functional and cosmetic results obtained with the case suggest that the dermal regeneration template may provide a potential alternative for coverage of complex wounds, which might include an open fracture, without the need for complex tissue transfer interventions.
Key words: reconstruction of lower limbs, dermal regeneration template, complex acute wounds, leg trauma, traumatic wounds.
Introduction
Treatment of high-energy trauma of the lower limb with associated soft tissue and bone injuries remains a challenging entity for clinicians. The management of these complex injuries has evolved over the last decade and many limbs have been saved where in the past they would have been amputated. Extremity salvage is a lengthy process, and patients may have to undergo multiple procedures such as: vascular anastomosis, fixation of fractures, wound debridement and reconstruction of soft tissue defects immediately or at a later stage. Good functional outcome for this type of injury is the result of the combined effort of orthopaedic, vascular and plastic surgeons, together with a multidisciplinary team involving mainly wound care practitioners, physiotherapists, and occupational therapists.
While fractures can be usually addressed by standard techniques such as external fixation, intramedullary nailing, and/or internal plating, complex fractures may need bone grafting (vascularized or non-vascularized), Ilizarov bone lengthening, or artificial bone matrix.1
Soft tissue coverage of lower limb wounds may include one or the association of some available reconstructive techniques, depending on the location, depth and extent of the wound. In smaller wounds without bone exposure, healing by secondary intention may be considered; this requires multiple dressing changes and a variable period of time before closure is achieved. Wounds not healed within three to four weeks should be grafted, provided they have vascularized wound bed2 Split thickness skin grafts must not be used in wounds with exposed bone without periosteum, exposed tendon without paratenon, and exposed vessels or nerves.2
Flap selection for wound coverage of lower limb injuries is based on the location of the injury, availability of local tissues and donor-site morbidity. The leg should be divided topographically into thirds:2
1) for proximal third injuries, defects are often addressed using local muscle flaps associated with skin grafting; the flap most frequently used is the Gastrocnemius muscle;
2) For middle third defects the Soleus muscle is often used as a local flap;
3) Distal third defects are difficult to treat, and muscle flaps are often unreliable; although microvascular free flaps are mostly required in these patients, the Sural fasciocutaneous flap has proven to be an effective alternative.2
The main challenge using local flaps is the fact that they are usually involved in the zone of injury, may have associated crush injury and be damaged, thus they may not be available for local transfer. Microvascular free flaps have some disadvantages particularly in centres with limited resources, such as: need for specialized equipment and a trained team, lengthy theatre time and the need for good vascularity of blood vessels at the recipient site.3
The objective of this report is to present a case of a complex traumatic wound managed with a dermal replacement template (DRT) followed by skin grafting and vacuum-assisted dressing therapy.
Case Report
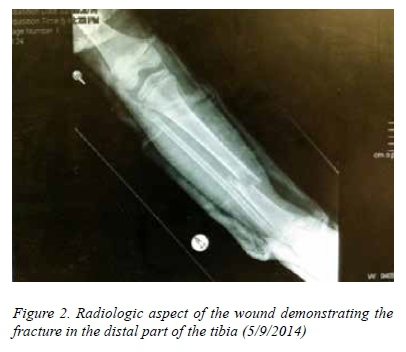
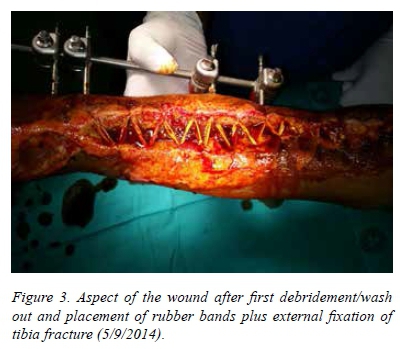
A nine-year-old boy was involved in a high velocity pedestrian vehicle accident (PVA) and was admitted to Kimberley Hospital Complex (KHC), a tertiary hospital situated in the Northern Cape Province (NCP), South Africa (SA). He sustained a degloving injury to the right lower extremity with extensive tissue loss measuring 25 x 15 cm with areas of exposed tibia (Figure 1), associated with an underlying distal tibia fracture (Figure 2). The child had no other concomitant injuries or other illnesses. He was admitted on 05/09/2014 and underwent surgery on the same day for washout and debridement of the wound, approximation of wound edges, using dermatotration and a "shoe lace" technique, with rubber band secured in place by surgical clips positioned closer to the wound edges4,5 and placement of external fixation (Figure 3). The wound was covered with silver-releasing dressing (Acticoat® -Smith and Nephew) and a "homemade" negative pressure wound therapy (NPWT) applied with wall suction.6,7,8 After four days from the initial surgical procedure, the child was taken to surgery for wound inspection, washout and further debridement of devitalized tissue. NPWT was used applying silver-releasing dressing (Acticoat®) to the wound bed.

On 12/09/2014, after assurance of a clean and viable wound bed, a dermal template (Integra® - Baroque Medical) manually meshed (with scalpel) was applied covering most of the wounds, including over two areas of exposed tibia, measuring around 3 x 1.5 cm. The dermal template was placed over the open distal tibia fracture. Split skin grafts (SSG) were applied onto the wounds distally to the dermal template, where granulation tissue was already developing, and silver-based dressings plus NPWT covered both grafts and DRT.
The dermal template and the distal grafts showed good uptake, and localised collections were drained with sterile needles during dressing changes in the ward, which took place every third day. The top silicone layer of the template was surgically removed on 7/10/2014 (day 21st post application), followed by immediate coverage with meshed SSG (1.5:1). Figure 4 depicts the aspect of the dermal matrix before removal of the top silicone layer. Silver-releasing dressings combined with NPWT were used in the following postoperative days. Dressings were changed in the ward every five days, reapplying the NPWT, until the inspection showed good uptake of skin grafts.

The child was discharged from the ward on 27/10/2015 for follow up dressings at a local clinic and follow up visits at the Kimberley Hospital Surgical and Orthopaedics Outpatient Clinics, and at the Physiotherapy Department. The final follow up visit was five months after the injury, when good functional and cosmetic result could be verified (Figure 5).

Discussion
Reconstruction of complex soft tissue defects secondary to trauma presents a surgical challenge. The standard reconstructive ladder is applied to these patients; however, every step of the ladder has its own sets of problems. To this particular wound, local fasciocutaneous flaps were not an option due to the size of the defect, and rotational muscle flaps or large fasciocutaneous flaps would lead to donor site morbidity and contour abnormality which would be difficult to be addressed. Although the use of free tissue transfers has revolutionized the approach to oncological and trauma surgery, microsurgical technique is time consuming even in the most experienced hands. A recipient vessel may be difficult to identify in a patient with trauma-related injury and previous surgical debridements.3 With those challenges in mind in our setting, a tertiary hospital with limited resources, we sought a new approach to the management of this complicated defect.
The "shoe-lace" technique used for this case (Figure 3) is popular amongst orthopaedic surgeons. It was initially created for the attempted primary closure of fasciotomy wounds. It is also sometimes referred to as dermatotraction and relies on the inherent laxity of skin and the fact that often with fasciotomy wounds, there is no tissue loss. While there are many specialised and costly devices to assist with dermatotraction, the basic principles can also be carried out with simple materials found in many hospitals, such as rubber bands, urinary catheters and skin staples. For fasciotomy wounds, the results of dermatotraction are thought to be superior to conventional methods of closure of fasciotomy wounds, such as split thickness skin grafts. The skin used for closure is sensate, often cosmetically more acceptable and does not result in donor site morbidity.4,5 As with the case in this report, this technique might not be able to primarily close a large wound, but it has proved of value in reducing the size of the defect, which assists in further management of the wound.
Integra® is a bi-layer system consisting of a dermal replacement matrix which has emerged as an adjunctive therapy to enhance healing of wounds. The dermal layer is an acellular matrix of bovine tendon collagen and glycosaminoglycan which serves as a template for the generation of a neodermis. The upper layer is a temporary epidermal substitute made of silicone.9 During neodermis formation, the top silicone layer avoids moisture loss from the wound and reduces shearing forces on the regenerating dermis; this layer is removed once the neodermis has fully developed. A thin epidermal autograft (SSG) is then applied over the neodermis. In clinical trials the dermal regeneration template has demonstrated excellent take and satisfactory aesthetics.10 Its efficacy has been proven in the closure of burn wounds, defects secondary to fasciitis, closure of chronic wounds, skin cancer excision sites, skin reconstruction (controlling keloid formation, correcting contractions) and degloving injuries.11,12,13,14
A few studies have demonstrated the successful grafting of a dermal regeneration template onto bone, supporting our decision for the use of this method.12,15,16,17,18 Engraftment onto bone is often clinically challenging due to the lack of vascularity and risk of infection.8 The DRT, unlike the skin, is acellular and therefore does not require immediate revascularization for successful incorporation into poorly vascularized tissues such as bare bone.13,15,16,17,18 Applied to acute wounds, Integra® controls inflammation and physiological reactions to injury, protects the wound and preserves tissue; it minimizes symptoms and nursing requirements, and fosters a rapid return to activity and rehabilitation.13 Creative use of this material has resulted in unexpected success with distal limb salvage allowing this technique to take its place along with adjacent tissue transfer, composite flaps and vascular pedicle flaps.9,13
While the literature on the use of DRT over exposed bone is rather extensive, there are relatively few reports of the use of DRT over open or healing fracture sites. One such example reports the successful use of a DRT over the open fractures and the exposed tendons of the foot; the DRT used in this reported case was PELNAC (Gunze Ltd., Kyoto, Japan), which is similar to Integra® in that it consists of a bilayer, with silicone as the top layer and a collagen matrix as the bottom layer, which provides the scaffold for the neodermis to regenerate.19 However the collagen layer of PELNAC is porcine based (derived from pig tendon) compared to the bovine-based collagen layer of Integra®. The case reported in this article serves as a further example of the successful use of a DRT over a healing fracture, demonstrating that regeneration of a neodermis over a fracture site is possible and will allow further successful skin grafting.
The integral role of NPWT in the management of complex wounds, such as the one presented in this case report, has been thoroughly described, with many known and perceived benefits. The mechanisms by which NPWT, using a foam interface, bring about these benefits are by creating
1) small micro-deformations on the wound surface,
2) macro-deformations,
3) removal of excess fluid and
4) optimisation of wound environment.20
The micro-deformations caused by NPWT stretch and draw out cells into the foam, thereby initiating intracellular pathways which promote cellular division and angiogenesis. However, the foam-wound interface is not present when a DRT is in place, as the silicone layer is in contact with the foam of the NPWT, therefore this mechanism might have a slightly diminished effect. Yet, some in vitro studies have shown that there is some increase in endothelial cell migration and mitosis into the DRT matrix; other in vivo studies have given conflicting evidence that NPWT does not accelerate neovascularisation.20,21,22
The macro-deformations involve the visible contraction of the wound edges as the negative pressure is applied to the dressing. Seromas, oedema and haematomas are often hindrances to optimal wound healing and skin graft survival; NPWT greatly reduces these obstacles by continually removing excess fluid from the wound bed and environment. This excess fluid often also contains toxins and bacteria which would otherwise have interfered with wound healing. Often when a DRT is placed, small cuts are purposefully made in the top silicone layer; this has a few functions, but will also assist in the removal of fluid if the wound is to receive NPWT. The wound environment is optimised by enhanced thermoregulation, provided by the foam and semi-occlusive dressing and by modulation of the inflammatory process at the wound bed. This is achieved through constant removal of inflammatory mediators and leukocytes.20
The common reasons for skin graft failure are:
1) poor wound bed preparation,
2) haematomas and seromas,
3) infections and
4) movement at the wound bed.
There is good evidence for the use of NPWT both before and after a complex wound is definitely closed as it greatly reduced the burden of these factors. NPWT has an important and beneficial role in preparing a wound for either the placement of a DRT or a skin graft. The use of NPWT also has many advantages after the wound has been addressed with a DRT or skin graft.23,24
Apart from the benefits of NPWT at the wound bed, NPWT has the additional, and welcomed benefits of splinting the wound and reducing mechanical shearing forces. As negative pressure is applied to the dressing, the foam becomes rather firm and inflexible, which slightly decreases mobility in the area. The negative pressure also allows for the rigid DRT to better conform to defects, especially those that are concave and circumferential.25 These factors play an important role in the integration of the dermal template and the survival of subsequent skin grafts.24
It has also been demonstrated that wounds managed with the combination of NPWT and DRT have resulted in greater elasticity of scars and a closer to natural skin pigment on the grafted sites.23,24,26
Often a barrier to NPWT, especially in resource limited settings, is the high cost of formal NPWT systems. For this case we used a "homemade" NPWT system, which consisted of a sterile foam, which was cut to conform to the shape of the defect, tubing, which was often a large bore feeding tube, with multiple holes in the tip or simple suction tubing, and an adhesive plastic dressing which covered the tubing and foam, as well as adhering past the borders of the wound to create an airtight seal. The tubing was then connected to a wall suction and subatmospheric pressures were applied to the wound. These homemade systems proved to be an efficient and cost-effective alternative to formal NPWT devices and systems.6,7,8
The ideal treatment for a particular patient should be tailored around the patient's needs. In complex wounds, the goal should include coverage and protection of exposed tendons and bones, filling in deep soft tissue defects and preservation of function.14 To reach this goal, a range of adjunctive treatment modalities have been available including cultured epidermal autografts, myocutaneous flaps and neuromuscular pedicle muscle flaps. These modalities have shown varied degrees of success. Because of those results, the use of synthetic "scaffolds" allows for native tissue regeneration and continues to be an attractive alternative.14 Despite the necessity for a two stage procedure, matrix templates offer many advantages, inclusive immediate availability, ability to cover large defects, minimal donor site morbidity, good cosmetic results with optimal contouring, and reduced scarring and hypertrophy.13
Although the hospital stay of the patient (52 days in total) in this report may not be used to draw conclusions about the associated costs or to compare with the estimated average of stay for more complex procedures and their complications, it showed to be adequate if we consider our limited resources in terms of equipment, staff and theatre availability.
Conclusion
On the basis of this clinical case, the use of dermal matrix (DRT) for the treatment of complex traumatic wound resulted in good cosmetic and functional results and less donor-site morbidity. Thus, DRT is a viable alternative and should be considered in patients with large complex traumatic wounds of the lower limbs in settings with limited resources.
REFERENCES
1. Cross WW, Swiontkowski MF. Treatment principles in the management of open fractures. Indian J Orthop. 2008;42(4):377-386. [ Links ]
2. Reddy V, Stevenson TR. Lower extremity reconstruction. Plast Reconstr Surg. 2008;121(4S):1-7 [ Links ]
3. Kang MJ, Chung CH, Chang YJ, et al. Reconstruction of the lower extremity using free flaps. Arch Plast Surg. 2103;40(5):575-583. [ Links ]
4. Sandiford N, Hotouras A, Rao S. The Dermatotraction Technique For Closure Of Fasciotomy Wounds. The Internet Journal of Orthopedic Surgery. 2006;5(2). [ Links ]
5. Eid A, Elsoufy M. Clinical Study: Shoelace Wound Closure for the Management of Fracture-Related Fasciotomy Wounds. International Scholarly Research Network. ISRN Orthopedics. Volume 2012, Article ID 528382 [ Links ]
6. Gill NA, Hameed A, Sajjad Y, Ahmad Z, Mirza MA. "Homemade" Negative Pressure Wound Therapy. Treatment of Complex Wounds Under Challenging Conditions. Wounds. 2011;22(4):84-92. [ Links ]
7. Rozen WM, Shahbaz S, Morsi A. An improved alternative to vacuum-assisted closure (VAC) as a negative pressure dressing in lower limb split skin grafting: a clinical trial. J Plast Reconstr Aesthet Surg. 2008;61(3):334-7. [ Links ]
8. Shalom A, Eran H, Westreich M, Friedman T. Our experience with a "homemade" vacuum-assisted closure system. Isr Med Assoc J. 2008 Aug-Sep;10(8-9):613-6. [ Links ]
9. Halim AS, Khoo TL, Mohd SJ. Biologic and synthetic skin substitutes: An overview. Indian J Plastic Surg, 2010;43:23-28. [ Links ]
10. Simon S, Hammoudeh J, Low C, et al. Complex wound management with an Artificial Dermal Regeneration Template. Available at www.woundresearch.com [assessed 12 February 2015]. [ Links ]
11. Gottleib ME, Furman J. Successful management and surgical closure of chronic and pathological wounds using Integra. J Burns & Surgery Wound Care. 2004;3:54-60. [ Links ]
12. Jeng CJ, Fidler PE, Sokolich JC. Seven years' experience with Integra as a reconstructive tool. Paper presented at the 38th Annual Meeting of American Burn Association, 2006 April 4-7, Las Vegas: Nevada. [ Links ]
13. Steward JE. Next generation products for wound management. Available at www.worldwidewounds.com [assessed 12 February 2015]. [ Links ]
14. Tufaro AP, Buck DW, Fischer AC. The use of artificial dermis in the reconstruction of oncologic surgical defects. Plast Reconstr Surg. 2007;120:638-646. [ Links ]
15. Herlin C, Louhaem D, Bigorre M, Dimeglio A, Captier G. Use of Integra in a Paediatric Upper Extremity Degloving Injury. Journal of Hand Surgery. European Volume, 2007;32E(2):179-184 [ Links ]
16. Morozzo U, Villafane JH, Ieropoli G, et al. Soft Tissue Reconstructions with Dermal Substitutes Versus Alternative Approaches in Patients with Traumatic Complex Wounds. Indian J Surg. December 2015;77(Suppl 3):S1180-S1186 [ Links ]
17. Nguyen DQ, Potokar TS, Price P. An objective long-term evaluation of Integra (a dermal skin substitute) and split thickness skin grafts, in acute burns and reconstructive surgery. Burns. 36(2010);23-28 [ Links ]
18. Muangman P, Engrav LH, Heimbach DM, et al. Complex Wound Management Utilizing an Artificial Dermal Matrix. Ann Plast Surg. 2006;57:199-202 [ Links ]
19. Zhao JC, Yu JA, Shi K, Jin ZH, Niu ZH. Treatment of an Open Fracture Wound with Skin Graft Dressings (PELNAC): A Case Report. Wounds. 2011;23(8):E21-E26. [ Links ]
20. Huang C, et al. Effect of Negative Pressure Wound Therapy on Wound Healing. Current Problems in Surgery. 2014;51:301-331 [ Links ]
21. González Alana I, Torrero López JV, Martín Playá P, Gabilondo Zubizarreta FJ Combined Use of Negative Pressure Wound Therapy and Integra® To Treat Complex Defects in Lower Extremities after Burns. Annals of Burns and Fire Disasters. 2013 June; Vol. XXVI(2) [ Links ]
22. Moiemen, NS, Yarrow J, Kamel D, Kearns D, Mendonca D. Topical negative pressure therapy: Does it accelerate neovascularisation within the dermal regeneration template, Integra? A prospective histological in vivo study. Burns. 2010;36:764-768 [ Links ]
23. Bloemen MC, van der Wal MB, Verhaegen PD, et al. Clinical effectiveness of dermal substitution in burns by topical negative pressure: a multi-center randomized controlled trial. Wound Repair Regen. 2012;20(6):797-805. [ Links ]
24. Dini M, Quercioli F, Mori A, Romano GF, Lee AQ, Agostini T. Vacuum-assisted closure, dermal regeneration template and degloved cryopreserved skin as useful tools in subtotal degloving of the lower limb. Injury, Int. J. Care Injured. 2012;43:957-959 [ Links ]
25. Stiefel D, Schiestl CM, Meuli M. The positive effect of negative pressure: vacuum-assisted fixation of Integra artificial skin for reconstructive surgery. Journal of Pediatric Surgery. 2009;44:575-580 [ Links ]
26. Nguyen DQ, Potokar TS, Price P. An objective long-term evaluation of Integra (a dermal skin substitute) and split thickness skin grafts, in acute burns and reconstructive surgery. Burns. 2010;36:23-28 [ Links ]
27. Ozturk CN, Opara P, Ozturk C, Djohan R. Treatment of Foot Degloving Injury With Aid of Negative Pressure Wound Therapy and Dermal Regeneration Template. The Journal of Foot & Ankle Surgery. 2015;54:1132-1135 [ Links ]
28. Morozzo U, Villafane JH, Ieropoli G, Zompi SC, Cleland JA, Navissano M, Malan F. Soft Tissue Reconstructions with Dermal Substitutes Versus Alternative Approaches in Patients with Traumatic Complex Wounds. Indian J Surg. December 2015;77(Suppl 3):S1180-S1186 [ Links ]
29. Gabriel A, Thimmappa B, Rubano C, Storm-Dickerson T. Evaluation of an ultra-lightweight, single-patient-use negative pressure wound therapy system over dermal regeneration template and skin grafts. International Wound Journal. 2012 [ Links ]
30. Milcheski DA, Chang AA, Lobato RC, et al. Coverage of Deep Cutaneous Wounds Using Dermal Template in Combination with Negative-pressure Therapy and Subsequent Skin Graft. Plast Reconstr Surg Glob Open. 2014;2:e170. [ Links ]
 Correspondence:
Correspondence:
Ravin R Patel
ravin.patel.3@gmail.com

