










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.54 no.4 Cape Town Nov. 2016
ORIGINAL ARTICLE
Comparative study of extralevator vs. conventional abdominoperineal excision in a single centre in the developing world
M OostenbroekI; E CoetzeeII; A BoutallII; R BaigrieIII; P GoldbergIII
IStudent at the Amsterdam University, Amsterdam Medical Centre, Amsterdam, The Netherlands
IIConsultant Colorectal Surgeon, University of Cape Town, Groote Schuur Hospital, South Africa
IIIAssociate Professor, Department of Colorectal Surgery, University of Cape Town, Groote Schuur Hospital, South Africa
ABSTRACT
ABSTRACT: Abdominoperineal excision (APE) is used to resect cancers in the distal rectum and anus where sphincter-preserving surgery is not possible. It is associated with increased local recurrence rates compared to anterior resection. The extralevator abdominoperineal excision (ELAPE) was developed to reduce local recurrence and was widely adopted without sound evidence.
AIM: To compare the short-term (2 years) outcomes of patients managed with ELAPE to those with conventional APE in a single institution in a developing country.
METHODS: A prospective database on all patients treated with prone ELAPE from 2010 to 2014 was compared to patients treated with conventional APE. Patient demographics, tumour characteristics, intra-operative tumour perforation, involvement of the circumferential resection margin (CRM), surgical complications and mortality are reported.
RESULTS: Fifty-six patients were treated with APE of which 29 were male. Median age was 56. Thirty underwent conventional APE (16 male; 14 female) and 26 underwent ELAPE (15 male; 11 female). The groups were similar in age, tumour histology, height above anal verge clinical staging and response to neoadjuvant treatment. Perineal closure techniques in both cohorts were similar. There was no difference in intra-operative tumour perforation, involvement of the CRM, perineal wound complications or 30-day mortality in the 2 groups.
CONCLUSION: There is no difference in the important short-term outcomes of conventional APE when compared to ELAPE.
Introduction
Abdominoperineal excision (APE) is a surgical treatment used to treat cancer of the lower third of the rectum or anus where sphincter-preserving surgery (anterior resection (AR) with anastomosis) is not possible. Patients undergoing APE for low rectal adenocarcinoma have an higher local recurrence rate and overall worse prognosis than patients undergoing AR.1,2 This may be explained by the anatomy of the distal rectum, which is covered by less mesorectum, resulting in earlier tumour invasion of surrounding structures compared to the more proximal rectum.3
In an effort to improve the prognosis for patients with distal rectal cancer the extralevator APE (ELAPE) was introduced in 2006.4 This surgical procedure aimed to excise a more extensive cylindrical specimen, which may reduce tumour involvement of the circumferential resection margin (CRM) and intraoperative tumour perforation.
It is still not clear whether oncological outcomes of the ELAPE are superior to conventional APE. Some authors have shown better outcomes using ELAPE,5-7 and others have not.8,9 One randomized controlled trial showed a reduction in local recurrence with ELAPE.10 Two systematic reviews reached different conclusions.11,12
A developing country is a nation with a lower living standard, underdeveloped industrial base, and low human development index relative to other countries. The United Nations and the World Bank have defined a developing country as a country with less than US$11905 per capita gross national income in 2015.17 Typically in this environment, patients present late in their disease course and this manifest in rectal cancer by a very high incidence of patients with locally advanced disease at presentation. One can postulate that less favourable surgical results with an increased involvement of CRM will be found in such a population.
One of the reported concerns with an extended resection is the potential for increased perineal wound complications. ELAPE was associated with an increase in wound complications in one series.5 Another series showed no difference in overall wound complications, but demonstrated a higher incidence of perineal wound infections.13 Reported perineal closure techniques vary between biological mesh implants, myocutaneous flaps or direct closure.5,9,15
In a recent study, the authors proposed that ELAPE should be used only in selected cases as a decrease in intra-operative tumour perforation was shown only in patients with T0-T2 tumours within 4 cm of the anal verge.13
The aim of this study is to assess the short-term outcome of ELAPE versus standard APE in a single academic centre in a developing country.
Patients and methods
A prospective database of patients treated with prone ELAPE from 2010 to 2014 was compared to those patients treated with conventional APE. Data was prospectively collected on a data sheet and captured on a spread sheet (Microsoft Excel). One senior surgeon performs ELAPE and the other conventional APE. The choice of procedure thus depended on the senior surgeon performing or supervising the surgery. Patient allocation to either surgeon was determined by operating list availability. The limited access to operating time in this cost-constrained environment meant that patients were allocated to whichever surgeon's list could accommodate the operation, thus minimising the risk of selection bias.
Patients requiring surgery for low rectal cancer, or cancer of the anal canal, were included in this study. All patients treated for rectal adenocarcinoma and a single patient with rectal melanoma had a pre-treatment magnetic resonance imaging (MRI) of the pelvis. All patients had distant staging with computerized tomography (CT) of the abdomen and chest X-ray (CXR). Where suspicious lesions on CXR were identified, a CT scan of the chest was requested. All patients were managed through a multi-disciplinary team (MDT), with no selection criteria applied for allocation to either surgeon. All but one of the patients operated for squamous cancer of the anal canal had salvage surgery for treatment failure after chemoradiation.
The technique of prone ELAPE has previously been described4 and was adopted in our unit in 2010. The abdominal procedure is performed in the Lloyd-Davies position, and the dissection follows total mesorectal excision (TME) principles, down to the sacrococcygeal junction posteriorly and to the level of the upper part of the prostate anteriorly in males, or the first few centimetres of the vagina anteriorly in females. An omentoplasty is routinely performed. A suction drain, together with the omentum is sutured to the divided rectum, thereby facilitating correct placement after delivery of the resected specimen through the perineal wound. The abdominal incision is closed and the stoma created. Thereafter the patient is positioned in the prone jack-knife position and the perineal excision performed, after closing the anus with a purse string suture.
Perineal closure method was performed as per surgeon choice and was obtained by primary closure in the majority of patients by closing the ischiorectal, subcutaneous fat and skin in layers. Closure with myocutaneous flaps (gluteus maximus or vertical rectus abdominus (VRAM) flaps) was used where direct closure was not possible due to extensive resection of the ischiorectal space necessitated by large tumour size. Coccyx segments were resected in the initial cases, but routine resection of the coccyx was abandoned after the first 5 cases. Thereafter, resection of segments of the coccyx was only preformed when required to obtain an oncological sound resection or delivery of a bulky specimen.
Conventional APE was performed as a two-team procedure in the lithotomy-Trendelenburg position14 following the principles of total mesorectal excision. Both teams operated with the intention of obtaining a cylindrical specimen.
An involved circumferential resection margin was defined as tumour extending within 1 mm of the resection margin. Pathology samples were assessed by a consultant pathologist and reviewed by a team of pathologists when needed. After discharge from hospital, patients were routinely reviewed in a combined multi-disciplinary colorectal outpatient clinic and never discharged from this clinic. Statistical significance was calculated using the Fischer's Exact test and p=0.05 accepted as significant. The Human Research Ethics Committee of the University of Cape Town, South Africa, approved the study.
Results
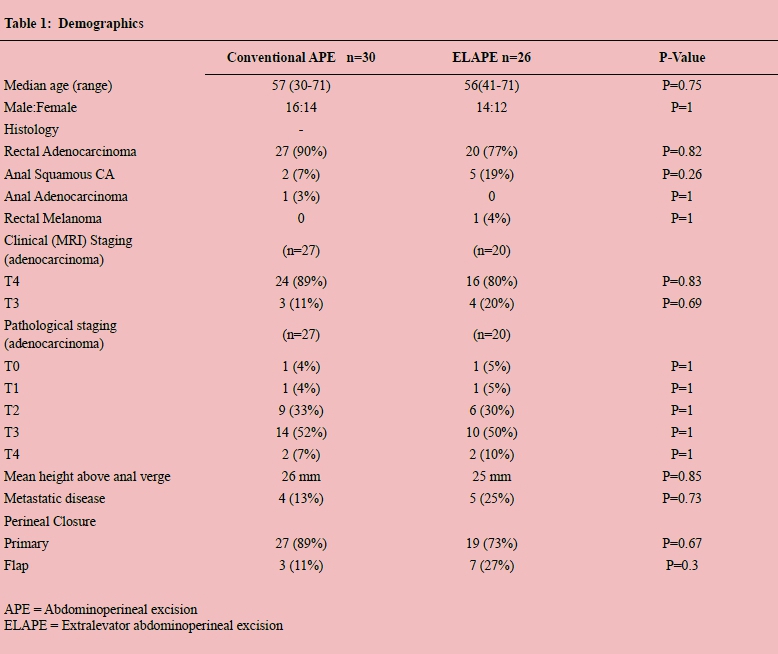
Fifty-six patients were treated with APE during the study period of which 29 were male. Median age was 56. Thirty underwent conventional APE (16 male; 14 Female) and 26 underwent ELAPE (15 male; 11 Female). The demographic data, histology and staging are summarised in Table 1. The median follow-up period was 25 months (range 2 to 55).
The pretreatment histological features and radiological T-staging were similar in the two groups (Table 1). One patient with an anal canal adenocarcinoma underwent conventional APE, and one patient with anal canal melanoma underwent ELAPE. With one exception, all patients with adenocarcinoma received long-course neoadjuvant chemoradiation. Patients with anal squamous carcinoma underwent salvage APE for persistent or recurrent disease after chemoradiation, except one who had a primary resection (conventional APE). The patient with melanoma of the rectum did not receive chemoradiation.
The presence of preoperative metastatic disease was similar in both cohorts. Primary perineal closure was achieved in 27 (89%) of patients who underwent conventional APE and 19 (73%) of those treated with ELAPE (p=0.67). Ten patients required myocutaneous flaps to achieve perineal closure (7= ELAPE, 3=Conventional APE, p=0.3). VRAM flaps were used in five patients in the ELAPE group and three patients in the conventional APE group. Gluteus advancement flaps were used in two patients treated with ELAPE.
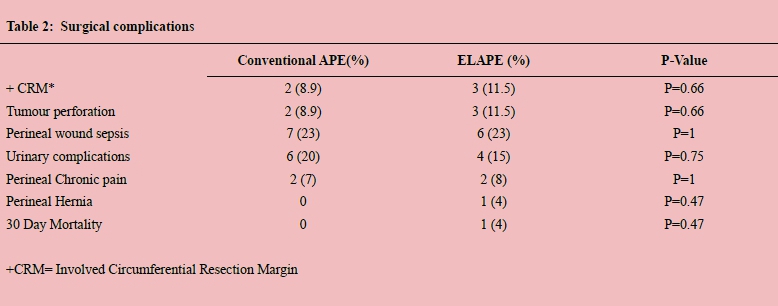
Surgical complications are reported in Table 2. Circumferential resection margin (CRM) involvement and tumour perforations were comparable in the two groups with 2 (8.9%) in the conventional APE cohort and 3 (11%) in the ELAPE cohort (p=0.66). There was no difference in the rates of perineal wound sepsis, urinary complications or perineal pain. One patient in the ELAPE cohort developed a perineal hernia and one patient died unexpectedly in the early postoperative period, from a cardiovascular event.
Discussion
Since the description by Holm et al 4 of the prone ELAPE, there has been widespread adoption of this technique without clear evidence of its benefits over the conventional approach.
By extending the perineal margin of resection, the aim is to improve local control, while accepting a presumed increase in the risk of perineal wound complications and perineal hernia.5 In the initial description by Holm, gluteus maximus myocutaneous flaps were used to reconstruct the perineal wound. Others have used biological mesh to obtain closure.5,9 Primary closure of the defect where possible has been advocated by others.15 There was only one perineal hernia in the ELAPE group during the follow-up period. This patient had primary closure of the perineal wound without mesh or flap closure. Our preference is not to routinely use mesh or myocutaneous flaps when primary closure is possible.
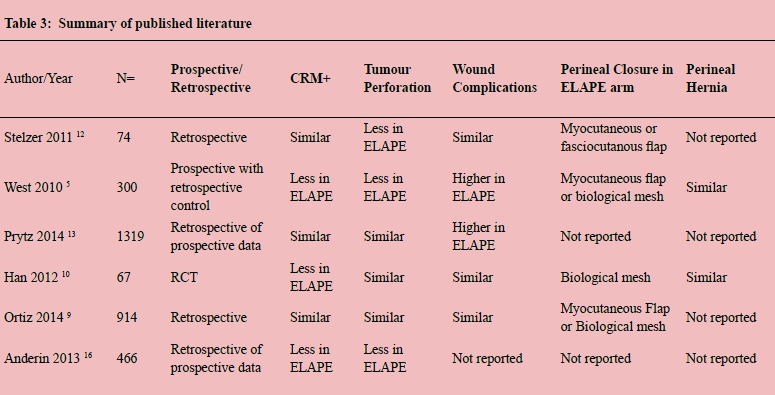
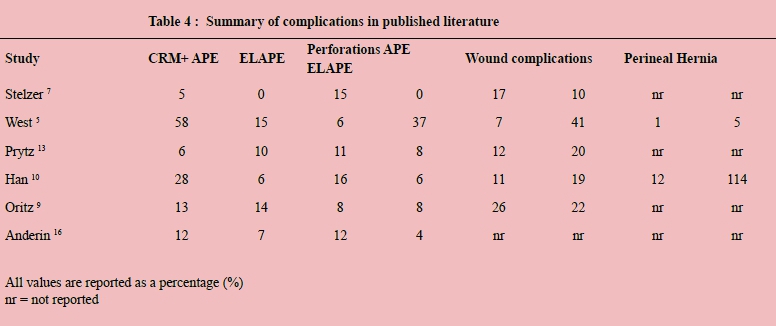
There are only six comparative series published, with a disparity of findings. Some demonstrated similar outcomes, and others showed improved local resection outcomes for ELAPE, with decreased intraoperative tumour perforation and decreased rates of involved circumferential resection margins (Table 3). The only randomized controlled trial showed a decreased rate of positive CRM in the ELAPE cohort, but similar intraoperative tumour perforations, perineal wound complications and perineal hernia rates for ELAPE and conventional APE.10
This study demonstrates no difference in the rates of positive CRM, intraoperative tumour perforations, perineal wound septic complications, perineal pain or perineal hernia. This outcome was similar to those published in two studies reported in Table 3. Only two studies reported perineal hernia rates. In both these studies, the rate of perineal herniation was similar in both cohorts. Even though over 75% of patients in this study had primary closure of the perineal defect, only one patient in the ELAPE group developed a perineal hernia at 17 months.
In this series, the mean tumour height from the anal verge in the conventional APE and ELAPE patients was similar. More than 80% of adenocarcinomas in both cohorts in this study were staged as T4 on pretreatment imaging and as ypT3 after resection, following neoadjuvant chemoradiation. This is a testimony of the locally advanced nature of pathology treated in a developing world environment, which provides a particular technical challenge when compared to comparative staging in the developed world. The rate of involved CRM and intraoperative tumour perforation was comparable to that in the published literature. By aiming to achieve a cylindrical specimen in both the lithotomy-Trendelenburg and prone positions, acceptable surgical results were achieved.
The prone position offers better exposure and an easier operating field to the surgeon, assistants and trainees. This has ensured its unanimously preferred status in our unit amongst trainees who, because of the simultaneous accrual to both cohorts, have had the benefit of experiencing both techniques in their training.
This study has several strengths and limitations. It is not a randomised trial, but the two cohorts were selected without bias, and recruited simultaneously. Both surgeons were highly experienced, with each having over 20 years' experience. The relatively small sample size is a limitation, but this is of considerably less importance when only short-term outcomes are being assessed, rather than long-term oncological outcomes. There were no obvious trends to suggest that larger cohorts would have resulted in different conclusions. There was homogeneity in the groups with no difference in demographic or oncological characteristics. This series is the first to be reported from a centre in the developing world and reports on APE in a cohort presenting with a locally advanced stage. It demonstrates the feasibility and acceptance of prone ELAPE in this environment.
Conclusion
This study demonstrated no difference in the important short-term outcomes of conventional APE when compared to ELAPE in two synchronous and comparable cohorts of patients presenting with advanced local disease in the developing world. Surgeon preference remains the primary determinant of choice of technique.
REFERENCES
1. Nagtegaal ID, van de Velde CJ, Marijnen CA, van Krieken JH, Quirke P, Dutch Colorectal Cancer Group, et al. Low rectal cancer: a call for a change of approach in abdominoperineal resection. J Clin Oncol. 2005 Dec 20;23(36):9257-9264. DOI:10.1200/JCO.2005.02.9231 [ Links ]
2. How P, Shihab O, Tekkis P, Brown G, Quirke P, Heald R, et al. A systematic review of cancer related patient outcomes after anterior resection and abdominoperineal excision for rectal cancer in the total mesorectal excision era. Surg Oncol. 2011 Dec;20(4):e149-55. DOI: 10.1016/j.suronc.2011.05.001. [ Links ]
3. Marr R, Birbeck K, Garvican J, Macklin CP, Tiffin NJ, Parsons WJ, et al. The modern abdominoperineal excision: the next challenge after total mesorectal excision. Ann Surg. 2005 Jul;242(1):74-82. DOI: 10.1097/01.sla.0000167926.60908.15 [ Links ]
4. Holm T, Ljung A, Haggmark T, Jurell G, Lagergren J. Extended abdominoperineal resection with gluteus maximus flap reconstruction of the pelvic floor for rectal cancer. Br J Surg. 2007 Feb;94(2):232-238. DOI: 10.1002/bjs.5489 [ Links ]
5. West NP, Anderin C, Smith KJ, Holm T, Quirke P, European Extralevator Abdominoperineal Excision Study Group. Multicentre experience with extralevator abdominoperineal excision for low rectal cancer. Br J Surg. 2010 Apr;97(4):588-599. DOI: 10.1002/bjs.6916 [ Links ]
6. Anderin C, Martling A, Lagergren J, Ljung A, Holm T. Short-term outcome after gluteus maximus myocutaneous flap reconstruction of the pelvic floor following extra-levator abdominoperineal excision of the rectum. Colorectal Dis. 2012 Sep;14(9):1060-1064. DOI: 10.1111/j.1463-1318.2011.02848.x [ Links ]
7. Stelzner S, Hellmich G, Schubert C, Puffer E, Haroske G, Witzigmann H. Short-term outcome of extra-levator abdominoperineal excision for rectal cancer. Int J Colorectal Dis. 2011 Jul;26(7):919-925. DOI: 10.1007/s00384-011-1157-0 [ Links ]
8. Asplund D, Haglind E, Angenete E. Outcome of extralevator abdominoperineal excision compared with standard surgery: results from a single centre. Colorectal Dis. 2012 Oct;14(10):1191-1196. DOI: 10.1111/j.1463-1318.2012.02930.x. [ Links ]
9. Ortiz H, Ciga MA, Armendariz P, Kreisler E, Codina-Cazador A, Gomez-Barbadillo J, et al. Multicentre propensity score-matched analysis of conventional versus extended abdominoperineal excision for low rectal cancer. Br J Surg. 2014 Jun;101(7):874-882. DOI: 10.1002/bjs.9522. [ Links ]
10. Han JG, Wang Z, Wei GH, Gao ZG, Yang Y, Zhao BC. Randomized clinical trial of conventional versus cylindrical abdominoperineal resection for locally advanced lower rectal cancer. Am J Surg. 2012(204):274. DOI: 10.1016/j.amjsurg.2012.05.001. [ Links ]
11. Krishna A, Rickard MJ, Keshava A, Dent OF, Chapuis PH. A comparison of published rates of resection margin involvement and intra-operative perforation between standard and 'cylindrical' abdominoperineal excision for low rectal cancer. Colorectal Dis. 2013 Jan;15(1):57-65. DOI: 10.1111/j.1463-1318.2012.03167.x. [ Links ]
12. Stelzner S, Koehler C, Stelzer J, Sims A, Witzigmann H. Extended abdominoperineal excision vs. standard abdominoperineal excision in rectal cancer-- a systematic overview. Int J Colorectal Dis. 2011 Oct;26(10):1227-1240. DOI: 10.1007/s00384-011-1235-3 [ Links ]
13. Prytz M, Angenete E, Ekelund J, Haglind E. Extralevator abdominoperineal excision (ELAPE) for rectal cancer--short-term results from the Swedish Colorectal Cancer Registry. Selective use of ELAPE warranted. Int J Colorectal Dis. 2014 Aug;29(8):981-987. DOI: 10.1007/s00384-014-1932-9. [ Links ]
14. Schmidt RL, Nelson PA, Martin GB, Boghossian HM. Synchronous (two-team) abdominoperineal resection of the rectum. AMA Arch Surg. 1958 Oct;77(4):492-497. DOI: 10.1001/archsurg.1958.04370010024003. [ Links ]
15. Palmer G, Anderin C, Martling A, Holm T. Local control and survival after extralevator abdominoperineal excision for locally advanced or low rectal cancer. Colorectal Dis. 2014 Jul;16(7):527-532. DOI: 10.1111/codi.12610. [ Links ]
16. Anderin C, Granath F, Martling A, Holm T. Local recurrence after prone vs supine abdominoperineal excision for low rectal cancer. Colorectal Dis. 2013 Jul;15(7):812-815. DOI: 10.1111/codi.12148 [ Links ]
17. United Nations Department of Economic and Social Affairs 2015. What is a Developing Nation? Available from: http://unstats.un.org. Accessed 27 May 2016. [ Links ]
 Correspondence:
Correspondence:
E Coetzee
emile@rectalsurgery.co.za


{kind=link}
{kind=link}
{kind=link}
{kind=link}