










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.54 no.4 Cape Town Nov. 2016
TRAUMA
Trauma unit attendance: Is there a relationship with weather, sporting events and week/ month-end times? An audit at an urban tertiary trauma unit in Cape Town
K L Milford; P H Navsaria; A J Nicol S Edu
Trauma Centre, Department of Surgery, Groote Schuur Hospital, and University of Cape Town
ABSTRACT
BACKGROUND: The Groote Schuur Hospital Trauma Unit is a high-volume referral center where patient volumes may be related to temporal and environmental factors.
OBJECTIVE: This audit aimed to determine if numbers of patients presenting after motor vehicle collisions (MVCs) and interpersonal violence (IPV) were related to temporal factors, weather variables and important soccer matches.
METHOD: Numbers of patients presenting to the unit per shift over 17 months were obtained from unit logs. Weather data, local soccer match locations and results, and information regarding public holidays and long weekends were obtained for the relevant shifts. Average daily attendances for IPV-related injuries and MVCs were compared across the various external factors described. Poisson regression models were fitted and used to express the relative incidence of attendances. These results are expressed using incidence rate ratios (IRRs).
RESULTS: For the study period, 7 350 attendances due to IPV-related injuries, and 3 188 injuries due to MVCs were recorded. Weekdays, long-weekend nights and month-end weekends had increased MVC-related attendance. Precipitation also increased attendances related to MVCs. Public holidays had less MVC-related attendance. IPV-related attendances were increased at night, on long weekends, and on month-end weekends. Weekend shifts were busier than weekday shifts, particularly at month-end. Long weekends showed similar trends to ordinary weekends, and public holidays showed similar trends to ordinary weekdays. Increasing temperatures are associated with increased attendances. Soccer matches and their outcomes have no significant effect on IPV-related attendances.
CONCLUSION: Temporal and weather factors can help predict which trauma unit shifts will be busiest.
Keywords: trauma unit, assault, motor vehicle collision, weather, temperature, sport
Introduction
"It's very clear; it's the first or second day of every month; whenever there's money and alcohol." - Dr Sa'ad Lahri, (SAMJ Izindaba November 2014), describing peak trauma times at Khayelitsha District Hospital in Cape Town.1
The number of patients presenting to a trauma unit can vary greatly from shift to shift and from day to day. Events leading up to a presentation at a trauma unit are unplanned and therefore unpredictable, but staff working in trauma units will report that factors such as time of the day, week and month, local weather conditions and major sporting events play a role in unit busyness. The purpose of this audit was to assess the relationship between temporal factors (time of day, week and month, public and religious holidays), weather variables and major soccer matches, and the volumes of patients presenting due to interpersonal violence (IPV)-related injuries and motor vehicle collisions (MVCs). There is a dearth of South African literature on the subject. Trauma unit staff anecdotally predict that the busiest times are month-end weekends, and the purpose of this audit was to test this theory, using data from the Trauma Unit at Groote Schuur Hospital in Cape Town.
The Trauma Unit at Groote Schuur Hospital is one of two tertiary-level, state-run adult trauma facilities in the Western Cape. Rates of interpersonal violence are high in Cape Town: the murder rate is higher than in any other South African city2 and thousands of assaults, common assaults and sexual assaults are reported each year.3 Motor vehicle collisions also occur frequently, with over 1 200 road fatalities in the Western Cape in each of the 2009/2010 and 2010/2011 periods.4 Victims of these assaults and accidents are treated at a variety of district and regional-level facilities around the city, but those requiring tertiary-level care will be referred on to Groote Schuur Hospital. Of note is that the Groote Schuur catchment area also includes some areas outside of the City of Cape Town metropole.
Temporal factors (time of day, week and month and public holidays), weather (temperature and precipitation) and soccer matches were chosen as the external factors to compare trauma unit volumes for this audit.
Regarding temporal factors, the conventional South African working week is from Monday to Friday with work on evenings, weekends and public holidays by special arrangement only.
Cape Town has a warm summer Mediterranean climate. Summer lasts from early December to March and is warm and dry, with average temperatures ranging from 16-26 °C. Winter, from the beginning of June to the end of August, is the wet season, with an average annual rainfall of 515 mm. Winter temperatures range from 8.5-18 °C on average.5
Soccer is a popular sport in South Africa, which played host to the FIFA Soccer World Cup in 2010. The Premier Soccer League (PSL) is the top-level football league in the country, and the Premier Division of this league consists of 16 clubs who play an annual tournament. Ajax Cape Town is a local club that has represented consistently in the Premier Division since its founding in 1998, but the two PSL clubs that enjoy the most enthusiastic support are Kaiser Chiefs and Orlando Pirates. The South African national team is known as Bafana Bafana.
Methods
Study design
This study was a retrospective audit.
Data Collection
Patients who presented to the Groote Schuur Hospital Trauma Unit as a result of injuries sustained due to interpersonal violence and motor vehicle collisions were included in the audit. The time frames were 8 January 2011 to 11 June 2011, and 14 November 2011 to 29 November 2012. The unit's admission logs, which record each patient attending the unit along with their presenting diagnosis or complaint, were studied. The logs for the period 12 June 2011-13 November 2011 were missing and could not be found, hence the gap. Attendances were entered into an Excel spreadsheet containing categories for interpersonal violence, motor vehicle collisions, accidents and miscellaneous incidents. MVC refers to all injuries sustained either as a driver or passenger in a motor vehicle, as a pedestrian or cyclist in collision with a motor vehicle, or injuries sustained in accidents involving trains. 'Accidents' were injuries that did not occur as a result of interpersonal violence or motor vehicle collisions (such as sporting injuries), and 'miscellaneous' events were those that did not conform to another category but are traditionally managed at this trauma unit (such as rings stuck on fingers). Each date of the study period was divided into two shifts (a day shift was defined as a period from 07h00 to 19h00, and a night shift was defined as a period from 19h00 to 07h00 the following morning), and attendances were recorded as a number of instances per shift.
Shifts that fell on South African public holidays were used in analyses comparing volumes on public holidays to other days, and if a public holiday fell on a Friday, Sunday (in which case it was celebrated on the Monday) or Monday, that weekend was considered a long weekend.
Details of home-team (Ajax Cape Town, Kaiser Chiefs, Orlando Pirates and Bafana Bafana) soccer matches were entered into the spreadsheet. Whether the team played at home or away was recorded, along with whether the team won, lost or drew the match. Archived Ajax, Chiefs and Pirates results were obtained from the PSL website, and archived Bafana results were obtained from the South African Football Association website.
Data regarding temperature and precipitation in Cape Town for the study period was obtained via personal correspondence with the South African Weather Service.
Statistical Analysis
Average daily attendances for IPV-related injuries and MVCs were compared across various temporal factors. Poisson regression models were fitted using Stata 13 (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP), and used to express the relative incidence of attendances. These results were then expressed using incidence rate ratios (IRRs).
Results
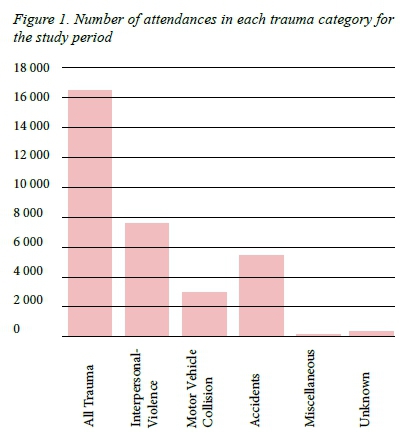
In total, 16 706 attendances were recorded over 1 074 shifts. Of these, 7 350 (44%) attendances were due to injuries sustained as a result of interpersonal violence (IPV), and 3 188 (19%) were due to MVCs (Figure 1).
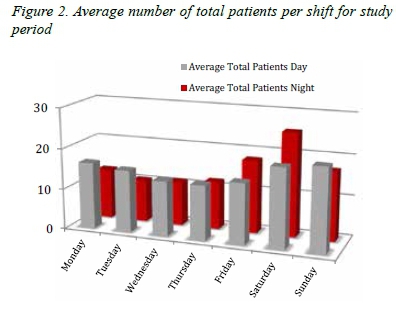
When looking at the averages for total numbers of patients presenting for all trauma types, it is clear that, on average, the weekends are busier than the weekdays. In general, the quietest shifts fall in the middle of the week (Tuesdays through Thursdays), with the night shifts being less busy than the day shifts (Figure 2). The fact that Mondays tend to be busier than other week days may represent delays in presentation after weekend incidents, possibly due to long waiting times at districtand secondary-level institutions and ambulance availability.
Motor Vehicle Collisions
Temporal relationships
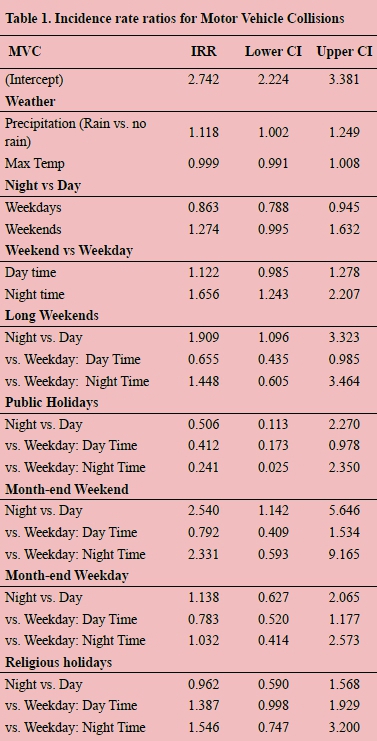
Comparing day shifts to night shifts, incidence of MVC-related injuries decreased by 14% (95% CI 0.79-0.95) on night shifts compared to day shifts during the week. On ordinary weekends and public holidays, there was no statistically significant difference in attendances for MVC-related injuries between day and night shifts. However, on long weekends attendances for MVC-related injuries increased by 93% (95% CI 1.10-3.32) at night compared to the day, and if the last day of the month fell on a weekend, attendances for MVC-related injuries increased by 156% (95% CI 1.14 - 5.65) on the night shift compared to the day shift.
Comparing week shifts to weekend shifts, there was no statistically significant difference between attendances for MVC-related injuries on an ordinary weekday and weekend day shift, but weekend nights saw a 66% (95% CI 1.24-2.21) increase in these injuries compared to week night shifts. Regarding public holidays, if the holiday fell on a weekday there was a 59% (95% CI 0.17-0.98) decrease in attendances for MVC-related injuries on the day shift compared to a normal weekday, and if the holiday formed part of a long weekend there was a 39% (95% CI 0.44-0.99) decrease in these types of injuries. Night shifts on public holidays and long weekends showed no statistically significant difference in attendance for these kinds of injuries when compared to ordinary week nights. Regarding0 month end, there was a trend towards increased MVC-related injuries at night if the last day of the month fell on a weekend, but this did not achieve statistical significance (CI 0.593-9.165) (Table 1).
Weather Relationships
The presence of rain on a particular day resulted in a 12% (95% CI 1.002-1.249) increase in attendances for motor vehicle-related injuries on that day. Change in temperature resulted in no significant change in the number of attendances (Table 1).
Interpersonal violence-related injuries
Temporal Relationships
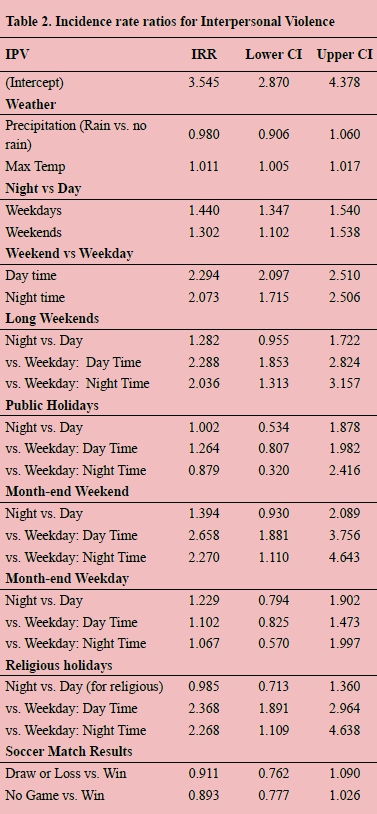
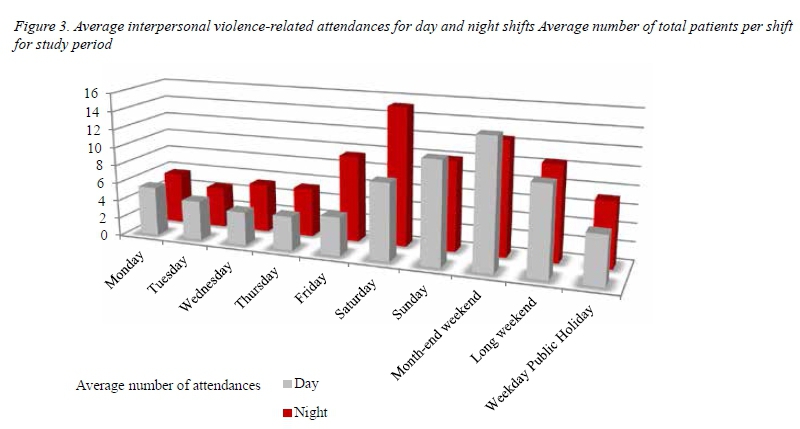
Attendances for IPV-related injuries increased for nighttime shifts compared to daytime shifts for both ordinary weekdays and weekends (Figure 3). During the week, night shifts see 44% (95% CI 1.35-1.54) more IPV-related injuries, and on weekends night shifts see 30% (95% CI 1.10-1.54) more IPV-related injuries compared to daytime shifts. Peculiarly, when looking at attendances for IPV-related injuries for night versus day shifts on public holidays, long weekends, and weekdays or weekends that fell on the last day of the month, there was no statistically significant difference.
Shifts on weekends are also busier than weekday shifts from an IPV perspective. Weekend day shifts see 130% (95% CI 2.10-2.51) more IPV-related injuries than daytime shifts during the week, and weekend night shifts see 107% (95% CI 1.7-2.5) more IPV-related injuries than weeknight shifts. This effect is particularly pronounced on weekends that fall on the last day of the month, where the day and nights shifts see an increase of 165% (CI 1.88-3.7) and 127% (CI 1.11-4.6) compared to their weekday counterparts, respectively. When the last day of the month falls on a week day, there is no statistically significant change in the numbers of IPV-related injuries compared to other week days.
Regarding IPV-related injuries, long weekends show a similar trend to ordinary weekends: the day shifts see a 128% (95% CI 1.85-2.82) increase compared to ordinary weekday shifts, and the night shifts see a 103% (95% CI 1.31-3.16) increase compared to ordinary week night shifts. If a public holiday does not form part of a long weekend, there is no significant difference in the number of IPV-related injuries on either the day or night shifts compared to corresponding shifts on an ordinary week day (Table 2).
Weather Relationships
The presence or absence of precipitation results in no significant change in attendances due to IPV-related injuries.
The lowest maximum temperature recorded for the study period was 8 °C. It was found that for every one degree increase in the maximum temperature for the day, there was a 1% increase attendance for IPV-related injuries (95% CI 1.01-1.02)
Soccer Matches
The volume of IPV-related attendances is not affected by whether or not a home or major team is playing a soccer match. This was found to be true regardless of whether the match was played at a local Cape Town stadium, whether or not the home team won (in the case of Ajax and Bafana Bafana games), and simply whether or not a match was played at all.
Discussion
Regarding interpersonal violence-related injuries, night shifts are busier than day shifts, and weekend shifts are busier than weekday shifts. Long weekends show a similar attendance pattern to normal weekends, but if a weekend falls on the last day of the month it is significantly busier than the others. This supports the anecdotal belief that assault times are highest when people have recently been paid, and aligns with international literature which shows that trauma units are generally busier at night,6 on weekends,6 and on the evenings before public and religious holidays, with a particular spike on New Year's Eve.7 Assaults, in particular, occur more frequently at night and on weekends.7,8
Weekends (and particularly month-end weekends) are likely busier from an IPV point of view than weekdays for several reasons. Chief among these is the fact that heavy alcohol consumption (which plays a large role in the presentation patterns at the unit, where it was found that alcohol was implicated in between 23% and 68% of IPV-related injuries9) is associated with increased violence.8 There is evidence that alcohol consumption increases on weekends10 and around payday.11 In addition, it is possible that increased interaction with others outside of the formal constraints of the work environment predisposes to increased assault.12
Although warmer temperatures seem to result in increased levels of assault, precipitation plays no role. This fitted with studies showing increased numbers of trauma unit visits in 'good' weather (warm and dry with long daylight hours),13 assault and violent crime in particular being been shown to be related to increasing temperatures.14
This audit also found that major soccer matches and the outcomes thereof had no impact on levels of interpersonal assault. This is not in keeping with international findings, where both local and international home-team sport matches are related to increased numbers of assaults.7,15 One local study from Cape Town demonstrated fewer trauma-related emergency department visits during the FIFA 2010 World Cup.16 This discrepancy between our findings and international findings could possibly be explained by a few things. Firstly, it is possible that South Africa in general and the Western Cape in particular has a higher 'baseline' level of IPV than countries that do demonstrate a spike in IPV on big soccer days, and that assaults that are related to soccer matches and their outcomes are masked by all the other assaults that would have occurred anyway. Secondly, South Africans have fairly varied interest in sport (they enjoy rugby and cricket in addition to soccer, and are also keenly interested in international soccer leagues as well as local ones), and assault spikes related to these many other sporting activities were not picked up by this data set.
Regarding MVCs, attendances were more numerous during weekday dayshifts than weeknight shifts. This may represent the fact that many MVCs occur during work hours, amongst people who are using roads during high-traffic periods. Weekend nights showed increased attendances compared to weeknights, and nightshifts on long weekends and month-end weekends were busier than dayshifts. International literature showed an increase in numbers of MVCs at times of poor visibility such as at night,17 and on weekends6,17 with increased fatality at these times.17 South African data shows that MVCs increase during the school holiday months.4
The nighttime increase in MVCs outside of the working week when traffic volumes are expected to be lower may represent MVCs that occur at times when people are driving more recklessly or whilst intoxicated (alcohol is implicated in 16.8% of MVC-related admissions to this unit).9
Rain results in increased numbers of MVCs, likely due to slippery roads and poor visibility resulting in more dangerous driving conditions. Rainfall intensity has been shown to be significant in predicting both crash incidence and severity.17
Study Limitations
This study gives insight into when busy times are expected and what types of trauma are likely to predominate. There still is a lot to learn, however, with regards to presentation patterns at this unit and others. The Trauma Unit at Groote Schuur is a tertiary level unit, and as such the patterns seen at this unit may not reflect those seen at district or secondary-level units. Also, this study looked only at absolute numbers of patients and not at trauma severity, and trends regarding this may be an area for further study. There are also other temporal factors that could be looked at. The period for which data was collected includes only one New Year's Eve, and so it was not possible to establish whether New Year's Eve (or Day) had any particular effect on trauma attendances. Also, the study only looked at 'day' and 'night' shifts: it may be useful to analyse hour-to-hour trends, as well as the impact of delays in referrals due to long waiting times at district- and secondary-level facilities or low ambulance availability. Finally, missing trauma logs have created an unfortunate temporal gap in this data.
Conclusion
It is possible to use temporal and some weather factors to predict which trauma unit shifts will be busier and which will be quieter, and what kinds of injuries can be expected. Although this study confirms many long-held beliefs about busy times in the unit, it provides data that should allow not only the trauma unit but also other pre- and in-hospital services to prepare appropriately for busy shifts. An analysis of trauma severity trends may be particularly useful to predict when high-resource areas such as the operating theatres and intensive care unit will be in most demand. In addition, the data should also be useful to those involved in traumaprevention, such as the traffic and police services.
REFERENCES
1. Bateman C. The smell of coffee, blood and disinfectant .... S Afr Med J. 2014;104(11):727-9. doi: 10.7196/SAMJ.9004 [ Links ]
2. Lancaster L. Where murder happens in South Africa - Africa Check. Africa Check. 19 September 2013 [Internet]. Available from: https://africacheck.org/2015/10/07/where-murder-happens-in-south-africa/ [ Links ]
3. Institute for Security Studies. SA Crime Stats [Internet]. Available from: https://www.issafrica.org/crimehub/top-20-precincts-per-category/2014 [ Links ]
4. Road Traffic Management Corporation. Road Traffic Management Corporation: Annual Report 2010/2011. 2011. [ Links ]
5. Wikipedia. Cape Town - Wikipedia, the free encyclopedia [Internet]. Wikipedia. 2014. Available from: http://en.wikipedia.org/wiki/Cape_Town#Climate [ Links ]
6. Ovadia P, Szewczyk D, Walker K, Abdullah F, Schmidt Gillespie S, Rabinovici R. Admission Patterns of an Urban Level I Trauma Center. Am J Med Qual. 2000;15(1):9-15. doi:10.1177/106286060001500103 [ Links ]
7. Bellis MA, Leckenby N, Hughes K, Luke C, Wyke S, Quigg Z. Nighttime assaults: using a national emergency department monitoring system to predict occurrence, target prevention and plan services. BMC Public Health. January 2012;12(1):746. doi: 10.1186/1471-2458-12-746. PMID: 22950487. [ Links ]
8. Nzaumvila D, Govender I, Kramer EB. Glass injuries seen in the emergency department of a South African district hospital. African J Prim Heal Care Fam Med. 2015;7(1):1-8. doi: 10.4102/phcfm.v7i1.886 [ Links ]
9. Nicol A, Knowlton LM, Schuurman N, Matzopoulos R, Zargaran E, Cinnamon J, et al. Trauma Surveillance in Cape Town, South Africa: An Analysis of 9236 Consecutive Trauma Center Admissions. JAMA Surg. 2014;149(6):549-56. doi: 10.1001/jamasurg.2013.5267. PMID: 24789507. [ Links ]
10. Lesch E, Casper R. "Drinking with respect": Drinking constructions of men who live in a Cape Winelands farm community in South Africa. J Health Psychol. 2015; Special Issue. doi: 10.1177/1359105315603476 [ Links ]
11. Chinyadza E, Moyo I, Katsumbe T, Chisvo D, Mahari M, Cock D, et al. Alcohol problems among patients attending five primary health care clinics in Harare. Cent Afr J Med. 1993;39(2):26-32. [ Links ]
12. Cohn EG. Weather and Crime. Br J Criminol. 1990;30(1):51-64. [ Links ]
13. Atherton WG, Harper WM, Abrams KR. A year's trauma admissions and the effect of the weather. Injury. 2005;36(1):40-6. doi: 10.1016/j.injury.2003.10.027. PMID: 15589911. [ Links ]
14. Gamble JL, Hess JJ. Temperature and Violent Crime in Dallas, Texas: Relationships and Implications of Climate Change. West J Emerg Med. 2012;13(3). doi: 10.5811/westjem.2012.3.11746 [ Links ]
15. Miller P, McDonald L, McKenzie S, O'Brien K, Staiger P. When the cats are away: the impact of sporting events on assault- and alcohol-related emergency department attendances.Drug Alcohol Rev. 2013;32(1):31-8. doi: 10.1111/j.1465-3362.2012.00481.x. PMID: 22715998. [ Links ]
16. Zroback C, Levin D, Manlhiot C, Alexander A, van As AS, Azzie G. Impact of the 2010 FIFA (Federation Internationale de Football Association) World Cup on Pediatric Injury and Mortality in Cape Town, South Africa. J Pediatr. 2014;164(2):327-31. doi: 10.1016/j.jpeds.2013.10.009. PMID: 24252783. [ Links ]
17. Zhao X, He X, Wu J, Zhao G, Ma Y, Zhang M, et al. Risk factors for urban road traffic injuries in Hangzhou, China. Arch Orthop Trauma Surg. 2009; (4):507-13. doi: 10.1007/s00402-009-0827-7. PMID: 19221774 [ Links ]
 Correspondence:
Correspondence:
Prof PH Navsaria
pradeep.navsaria@uct.ac.za


{kind=link}