










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Surgery
versión On-line ISSN 2078-5151
versión impresa ISSN 0038-2361
S. Afr. j. surg. vol.54 no.4 Cape Town nov. 2016
TRAUMA
The effect of emergency medical services response on outcome of trauma laparotomy at a Level 1 Trauma Centre in South Africa
S ChowdhuryI; P H NavsariaII; S EduIII; A J NicolIV
IDepartment of Surgery, Groote Schuur Hospital and University of Cape Town, South Africa
IIDeputy Director of Trauma Centre, Groote Schuur Hospital, and Professor of Surgery University of Cape Town, South Africa
IIISenior Consultant Trauma Surgeon, Groote Schuur Hospital and University of Cape Town, South Africa
IVHead and Director of Trauma Centre, Groote Schuur Hospital, and Associate Professor of Surgery, University of Cape Town, South Africa
ABSTRACT
BACKGROUND: Due to resource constrained pre-hospital emergency medical services (EMSs) there is a significant delay in injured patients arriving at Groote Schuur Hospital Trauma Centre (GSHTC). The aim of the study was to examine the effectiveness of EMSs in transferring trauma patients to GSHTC. The effect of any delay to laparotomy from injury was noted.
METHODS: A prospective audit of patients presented directly from the scene to GSHTC following abdominal trauma over a four-month period was performed. Time from contact to the arrival of EMS at scene - the response time (RT) - was used as an indicator of EMS performance. Postoperative complications were graded according to Clavien-Dindo classification of surgical complications.
RESULTS: A total of 118 patients were admitted to the trauma surgery ward following abdominal trauma. The mechanism was penetrating 101 (85.6%) [stab wounds in 67 (56.8%) and gunshot in 34 (28.8%)], and 17 (14.4%) with blunt injuries. EMSs transported 110 (93.2%) patients. A total of 48 index laparotomies were done during this period, of which 13 patients developed postoperative complications. The median RT of the EMS after contact was 53 min for patients who developed complications. It was significantly longer than for those without complications, 21 min (p < 0.01). The median delay to laparotomies from injury for patients with postoperative complications was 10.3 hours and for those without complications was 7.5 hours. The delay from injury to the theatre was also a significant factor in the development of complications (p = 0.02).
. CONCLUSION: The response delay by EMS and delay from injury to the theatre increased complications. Therefore, rapid response by EMS in transferring trauma patients needs to be strengthened.
Keywords: emergency medical services, response time, laparotomy, postoperative complications, outcome
Introduction
Trauma is the leading cause of non-natural deaths worldwide and a major cause of permanent disability. Violence is the most significant contributor to high rates of injury in the Western Cape. It accounts for 12.9% of premature mortality as compared to 6.9% for road traffic injuries.1
The Groote Schuur Hospital Trauma Centre (GSHTC) is one of two Level 1 trauma centres in Cape Town serving the greater Western Cape. At GSHTC, the sub-specialist surgical and ancillary services are on site and immediately available. This centre serves as a referral resource for designated communities in its region. It offers 24-hour in-house availability of required specialist disciplines: anaesthesiology and critical care, radiology, general surgery, emergency medicine, internal medicine, neurosurgery, oral and maxillofacial surgery, orthopaedic surgery and plastic surgery.2
At GSHTC, the trauma surgical ward care is run by three full-time trauma surgeons, one general surgeon and four general surgical registrars. There are eight high care beds and a 30-bed general trauma ward for acute admissions. A dedicated trauma theatre is available Monday through Thursday from 8 am to 5 pm. Trauma cases occurring after hours, on Fridays and on weekends, are done in the main emergency theatre. The trauma surgeons operate on the neck, chest, abdominal trauma and on most vascular injuries.
South Africa is one of the few countries on the African continent with an organised statutory system of pre-hospital care. Both the public and private sector run the emergency medical services (EMSs). No formal single emergency call centre exists currently. The vehicles and personnel dispatch independently upon receiving calls from the incident. Most of the EMS vehicles in the public sector are staffed with paramedics trained in basic to intermediate life support. The majority of the population does not have medical insurance and relies on public EMS, which is a significant burden for public EMS.3
Time since contact to the arrival of EMS at scene -the response time (RT) - is considered an indicator of EMS performance worldwide.4 Often trauma patients are haemodynamically unstable from hypovolaemic shock following an injury. The urgent response of an EMS is essential for initiation of resuscitation, rapid transfer of the patient to definitive care facilities and prevention of further physiological deterioration.
The aim of the study was to examine the effectiveness of EMS in transferring patients with abdominal trauma to GSHTC. The effect of any delay to laparotomy was noted.
Methods
The study was a University of Cape Town (UCT) Human Research Ethics Committee (HREC) approved (Ref: 440/2013) observational, non-interventional, and descriptive study based on the prospective analysis of data related to patients presented directly from the scene to GSHTC following abdominal trauma and admitted to the trauma ward from 01 December 2013 to 31 March 2014. Patients' demographic details, geographical area of injury, mechanism of injury, time of injury, injury severity score (ISS), EMS response time (RT), time taken to arrival at GSHTC, time taken to surgery, delay from injury to theatre, total hospital stay and outcome in Postoperative surgical complications were graded according to the updated Clavien-Dindo classification of surgical complications.5,6
Categorical variables were assessed using frequency tables. Numerical variables were evaluated with summary statistics (median, interquartile range (IQR), etc.). A p-value of < 0.05 was considered to be significant.
Results
A total of 118 abdominal trauma patients presented directly from the scene during the period of study, with a significantly higher male to female ratio of 9:1. The median age was 25 (IQR 21-31) years. One hundred and one patients (85.6%) were admitted following penetrating trauma. Stab wounds comprised 67 patients (56.8%) and gunshot wounds (GSW) 34 (28.8%). The number of admissions due to blunt trauma was 17 (14.4%). The median ISS for a gunshot wound, stab wound, and blunt trauma was 18 (IQR 16-25), 10 (IQR 3-18), and 22 (IQR 17-27) respectively. Sixty-six patients (56%) were admitted with ISS > 15. EMSs transported 110 patients (93.2%). With respect to different ambulance services, government service (Metro) carried the majority of patients [106 (89.8%)], followed by private ambulance service [4 (3.4%)]. Only eight patients (6.8%) arrived at the hospital in their own or a private vehicle. EMS transported all patients who developed postoperative complications.
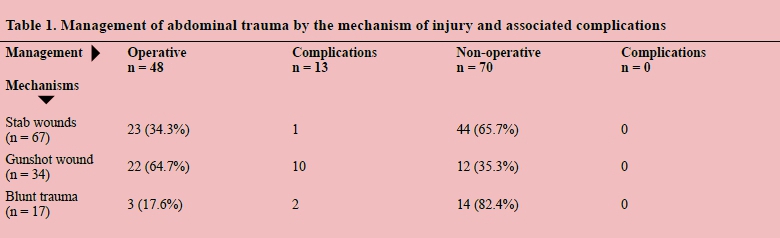
Seventy patients (59.3%) were managed conservatively. Forty-eight patients (40.7%) required surgery. Table 1 shows the management of abdominal trauma by the mechanism of injury.
Thirteen patients (27.1%) developed postoperative complications as listed in Table 2. Surgical site infection (SSI) and organ failure remained major postoperative complications.
The median hospital stay for all patients was 6 days (IQR 4-11). The median length of stay was significantly longer in patients who developed postoperative complications than in those who did not [16 (IQR 10-20) d vs. 5 (IQR 4-7) d, p < 0.01]. Only 1 patient (0.8%) died. The patient was a 17-year-old boy who was an unrestrained passenger involved in a motor vehicle accident. He was brought in by EMS and had sustained polytrauma including head injury, blunt abdominal trauma and pelvic fracture. On presentation to GSHTC, he was haemodynamically stable, and his Glasgow Coma Scale (GCS) was 8. His ISS was 34. His computed tomography (CT) scan of the brain and abdomen showed a sliver of left subdural and subarachnoid haemorrhage, pelvic fracture, grade 1-2 spleen fracture, and perinephric haematoma around the left kidney with suspected hollow visceral injury. He had a non-therapeutic exploratory laparotomy with spleen and kidney preservation. Postoperatively, he was admitted to the intensive care unit (ICU). His head injury and pelvic fracture were managed conservatively. He died on day 15 post-admission due to severe sepsis and multiorgan failure. His ambulance RT, injury to arrival at GSHTC, booking to start surgery and injury to theatre time were 53 min, 105 min, 100 min and 487 min respectively.
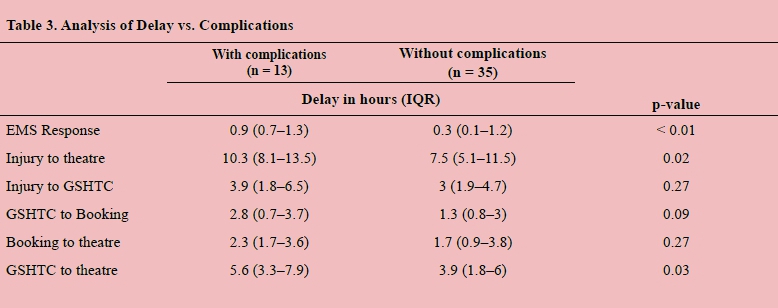
Analysis of delay vs. complications
The median RT of the EMS after being contacted was 53 min (IQR 46-78) for patients who developed postoperative complications, which was significantly more than those without complications, which was 21 min (IQR 10-75, p < 0.01). The median delay from injury to the theatre [with complications 10.3 hours (IQR 8.1-13.5), without complications 7.5 hours (IQR 5.1-11.5)] was a significant factor in the development of complications (p = 0.02). The median delay from the injury to arrival at GSHTC [with complications 3.9 hours (IQR 1.8-6.5), without complications 3 hours (IQR 1.9-4.7), p = 0.27] and from booking the case to start with surgery [with complications 2.3 hours (IQR 1.7-3.6), without complications 1.7 hours (IQR 0.9-3.8), p = 0.27] did not show a significant difference between both groups of patients (Table 3).
Subgroup analysis of gunshot abdomen patients
Out of thirty-four gunshot abdomen patients, 22 (64.7%) required surgery. In this group, 10 patients (45.5%) developed postoperative complications. The median response delay by EMS for gunshot abdomen patients with complications was 51 min (IQR 40-82), without complications 19 min (IQR 8-48), which was significant in the development of postoperative complications (p < 0.01). Also, the median delay from injury to the start of surgery for gunshot abdomen patients [with complications 10.7 hours (IQR 8.2-12.9), without complications 5.7 hours (IQR 3.4-10.8, p = 0.03) was also significant. The median ISS for gunshot patients with postoperative complication was 25 (IQR 16-25) and without complication was 16 (IQR 16-23). There was no association of severity of injury in the development of complications (p = 0.22).
Discussion
It is well known that the outcome improves when a trauma patient is transported to a designated trauma centre within an hour of injury - the "golden hour".7 This "golden hour" is supported by two significant studies by Sampalis et al. in 1993 and 1999. Both studies showed reduced mortality associated with the reduction of pre-hospital time.8,9 Shortened pre-hospital time was found to be associated with better outcomes in the case of trauma patients, such as patients with severe thoracic injuries, severe head injuries and intra-abdominal bleeding.7
The concept of the golden hour is disputable in many countries. In 2010, a prospective cohort study in North America by Newgard et al. showed there is no relationship between in-hospital mortality and EMS transfer of severely injured patients.10 More recently in Germany, Kleber et al. (2012) also found no significant survival benefit with shorter pre-hospital time.11 The result is also supported by various studies done at other centres in America and Europe.7
The reduction of pre-hospital time largely depends on the efficiency of the EMS system and especially on RT. In the event of a life-threatening condition, the rapid response of the EMS is an expectation, and it is used to measure the effectiveness of a pre-hospital system.4 The history of RT can be traced back to a Seattle study in 1979 where the survival of cardiac arrest patients improved after basic life support (BLS) and advanced life support (ALS) initiated within four and eight minutes respectively. Several studies were done subsequently and showed similar timeframes. In 2002, Blackwell et al. showed EMS response times less than five minutes are associated with improving survival.12 Later in 2005, Pons et al. found significant survival benefit, if the EMS response times were within four minutes.13 Both trauma and non-trauma emergencies were included in these studies. Eight-minute response time was set as a standard for EMS operations by many authorities, but its validity was challenged by many subsequent studies.4 It is wrong to have an arbitrary response time limit for all trauma and non-trauma emergencies. A cardiac arrest patient or one with penetrating trauma to the heart might need immediate attention of the EMS. On the other hand, a patient who sustained lower limb fracture following a motor vehicle accident might not need EMS response within eight minutes. So EMS response time should be according to the merit of the case. According to Campbell MacFarlane, in South Africa, EMS system RT varies from 15 min in an urban area to 40 min or longer in some rural areas due to the disproportionate distribution of services; in addition, many rural areas are poorly resourced as a result of historical inequalities.14
In the current study, it has been shown that the EMS response time is longer than the standard for abdominal trauma patients. It has also demonstrated that the patients who developed postoperative complications had longer EMS response time as well as a delay in access to surgery. After arrival to GSHTC, the group of patients who experienced complications took significantly longer time to go to theatre than the group who did not experience complications. This was possibly due to various in-hospital factors like longer time for resuscitation, investigations, multi-system involvement, waiting for decisions from different specialties in stable patients and finally decision making for surgery. On the other hand, after arrival to GSHTC the time delay to booking and delay after booking to start the surgery did not show any statistically significant outcome difference in both groups due primarily to effective emergency surgical case triaging method by the surgeon and finally by the anaesthesiologist at GSH.
Developing postoperative complications depends on various factors including patient factors, the nature of the injuries, contamination, operative delay, operative techniques, local facilities, and postoperative care. Despite the conflicting evidence about RT and the "golden hour", it is not illogical to conclude that taking the patients to a definitive care facility as early as possible following an injury must play a role in decreasing complications and improving outcome.
Conclusion
Penetrating trauma continues to be a significant burden on the resources of a trauma centre. The response delay by EMSs and delay from injury to theatre increases complications. Delay in surgery for gunshot abdomen patients is associated with potentially graver complications. These patients should be rapidly transferred by EMS to a trauma centre.
EMSs play a fundamental role in transporting patients worldwide. The EMS in South Africa has developed rapidly over the last decades. Available transport vehicles, both ground and aeromedical, should be placed strategically rather than based on facility and be used as a means to facilitate timely access and response, especially in the least accessible areas. Both government and private entrepreneurs should come forward to increase pre-hospital personnel as well as logistics to improve the current EMS system. Only an integrated modern EMS and first responders can help to provide faster access and more seamless patient transfer throughout the health care system.
REFERENCES
1. Bradshaw D, Nannan N, Laubscher R, et al. South African National Burden of Disease Study 2000: Estimates of Provincial Mortality. Summary Report, March 2006. http://www.mrc.ac.za/bod/estimate.pdf (accessed 7 June 2016). [ Links ]
2. Hardcastle TC, Steyn E, Boffard K, et al. Guideline for the assessment of trauma centres in South Africa. S Afr Med J. 2011;101(3):189-194. [ Links ]
3. Hardcastle TC, Finlayson M, Van Heerden M, et al. The Prehospital Burden of Disease due to Trauma in KwaZulu-Natal: The Need for Afrocentric Trauma Systems. World J Surg. 2013;37:1513-1525. [ Links ]
4. Al-Shaqsi SZK. Response time as a sole performance indicator in EMS: Pitfalls and solutions. Open Access Emergency Medicine. 2010;2:1-6 [ Links ]
5. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205-213. [ Links ]
6. Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187-196. [ Links ]
7. Rogers FB, Rittenhouse K. The golden hour in trauma: Dogma or medical folklore? The Journal of Lancaster General Hospital. 2014;9(1):11-13. [ Links ]
8. Sampalis JS, Lavoie A, Williams JI, et al. Impact of on-site care, pre-hospital time, and level of in-hospital care on survival in severely injured patients. J Trauma. 1993;34(2):252-261. [ Links ]
9. Sampalis JS, Denis R, Lavoie A, et al. Trauma care regionalization: a process-outcome evaluation. J Trauma. 1999;46(4):565-581. [ Links ]
10. Newgard CD, Schmicker RH, Hedges JR, et al. Emergency medical services intervals and survival in trauma: assessment of the "golden hour" in a North American prospective cohort. Ann Emerg Med. 2010;55(3):235-246 [ Links ]
11. Kleber C, Lefering R, Kleber AJ, et al. Rescue time and survival of severely injured patients in Germany. Unfallchirurg. 2013; 116(4):345-350. [ Links ]
12. Blackwell TH, Kaufman JS. Response time effectiveness: comparison of response time and survival in an urban EMS system. Acad Emerg Med. 2002;9(4):288-295. [ Links ]
13. Pons PT, Haukoos JS, Bludworth W, et al. Paramedic response time: does it affect patient survival? Acad Emerg Med. 2005;12(7):594-600. [ Links ]
14. MacFarlane C, van Loggerenberg C, Kloeck W. International EMS systems in South Africa - past, present, and future. Resuscitation. 2005;64 (2):145-148. [ Links ]
 Correspondence:
Correspondence:
Sharfuddin Chowdhury
dr_smahmud@yahoo.com


{kind=link}
{kind=link}
{kind=link}