










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.54 n.3 Cape Town Sep. 2016
CASE REPORT
Perforated appendicitis presenting as a thigh abscess: a lethal combination
S Naidoo; R Du Toit; A Bhyat
Department of General Surgery, Kimberley Hospital Complex, Kimberley
ABSTRACT
Typical cases of acute appendicitis have excellent treatment outcomes, if managed appropriately.1 We discuss an unusual case of perforated retrocaecal appendicitis that presented as a right thigh abscess without prominent abdominal symptoms, which highlights the lethal nature of advanced appendicitis even when appropriate surgical therapy is instituted.
Case report
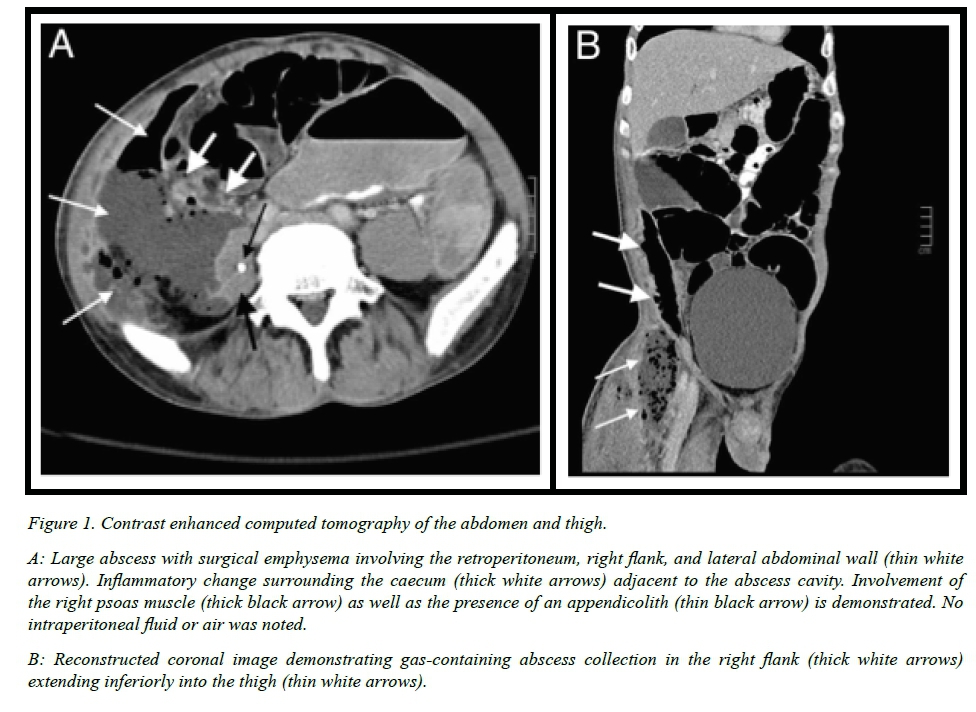
A 50-year-old male was seen in the emergency department complaining of painful disability of his right leg. The affliction began a week prior with pain located primarily at the right hip. The pain then worsened and spread to the thigh and knee, with associated swelling and progressive inability to bear weight on the limb. He denied abdominal pain, but experienced mild anorexia during the preceding week. There was no history of trauma or chronic illness. Physical examination revealed an acutely ill man with the following vital signs: heart rate 120 beats per minute, blood pressure 110/57 mmHg, respirations 20 breaths per minute, and temperature 38.8°C. Tenderness in the right iliac fossa and flank was appreciated, and the impression of a mass was noted. There was also erythema and swelling of the overlying abdominal skin. The right hip was maintained in flexion and external rotation, with significant limitation of movement demonstrated. The limb was severely inflamed, with a large fluctuant area extending from the groin to the knee. There was no evidence of crepitation at the affected sites. Significant laboratory results included white cell count, 13 180/mm3 and C-reactive protein, 297 mg/l. Contrast-enhanced computed tomography (CT) revealed features in keeping with perforated appendicitis, with large right-side retroperitoneal abscess and right thigh involvement (Figure 1).
Emergency laparotomy confirmed perforated retrocaecal appendicitis, with large retroperitoneal abscess that extended from the hepatic flexure of the colon, downward along the right psoas muscle and into the thigh. The peritoneal cavity was free from contamination. Right leg exploration then confirmed abscess extension into the limb via the iliopsoas muscle behind the inguinal ligament. Copious volumes of offensive pus were found in the anterior and medial compartments of the thigh, extending to just below the knee. Although small areas of myonecrosis were encountered, suppuration without necrotizing infection was the predominant feature.
Appendectomy was performed and the right leg incised and drained. Necrotic tissue was debrided and thorough irrigation of the affected area was carried out. Broad-spectrum antibiotics were commenced and later changed appropriately after surgical cultures revealed non-haemolytic streptococci and Escherichia coli. The patient underwent repeat debridement procedures at two and six days after the initial surgery. He continued to improve satisfactorily until he developed severe diarrhoea three weeks after admission. The patient deteriorated despite maximal treatment, his condition complicated by electrolyte disturbances and malnutrition. He eventually succumbed to severe sepsis two months after admission to hospital.
Discussion
Although perforated appendicitis is a well-established cause of retroperitoneal abscess formation,2 the absence of abdominal or flank pain, as well as extension into the thigh as seen with this case, is rare.3 Pus, bowel contents and gas can reach the leg by various routes. The most common pathway, and the route taken in this case, is along the iliopsoas muscle into the thigh and through Hunter's canal to reach the medial part of the knee.4,5 This case highlights important issues common to perforated retroperitoneal appendicitis. Insidious presentation with vague symptoms is common. CT is an important tool to make the diagnosis, delineate the extent of involvement, and plan surgery. Patients have prolonged hospital admission and demonstrate significant morbidity and mortality. A high index of suspicion and expeditious management are required to successfully treat this grave disease.
CONSENT
Written informed consent was obtained from the patient for publication of this report and any accompanying images. A copy of the written consent is available for review by the Editor-in -Chief of this journal.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest.
AUTHORS' CONTRIBUTIONS
SN conceived the paper, performed the literature search and drafted the manuscript. RD and AB performed the surgeries and revised the manuscript. All authors read and approved the manuscript for submission.
REFERENCES
1. Ong EMW, Venkatesh SK. Ascending retrocecal appendicitis presenting with right upper abdominal pain: Utility of computed tomography. World J Gastroenterol. 2009;15(28):3576-3579. [ Links ] [PMID: 19630119] [http://dx.doi.org/10.3748/wjg.15.3576]
2. Litkouhi B, Huang AS, Lundy DJ, Solis M. Perforation of a retrocecal appendix resulting in retroperitoneal air: a case report. Case Rep Radiol. 2013;(2013):584925. [ Links ] [PMID: 23476871] [http://dx.doi.org/10.1155/2013/584925]
3. Dheer AK, Carr B, Morrison P, Watson N. Appendicular abscess and a swollen knee. Lancet. 2001;358(9290):1366-1367. [ Links ] [PMID: 11684243] [http://dx.doi.org/10.1016/S0140-6736(01)06425-X]
4. Pande SD, Hossenbocus A. A swollen right leg. Lancet 2001;357(9270):1762. [ Links ] [PMID: 11403815] [http://dx.doi.org/10.1016/S0140-6736(00)04899-6]
5. Greenway BA. An unusual presentation and complication of acute appendicitis. Postgrad Med J. 1978;54(632):425-426. [ Links ] [PMID: 683916] [http://dx.doi.org/10.1136/pgmj.54.632.425]
 Correspondence:
Correspondence:
Sashelin Naidoo
sashelin@smail.com


{kind=link}