










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Surgery
versión On-line ISSN 2078-5151
versión impresa ISSN 0038-2361
S. Afr. j. surg. vol.54 no.3 Cape Town sep. 2016
CASE REPORT
Primary seromucinous cystadenocarcinoma of the mesentery
S SobnachI; J C KloppersI; S BurmeisterI; M LocketzII; L RoodtI; S R ThomsonI; J E J KrigeI
ISurgical Gastroenterology Unit and Department of Surgery, Faculty of Health Sciences, University of Cape Town, Republic of South Africa
IIDepartment of Anatomical Pathology, Faculty of Health Sciences, University of Cape Town, Republic of South Africa
ABSTRACT
A 72-year-old woman presented with a slow growing mass on the left side of the abdomen, which was found to originate from the mesentery of the descending colon. Histopathology revealed a seromucinous cystadenocarcinoma of the mesentery, a rare clinical entity occurring most often in females. There are only 20 cases reported in the literature. It is postulated that these tumours develop as a result of serous or mucinous metaplasia of pre-existing coelomic mesothelium. Surgical excision remains the mainstay of successful management.
Background
Benign and borderline cystic mucinous tumours of the mesentery and retroperitoneum are rare, with an incidence of about 1 per 100 000 of hospitalised patients. The disease predominantly affects women and occurs in patients of all ages. A primary mesenteric seromucinous cystadenocarcinoma, however, is an extremely rare clinical entity. There are only 20 reported cases in the literature. Although the pathogenesis is poorly understood, it is postulated that these tumours develop through serous or mucinous metaplasia of preexisting coelomic mesothelium. Surgical excision remains the mainstay of successful management.1-2
Case report
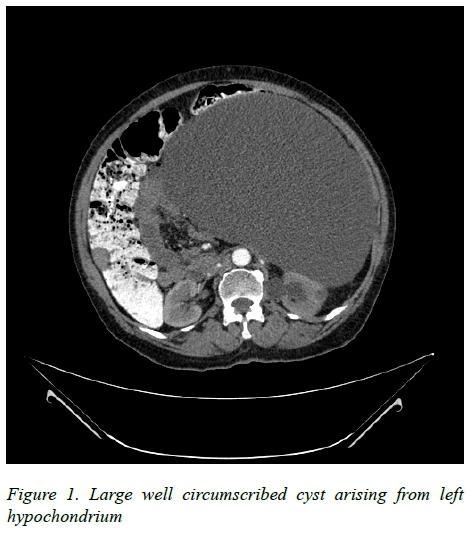
A 72-year-old woman was referred with a three-year history of abdominal discomfort, weight loss and increased abdominal girth. On physical examination there was a mass in the epigastrium, which extended to the left hypochondrium. The mass was non-tender and mobile. All her blood tests results including Full Blood Count, Carcinoembryonic Antigen (CEA) and Carbohydrate Antigen (CA19-9) levels were normal. However, a percutaneous aspirate obtained at the referring institution revealed an elevated CEA of 32845.7 (normal range: 2.5-5.0). Abdominal CT scan showed a large well-circumscribed cystic mass with features suggestive of a mesenteric cyst (Figure 1).
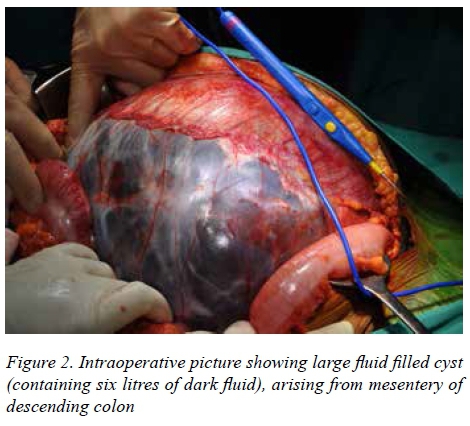
At surgery, a large cyst containing six litres of fluid was dissected free from the left descending mesocolon (Figure 2); no colonic resection was required. Further inspection of the peritoneal cavity confirmed normal hollow viscera, unremarkable solid organs and no lymphadenopathy. Her postoperative course was uneventful. Histopathological assessment confirmed a completely excised cyst. The wall was thick and fibrotic with focal dystrophic calcification and aggregates of lymphocytes. The cyst lining included a variable glandular epithelial lining, ranging from single-layered mucus-secreting cells to multilayered dysplastic papillary epithelium with admixed goblet cells. Superficial invasion of the cyst wall by adenocarcinoma with a stromal response was present (Figure 3). No ovarian stroma was observed. Predominantly acidic mucin was present on Alcian Blue Periodic Acid Schiff staining. The tumour was strongly positive for CK7 and CK19 but focally positive for CK20. These findings were in keeping with the diagnosis of a primary seromucinous cystadenocarcinoma.

After multidisciplinary assessment and discussion with the patient, adjuvant chemo-radiation was not undertaken, and a conservative approach with regular clinical follow-up was adopted.
Discussion
Primary seromucinous cystadenocarcinoma of the mesentery is rare. The histogenesis of this condition is still poorly understood. It is postulated that these tumours arise from müllerian or paramesonephric duct remnants, which were deposited when the ovary descended during embryogenesis. The tissue remnants subsequently undergo proliferation and mucinous metaplasia.3 Immunoreactivity for intestinal markers and point mutations within the K-ras oncogene have also been documented in these lesions.4
In this particular case, the tumour is classified as an extra-ovarian seromucinous cystic neoplasm due to the absence of ovarian stroma on histology. Although its origin is debatable, the most likely scenario is that the initial pathology was a benign mesenteric cyst with subsequent malignant transformation.
The mainstay of therapy for patients with large cysts with a suspicion of malignancy is surgery. Laparoscopy should be reserved for small cysts where the risk of rupture is small as cyst rupture at surgery negatively affects survival and predisposes to peritoneal carcinomatosis.1-4 A biopsy should only be performed when a palliative scenario is encountered. Patients with cyst rupture and wall invasion on histology may benefit from chemotherapy or radiation.1 Due to the paucity of data in the literature, the management of these tumours should be individualized.
REFERENCES
1. Linden PA, Ashley SW. Mucinous cystadenocarcinoma of the mesentery. Surgery. 2000 Jun 30;127(6):707-8. [ Links ]
2. Obuchi T, Shimooki O, Sasaki A, Abe T, Wakabayashi G. Serous cystadenocarcinoma of the mesentery in a man: case report and review of literature. Gastroenterology Report. 2014 Nov 1;2(4):306-10. [ Links ]
3. Pennell TC, Gusdon JP. Retroperitoneal mucinous cystadenoma. American Journal of Obstetrics and Gynecology. 1989 May 31;160(5):1229-31. [ Links ]
4. Tenti P, Romagnoli S, Zappatore R, Giunta P, Carnevali L, Pellegata NS, Ranzani GN. Primary retroperitoneal mucinous cystoadenocarcinomas: an immunohistochemical and molecular study. Virchows Archiv. 1994 Jan 1;424(1):53-7. [ Links ]
 Correspondence:
Correspondence:
S Sobnach
sanjusobnach@yahoo.com

