










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.54 no.3 Cape Town Set. 2016
CASE REPORT
Perforated caecal duplication cyst presenting as an appendicular abscess
J Sookram; N Naidoo; S Cheddie
Madadeni Hospital, Department of General Surgery, University of KwaZulu-Natal and Nelson R Mandela School of Medicine, Durban, South Africa
ABSTRACT
A duplication cyst of the caecum is a very rare congenital malformation, representing 0.4% of all gastrointestinal duplications. We present a case of cystic duplication of the caecum in a 12-year-old child who presented with a right iliac fossa mass and peritonitis. An ischaemic, perforated caecal duplication cyst was found on emergency laparotomy, mandating a right hemicolectomy.
Gastrointestinal duplication covers a wide variety of lesions throughout the alimentary tract, which can either be cystic or tubular, occurring at any level, from the base of the tongue to the anus. The terminal ileum is the most common site. Only 13% of all gastrointestinal duplications arise from the colon. The clinical presentation depends on the location, size and presence of ectopic gastric mucosa. Patients may present at any age, but 80% present in the first two years of life.1 Less than 20 cases of caecal duplication cysts have been reported in the English literature. This report describes the first case of a perforated caecal duplication cyst in a child.
Case study
A 12-year-old boy presented with colicky abdominal pain, vomiting and constipation for three days, which was worsening in severity. He had had a previous orchidopexy for an undescended testis, and was human immunodeficiency virus positive, and on highly active antiretroviral therapy.
The physical examination revealed a right lower quadrant mass and generalised peritonitis. Plain abdomen radiographs demonstrated a normal bowel gas pattern. Free air was not found under the diaphragm following an erect chest radiograph. An elevated white cell count (12.8 x109/l), normal C-reactive protein and raised erythrocyte sedimentation rate of 70mm/hour were reported after haematological analysis. The biochemistry analysis revealed metabolic acidosis (serum bicarbonate 16mmol/l).
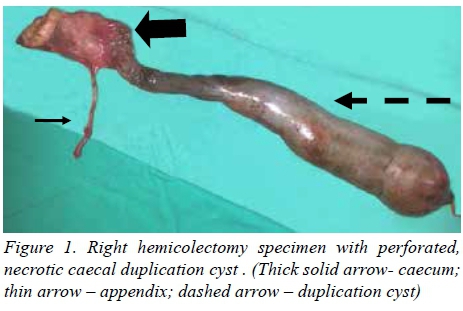
A gangrenous perforated duplication cyst of the caecum with faecal peritonitis was found during an exploratory laparotomy. A right hemicolectomy was performed and owing to extensive faecal contamination, an end ileostomy and mucus fistula was fashioned. Histopathology of the right hemicolectomy specimen revealed a 7cm segment of colon, in which two duplication cysts were identified. There was a perforation measuring 1.5cm in diameter in the larger cyst, which measured 36cm by 8cm, with evidence of transmural haemorrhage, infarction and perforation, together with an organising peritonitis. Ectopic mucosa, granulomatous inflammation and neoplasia were not identified. The postoperative course was uneventful.
Discussion
The occurrence of alimentary tract duplication cysts was first document in 1733 by Calder.2 Subsequently in 1937, Ladd utilised the term "duplication of the alimentary tract" to report congenital anomalies which involve the mesenteric border of the associated alimentary tract and share a joint blood supply with the native bowel.3 Duplication of the gastrointestinal tract is defined according to histological features, i.e. of having a well developed coat of smooth muscle, an inner mucosal lining, and firm attachment to at least one point of the alimentary tract.4 The majority of duplications are cystic in nature (53-85%), and the remaining are tubular and generally larger in size, with a tendency to communicate with the contiguous gut lumen.3 Duplication occurs most commonly in children, with an incidence of 1 in 5 000 live newborns.3 Cystic duplications of the gut are more common in female infants, with a male to female ratio of 1.0:2.3, and most patients present within three months of birth. A palpable abdominal mass is present in 50% of cases.5 Abdominal sites of duplication cysts include the ileum (30%), ileocaecal valve (30%), stomach (8%), jejunum (7%), colon (7%) and rectum (5%).
Oudshoorn and Heij reported only 16 cases (0.4%) of caecal duplication.6 Colonic duplication appears to be associated with a higher incidence of various congenital anomalies. The genitourinary tract is most commonly involved.4 Our index patient had a history of an undescended testis.4
The aetiology of gastrointestinal tract duplication formation is unclear. Hypotheses on the embryological formation include the following:
Split notocord syndrome.
• Abnormalities of recanalisation of the solid stage.
• The abortive twinning theory.
• The theory of embryological diverticulae.
• The theory of environmental factors, such as hypoxia and trauma.3
Malignant transformation of duplication cysts in adulthood has been sporadically reported.1 Common signs and symptoms of duplication are variable. Clinical presentations include:
• Intestinal obstruction, as a result of intussusception or compression of the adjacent bowel.
• Pain relating to distension of the cyst due to the accumulation of secretions or from infection of the content, and inflammation of the surrounding viscera.
• Gastrointestinal bleeding owing to ulceration which develops due to ectopic gastric mucosa, or interference with the vasculature.
• Respiratory distress, i.e. an intrathoracic duplication cyst.
• Asymptomatic, and discovered incidentally by routine X-ray.6
The diagnosis is usually established intraoperatively. However, imaging modalities may be used when there is diagnostic doubt. Ultrasound is the most common first-line imaging modality, and the "double wall" sign is highly suggestive of enteric duplication. Computed tomography (CT) scans and magnetic resonance imaging are more sensitive that ultrasound in prenatal foetal duplication diagnosis.3 The CT shows a well defined cystic structure, with low attenuation and contrast enhancement of the outer rim. Additional imaging modalities, such as a technetium-99m pertechnetate scintigraphy scan, can be used to demonstrate the presence of ectopic gastric mucosa in some duplication cysts.1
The treatment of choice is open surgery, which entails simple removal of the cystic duplication from where it is attached, or resection with the adjacent bowel segment, and primary end-to-end anastomosis.3 The Bianchi technique is preferred for tubular duplications which are long, and involves preservation of the adjacent bowel, and removal of the duplicated portion only, so as to prevent short bowel syndrome.3 Limited resection or mucosal stripping may be performed to save the adjacent bowel length in the presence of ectopic gastric mucosa. Laparoscopic resections can be performed with low morbidity, and excellent outcomes have been reported from specialised centres.3
Conclusion
Alimentary tract duplication cysts are rare, but should always be considered in the differential diagnosis of an acute abdomen in the paediatric population. Caecal duplication cysts can be an incidental finding, or may mimic an appendicular abscess or malignant mass. The majority of patients present in infancy, and surgical excision is the mainstay of therapy to prevent future complications.
REFERENCES
1. Keum S, Hwang MW, Na JI, et al. Intestinal obstruction caused by a duplication cyst of the cecum in neonate. Korean J Pediatrics. 2009;52(2):261-263. [ Links ]
2. Sudhamani S, Nahar A, Pandit A, et al. Duplication cyst of the caecum: a rare case report with review of literature. Bombay Hospital J. 2011;53(1):82-84. [ Links ]
3. Zavras N, Christianakis E, Papakonstantinou D, et al. Alimentary tract duplications in infancy and childhood. A 25- year experience with focus on rare types of the disease. OJ Ped. 2013;3(4):324-330. [ Links ]
4. Temiz A, Oguzkurt P, Serin SE, et al. Different clinical presentations, diagnostic difficulties, and management of cecal duplication. J Pediatr Surg. 2013;48(3):550-554. [ Links ]
5. Simmi K, Kulsreshtha R, Ratan J. Cystic duplication of the cecum with segmental dilatation of the ileum: report of a case. Surg Today. 2001;31(1):72-75. [ Links ]
6. Oudshoorn JH, Heij HA. Intestinal obstruction caused by duplication of the caecum. Eur J Pediatr. 1996;155(4):338-340. [ Links ]
 Correspondence:
Correspondence:
Jayveer Sookram
scheddie@gmail.com

