










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.54 no.3 Cape Town Set. 2016
GENERAL SURGERY
Comparing laparoscopic appendectomy to open appendectomy in managing generalised purulent peritonitis from complicated appendicitis: the uncharted path
B NdoforI; S MokotediI; M KotoII
IDepartment of Surgery, Sebokeng Hospital and the University of the Witwatersrand, Johannesburg, South Africa
IIDepartment of Surgery, Sefako Makgatho Health Sciences University
ABSTRACT
BACKGROUND: The objective of the study was to compare the outcomes of patients with generalised purulent peritonitis from complicated appendicitis diagnosed intraoperatively who were managed laparoscopically to those managed via the open approach in a single institution.
METHODS: Data were collected from all cases admitted at Sebokeng Hospital, Johannesburg, over the past two years (2008 and 2009) with an intraoperative diagnosis of generalised purulent peritonitis from complicated appendicitis. Cases managed laparoscopically or by the open approach were analysed. The demographic findings, theatre duration, complications, days to the commencement of a full ward diet and the length of the hospital stay were the analysed parameters.
RESULTS: One hundred and twenty appendectomies with generalised purulent peritonitis were performed during the study period. Of these, 58 patients underwent open appendectomy, and 62 patients had laparoscopic appendectomy. Both groups were comparable with regard to the demographics and preoperative findings. Theatre duration was significantly higher in the laparoscopic appendectomy group -116 minutes for a laparoscopic appendectomy compared to 87 minutes for an open appendectomy. The rate of intra-abdominal sepsis was also higher in the laparoscopic appendectomy group - 13% for a laparoscopic appendectomy, and 9% for an open appendectomy. A statistically significant decrease in the wound sepsis rate was shown in the laparoscopic appendectomy group. No statistical significant difference was demonstrated with regard to other postoperative complications, days to the commencement of a full ward diet and the length of hospital stay in both groups. More time (an average of 3.7 days) was spent in the intensive care unit and high care unit by those in the open appendectomy group, than those in the laparoscopic appendectomy group (an average of 2.0 days). However, age, duration of symptoms, clinical presentation and white blood cell count were influencing factors on the outcome measures in the open appendectomy group.
CONCLUSION: Generalised purulent peritonitis from complicated appendicitis can be managed successfully laparoscopically. Both approaches are feasible, safe and have comparable outcomes. The laparoscopic approach resulted in fewer postoperative wound sepsis complications
Keywords: complicated appendicitis, generalised purulent peritonitis, laparoscopic appendectomy, open appendectomy
Introduction
The laparoscopic appendectomy was first described by Semm in 1983.1 Since then, it has grown in popularity as a surgical option for the management of suspected or uncomplicated acute appendicitis. The benefits of various aspects of this approach over open surgery have been debated, with a reduction surgical site infection being the most consistent benefit.2 In South Africa, a midline laparotomy is considered the standard of management for patients with generalised purulent peritonitis from complicated appendicitis.3 However, a diagnosis of generalized purulent peritonitis is sometimes only made intraoperatively. Traditionally in these circumstances, the surgeon can elect to convert to a midline laparotomy or extend the original McBurney's point centered incision. Where the laparoscopic approach is used, the one can either convert or continue laparoscopically. Against this background, we compared the McBurney extension approach to the laparoscopic approach in a South African context.
Objectives
The main objectives of this study were to determine the role of a FAST as a screening tool in order to detect BAT in children who sustained HET, and whether or not it could replace CT scanning as a modality, given the limitations of the latter.
A secondary objective was to establish whether or not the combination of a FAST and a physical examination was adequate in detecting IAI.
Method
Study design and inclusion criteria
This study was conducted as a retrospective review of all cases with generalised purulent peritonitis from complicated acute appendicitis diagnosed intraoperatively at Sebokeng Hospital between January 2008 and December 2009. Generalised peritonitis was defined as a finding of purulent exudate at surgery, involving more than a single quadrant. Cases managed laparoscopically were compared to those managed via McBurney's initial incision, i.e. they were not converted to a midline laparotomy after the finding of generalised peritonitis, but rather the incision was extended. The decision to utilise either an open or a laparoscopic approach was made by the surgeon.
Exclusion criteria
Exclusion criteria included:
• All cases of generalised purulent peritonitis from other causes, except appendicitis.
• Cases of generalised purulent peritonitis which were managed via a midline laparotomy, or converted from McBurney's initial incision or Rocky-Davis incision to a midline laparotomy.
• Cases of patients with single, localised pus collection.
• All cases of patients with complicated appendicitis, i.e. appendiceal mass, gangrenous appendix or perforated appendix, without the presence of generalised purulent peritonitis.
Outcome measures
The main outcome measures for the purposes of this study were:
• The surgical approach, i.e. a laparoscopic appendectomy approach versus an open appendectomy approach.
• Theatre duration.
• Postoperative complications.
• The duration of stay in an intensive care unit (ICU) or high care unit (HCU).
• Time to the commencement of a full ward diet.
• Length of hospital stay.
Other measures included obtaining the demographic data, i.e. age, gender and duration of symptoms, prior to admission, and the clinical presentation of the patients, i.e. whether they presented with localised pain or generalised pain. These data were analysed.
Data analysis
The data were recorded in Microsoft® Excel® and comparisons between the groups made using SAS® version 9.1. Fisher's exact test was used when the number in a group was less than or equal to (<) 5. Multiple logistic regression was used to determine the theatre time, time taken to the commencement of a full ward diet, and time to discharge from the hospital. A p-value of < 0.050 was considered to be significant.
Results
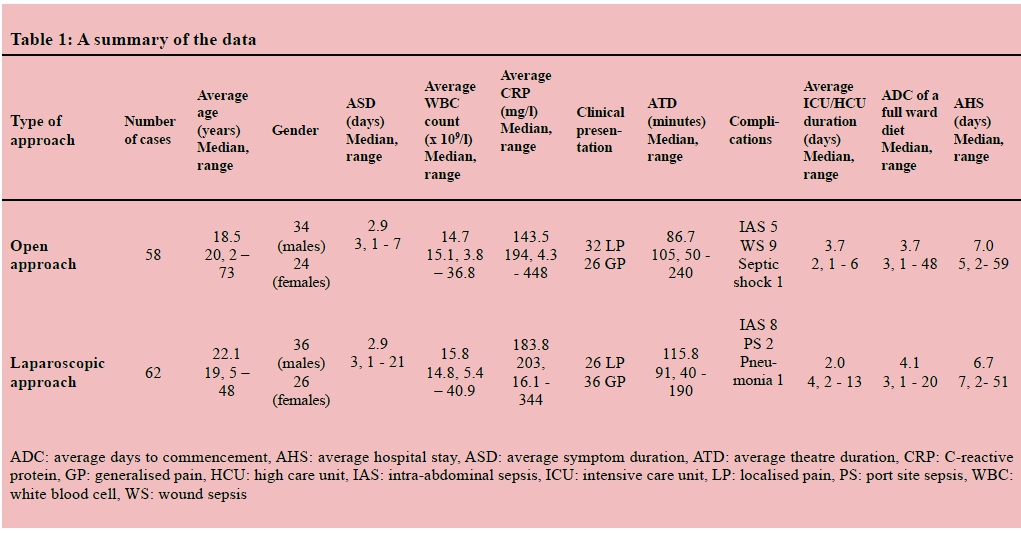
During the study period, a total of 120 cases of appendectomies with generalised purulent peritonitis were recorded. Of these, 58 cases underwent an open appendectomy and 62 cases a laparoscopic appendectomy. One case was converted from a laparoscopic approach to an open approach, constituting a conversion rate of 2%. Death did not occur in this study. The results of the open appendectomy and the laparoscopic appendectomy groups are summarised in Table 1.
Demographics and diagnostic evaluation
The study populations were comparable in both groups. The average age was 20 years, and most were males who presented at the hospital three days after the onset of the symptoms. There were no statistically significant differences with respect to age, gender, clinical presentation, duration of symptoms, WBC and CRP between the two groups (Table 2).
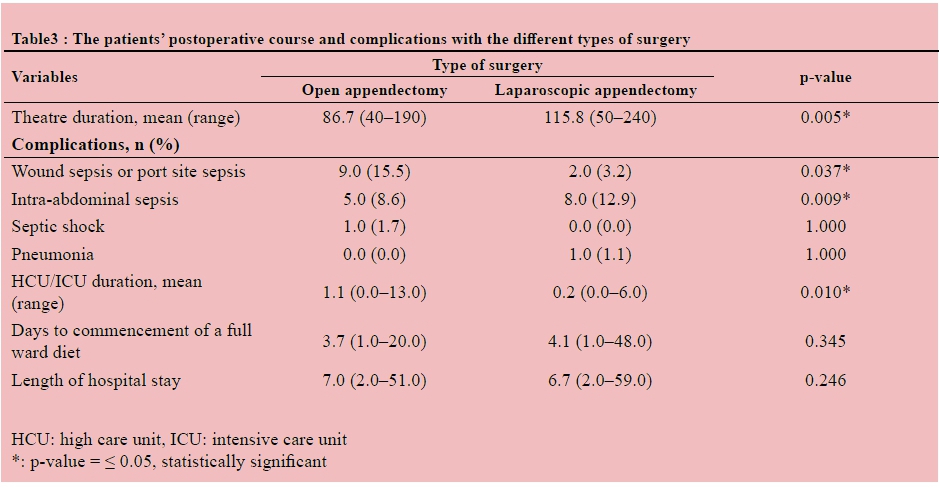
Outcome measures and complications
Table 3 shows the analysed outcomes variable for the two groups. The mean theatre duration was on average 30 minutes (p = 0.005) longer in the laparoscopic appendectomy group than in the open appendectomy group. The number of patients who developed wound/port site sepsis was significantly less in the laparoscopic appendectomy group than in the open appendectomy group (2/62 and 9/58 respectively, p = 0.037) The 5 cases (9%) of intra-abdominal sepsis (IAS) in the open appendectomy group and 8 cases (13%) in the laparoscopic appendectomy group were diagnosed by abdominal imaging. Of the 5 patients with IAS in the open appendectomy group, two were managed conservatively with intravenous antibiotics, one collection was drained rectally, and an exploratory laparotomy for drainage was required for the remaining two. However, of the eight patients with IAS in the laparoscopic appendectomy group, three were managed conservatively with intravenous antibiotics, four by laparoscopic drainage, and an exploratory laparotomy with a right hemicolectomy following caecal perforation was required for one patient. The clinical picture was the final arbiter in deciding whether the imaging shown IAS would be subjected to surgery.
A case of septic shock with renal failure was reported in the open appendectomy group, and a single case of pneumonia in the laparoscopic appendectomy group. Time to commencement of a full ward diet and the length of hospital stay were not different between the two groups.
Postoperative evaluation
Time to commencement of a full ward diet and the length of hospital stay were primary outcomes that were compared between the laparoscopic appendectomy and open appendectomy groups. The average times for both these outcomes were four and seven days, respectively. A significant difference was not noted between the groups (Table 3).
Although the average times to the commencement of full ward diet and length of hospital stay were not different, to determine whether more patients in either group commenced full ward diet or were discharged earlier, the data were re-analysed using Kaplan-Meier curves. No differences between the curves were noted for these parameters.
Discussion
General factors at presentation remain risk factors for outcome variables in appendicitis. The duration of symptoms was subdivided into early (<2 days) and late (>2 days). This was based on the study by Hayden et al. in which it was demonstrated that the risk of perforation increased to > 70% after 48 hours.4 The mean duration of symptoms was the same in both groups (2.9 days). This time reflects the delay in seeking medical assistance at a health institution. Based on the fact that 48% of the cases reported localised pain at their initial clinical presentation to the hospital, the intraoperative finding of generalised purulent peritonitis could not have been diagnosed with certainty on clinical presentation hence supporting a standard operative approach.
One case was converted from a laparoscopic approach to an open approach owing to technical difficulties as a result of grossly dilated loops of bowel (a conversion rate of 2%). It was shown in a literature review that conversion rates vary considerably from 1.7% to as high as 39%.5 The main reasons for conversion were poor visualisation, adhesions, and iatrogenic injury to the bowel and dilated loops of bowel.
The patients in the laparoscopic appendectomy group spent approximately 30 minutes longer in theatre than their open appendectomy counterparts, which is in keeping with the findings of other similar studies in the literature.5-7 Unlike the other studies, theatre duration (the time from when the patient was taken into theatre to the time that he or she was removed) was considered in this study. It was shown in a review of the literature with regard to a meta-analysis of laparoscopic versus open appendectomy for acute appendicitis, that the theatre time was calculated from the time of incision to the time of wound closure in most studies. However, Tate et al.8 used the time from induction to the time of reversal. In uncomplicated appendicitis, as in this study, Minne et al.9 recorded the total time spent in the operating theatre. Their results for median operating time were 82 minutes for the laparoscopic group, and 67 minutes for the open group. This was shorter than in this study which dealt with complicated appendicitis with peritonitis in whom peritoneal toilet added to the total time for theater.
An increase in the intra-abdominal sepsis (IAS) rate following the laparoscopic approach, especially for perforated appendicitis, has been documented in studies.9,10 Consequently, an open approach has been advocated. However, in a study by Katkhouda et al.6 on intra-abdominal sepsis rates after laparoscopic appendectomy, 645 cases of acute appendicitis were reviewed, of which 67 were perforated and 61 gangrenous. They were able to show that the IAS rate following laparoscopic appendectomy for perforated appendicitis was significantly lower that what had been reported in the literature. The findings of the present study indicated that laparoscopic appendectomy for purulent peritonitis from complicated appendicitis was associated with a statistically significant higher incidence of IAS of 13%, as opposed to 9% in the open appendectomy group (p = 0.009). However, in terms of management, the majority did not require an open surgical procedure and could be managed laparoscopically. The increase in intra-abdominal sepsis in the laparoscopic appendectomy group may be due to bacterial translocation caused by carbon dioxide pneumoperitoneum. Bloechle et al.11 in a rat model of gastric perforation, found a significant increase in the degree of peritonitis in the pneumoperitoneum group, compared to that in the control group. The results conflict with another rat's study where intraperitoneal fecal inoculums, resulted in a higher number of IAS compared with rats that underwent laparoscopy.12 There are several studies which attest to equivalent rates of IAS in open and advanced cases. 13,14
The wound sepsis rate was 4 times higher in the open appendectomy group, with only 2 cases (3%) of port site sepsis in the laparoscopic appendectomy group. One of the reasons for the lower incidence of port site sepsis in the laparoscopic appendectomy group was that the inflamed appendix was removed through the operating port without making contact with the wound itself otherwise a plastic bag extraction was used. This is a consistent finding in the laparoscopic versus open appendectomy meta-analysis. 2,5,7,10,13,15
One case of septic shock with renal failure occurred in the open appendectomy group. The patient in question spent a long time in ICU, and required haemodialysis for renal failure. He ultimately recovered and was subsequently discharged. A single case of pneumonia occurred in the laparoscopic appendectomy group as a result of complications. An uneventful course was also reported.
As far as can be determined, the influence of age, gender, duration of symptoms prior to admission, WBC count and CRP on outcome measures when comparing open appendectomy and laparoscopic appendectomy has not been established in any other study. The outcome measures of an open appendectomy depended on several factors in this study; age, the duration of symptoms, clinical presentation and the patient's WBC count. However, the outcome measures of a laparoscopic appendectomy were influenced only by the patient's age and the CRP.
The intrinsic weakness of a retrospective study is acknowledged. The results of the subgroup analyses should be interpreted with caution. The shortcomings of the current study were reflected by lack of defined selection criteria for the operative approach for complicated appendicitis. Selection bias cannot be excluded in the present study. In 2008, the surgical department of Sebokeng Hospital adopted a policy of laparoscopic appendectomy in all patients who presented to the emergency room with signs and symptoms of acute appendicitis. However, it is the decision of the surgical team on call, rather than the preoperative signs, operative findings and surgeon's technical skills (consultants are readily available) that determines the type of operative procedure. The sample size was another limitation in this study. However, this is a problem shared by every other trial analysed. Considering that conventional appendectomy is already a simple and minimally invasive operation with low morbidity and near-zero mortality, any possible improvement would only be modest. Therefore, the trial size should be appropriately large to detect an advantage beyond reasonable doubt, if any doubt exists.
Conclusion
The intrinsic weakness of a retrospective study is acknowledged. The shortcomings of the current study by the potential selection bias in a lack of standardised criteria for the choice of operative approach for complicated appendicitis. However, the study does show in selected patients that continuing a laparoscopic approach when peritonitis is observed is safe when compared to using local extension of the initial open incision. The approach comes at the cost of increased operating time and more IAS but it is offset by a fourfold lower wound infection rate.
REFERENCES
1. Semm K. Endoscopic appendectomy. Endoscopy. 1983;15(2):59-64. [ Links ]
2. Ohtani H, Tamamori Y, Arimoto Y, Nishiguchi Y, Maeda K, Hirakawa K. Meta-analysis of the results of randomized controlled trials that compared laparoscopic and open surgery for acute appendicitis. J Gastrointest Surg. 2012. doi:10.1007/s11605-012-1972-9 [ Links ]
3. Kong VY, Bulajic B, Allorto NL, Handley J, Clarke DL. Acute appendicitis in a developing country. World J Surg. September 2012;36(9):2068-73. doi: 10.1007/s00268-012-1626-9 [ Links ]
4. Hayden GE, Russell WS, Park DB, Presley BC. Perforated appendicitis diagnosed at the bedside. J Emerg Med. September 2014;47(3): e85-8. [ Links ]
5. Mancini GJ, Mancini ML, Nelson HS Jr. Efficacy of laparoscopic appendectomy in appendicitis with peritonitis. Am Surg. 2005;71:1-4. [ Links ]
6. Katkhouda N, Friedlander MH, Grant SW, et al. Intraabdominal abscess rate after laparoscopic appendectomy. Am J Surg. 2000;180(6):456-461. [ Links ]
7. Asarias JR, Schlussel AT, Cafasso DE, Carlson TL, Kasprenski MC, Washington EN, et al. Incidence of postoperative intraabdominal abscesses in open versus laparoscopic appendectomies. Surg Endosc. 2011;25:2678-2683. [ Links ]
8. Tate JT, Dawson JW, Chung SC, Li AK. Laparoscopic versus open appendectomy: prospective randomised trial. Lancet September 1993;342(8872):633-637. [ Links ]
9. Minne L, Varner D, Burnell A. Laparoscopic versus open appendectomy: prospective randomised study of outcomes. Arch Surg. 1997;132(6):708-712. [ Links ]
10. Martin LC, Puente I, Sosa JL, et al. Open versus laparoscopic appendectomy: a prospective randomised comparison. Ann Surg. 1995;222(3):256-262. [ Links ]
11. Bloechle C, Emmermann, Treu H. Effect of pneumoperitoneum on the extent and severity of peritonitis induced by gastric ulcer perforation in rats. Surg Endosc. 1995;9(8):898-901. [ Links ]
12. Jacobi CA, Ordemann J, Bohm B. Does laparoscopy increase bacteremia and endotoxemia in peritonitis model? Surg Endosc. 1997;11(6):235-238. [ Links ]
13. Raphael SC, Douglas YR, Li P, Diaz J. A meta-analysis of randomized controlled trial of laparoscopic versus conventional appendectomy. Am J Surg. 1999;177(5):250-256. [ Links ]
14. Penninga L, Gluud C, Wetterslev J. Meta-analysis of randomised trials on laparoscopic versus open surgery for acute appendicitis: has firm evidence been reached? J Gastrointest Surg. July 2014;18(7):1383-4. [ Links ]
15. Lin YM, Hsieh CH, Cheng CI, Tan BL, Liu HT. Laparoscopic appendectomy for complicated acute appendicitis does not result in increased surgical complications. Asian J Surg. 2012; 35:113-116. [ Links ]
 Correspondence:
Correspondence:
Brown Ndofor
brown@ndofor.com


{kind=link}
{kind=link}
{kind=link}