










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.54 n.3 Cape Town Sep. 2016
GENERAL SURGERY
Severe post-pancreatoduodenectomy haemorrhage: An analytical review based on 118 consecutive pancreatoduodenectomy patients in a South African Academic Hospital
M M BernonI, IV; J E J KrigeI, IV; E JonasI, IV; J C KloppersI; S BurmeisterI, IV; N G NaidooII; S J BeningfieldIII, IV
IHPB Surgical Unit
IIHPB Vascular Unit
IIIDepartment of Surgery and Department of Radiology
IVUniversity of Cape Town Health Sciences Faculty, Groote Schuur Hospital and Netcare University of Cape Town Private Academic Hospital
ABSTRACT
BACKGROUND: Bleeding after a major pancreatic resection, although uncommon, has serious implications and substantial mortality rates.
AIM: To analyse our experience with severe post-pancreatoduodenectomy haemorrhage (PPH) over the last 7 years to establish the incidence, causes, intervention required and outcome.
METHODS: All patients who underwent a pancreatoduodenectomy (PD) between January 2008 and December 2015 were identified from a prospectively maintained database. Data analysed included demographic information, operative details, anastomotic technique, histology, postoperative complications including pancreatic fistula and PPH, length of hospital stay, need for blood products and special investigations. Pancreatic fistula was classified according to the International Study Group of Pancreatic Surgery (ISGPS) classification. A modified ISGPS classification was used for PPH.
RESULTS: One hundred and eighteen patients underwent PD during the study period of whom 6 (5.0%) died perioperatively. Twenty patients (16.9%) developed a pancreatic fistula and 11 patients (9.3%) had a severe PPH of whom one (9.1%) died. No patients had a severe bleed during the first 24 hours postoperatively. Four patients bled within the first 5 days and the remaining 7 after five days. Six patients bled from the gastroduodenal artery and were all preceded by a pancreatic fistula. Three of the 7 patients who bled late presented with extraluminal bleeding, 3 presented with intraluminal bleeding and 1 with a combination of both. Patients presenting in the first 5 days were all successfully managed either endoscopically or surgically. Five patients who presented beyond 5 days postoperatively were managed primarily with interventional angiography, either with coiling or deployment of a covered stent. Three patients who had radiological intervention developed a liver abscess or necrosis.
CONCLUSION: Severe PPH is associated with substantial morbidity. Clinical factors including the onset of the bleeding, presentation with either extra and/or intraluminal haemorrhage, and the presence of a pancreatic fistula give an indication of the likely aetiology of the bleeding. A management algorithm based on these factors is presented.
Key words: Pancreatoduodenectomy, bleeding, postoperative
Introduction
The mortality rate following pancreatoduodenectomy (PD) has decreased substantially in most high volume centres over the past decade and is now less than 5%. However, surgical morbidity remains high - estimated to be between 20% and 40% - and includes pancreatic and bile leaks, delayed gastric emptying and infected intra-abdominal collections. Post-pancreatoduodenectomy haemorrhage (PPH) is a less frequent but serious complication that can result in significant morbidity and mortality, especially if further surgery is required for management. PPH early after the index operation may be arterial, usually from the uncinate process resection margin close to the superior mesenteric artery or venous from portal vein branches or from one of the 3 anastomoses. Common causes of delayed PPH include mucosal ulceration (commonly at the gastro-enteric anastomosis), or erosion of peri-pancreatic vessels (commonly the gastro-duodenal artery (GDA) stump or common hepatic artery). The latter is usually the result of a pancreatic leak eroding the vessel, causing a pseudoaneurysm and resultant haemorrhage.1
PPH has been classified by the International Study Group of Pancreatic Surgery (ISPGS) into three grades according to onset, site, severity and clinical consequences.2,3 Surgery is the recommended initial treatment for haemorrhage within 24 hours. In contrast, endovascular control of PPH has been shown to have a better rate of success with lower morbidity and mortality for delayed PPH. Several factors have been shown to predispose to late PPH including intra-abdominal infection, a pancreatic fistula or a bile leak. The early diagnosis and prompt treatment of PPH is essential to reduce the mortality rate.49
The aim of this study was to determine the incidence, presentation and management of PPH in a recent series of PD and to better define the roles of operative compared to angiographic intervention.
Methods
Data were obtained from a prospective database of all patients who underwent a PD between January 2008 and December 2015 in Groote Schuur Hospital and the Netcare University of Cape Town Private Academic Hospital. Patients undergoing other pancreatic operations including tumour enucleation, distal or total pancreatectomy and resections for trauma were excluded from the study. Information collected included demographic data, details of anastomotic technique, histology of the resected specimen, postoperative complications, the time interval between PD and PPH, the source of haemorrhage, treatment strategy, need for blood products, hospital stay and clinical outcome.
Definitions
Postoperative pancreatic fistula (POPF) was defined according to the ISPGS pancreatic fistula classification as any measurable volume of fluid on or after postoperative day 3 with an amylase content greater than 3 times the serum amylase level.10 For PPH a modified definition of the ISGPS classification was used, dividing the onset of bleeding into early, intermediate and late as defined in Table 1.
Surgical procedure
The resection of choice was a standard pylorus-preserving pancreatoduodenectomy (PPPD). A classic Whipple resection was performed when necessary. The GDA stump was suture ligated with 3/0 Prolene®. When separation of the tumour from the superior mesenteric vein or the portal vein was not feasible, venous resection was performed to obtain complete tumour resection with macroscopic clear surgical margins. For reconstruction after tangential resections, portal venorrhaphy was performed or, when required, a xenopericardial patch was used. For reconstruction after resection of a segment of portal vein, a primary end-to-end anastomosis was performed or, when needed, a reversed autologous internal jugular vein interposition. Completion anastomoses were by means of end-to-side, duct-to-mucosa pancreaticojejunostomy (PJ) or pancreatogastrostomy (PG), end-to-side hepaticojejunostomy (HJ) and duodenojejunostomy (DJ) or gastrojejunostomy (GJ). Silicone suction drains were routinely placed near the PJ and HJ. Patients were transferred to a high care unit after the procedure with thromboprophylaxis commenced 8 hours after surgery. The amylase level of drain fluid was analysed 72 hours after the surgery.
Investigation of and intervention for PPH
In patients with PPH, investigations were dictated by a modified classification system based on the time of onset, presentation and severity (Table 1). Our policy was that patients with severe early bleeding underwent surgical exploration, whereas those with severe intermediate or late bleeding had either endoscopy or angiography depending on the most likely source of bleeding. Intraluminal sources of bleeding, identified during endoscopy were managed endoscopically, when amenable. Haemorrhage or pseudo-aneurysms identified angiographically were controlled by trans-catheter coil embolization or covered stent grafts.
Results
Patient characteristics
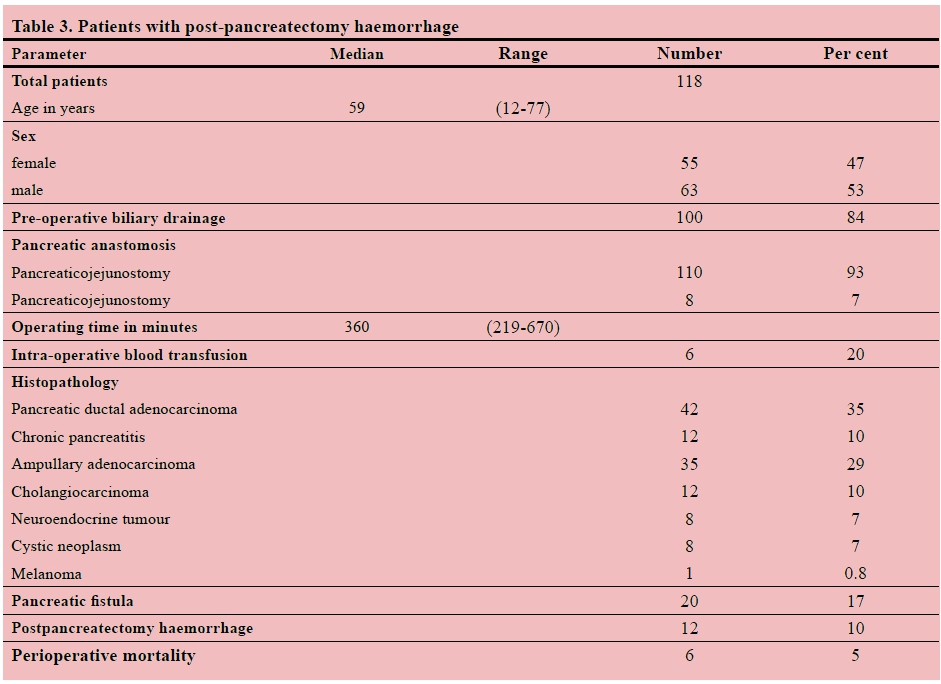
One hundred and eighteen patients underwent PD between January 2008 and December 2015 of whom 6 (5.0%) died within 30 days and 60 (50.8%) had a postoperative complication (Table 2). The most common complication was wound sepsis (n = 29, 24.6%), while 20 patients (16.9%) developed a pancreatic fistula according to the ISPGS definition. Six patients (5.1%) developed infected intra-abdominal collections and 5 patients (4.2%) manifested a bile leak.
Post pancreatoduodenectomy haemorrhage
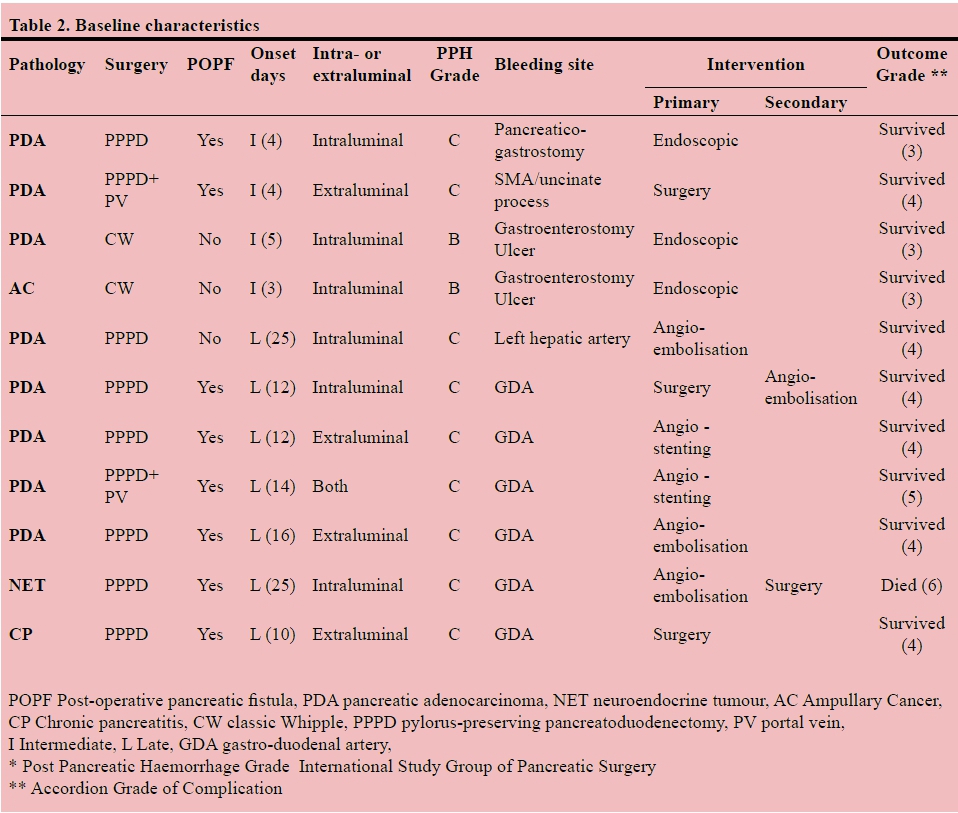
Eleven patients (9.3%) developed severe PPH, none of which occurred early (Table 3). The most common source of PPH was the GDA stump, seen in six patients (54.5%). In two patients, the source was a submucosal vessel at the GE. One patient bled from the PG, another from the uncinate branch of the superior mesenteric artery (SMA) and a third patient bled from the left hepatic artery.
Four patients (36.4%) bled during the intermediate period, while the remaining 7 (63.6%) presented late, of which one patient died (Table 3). The source of the late bleeds was the GDA in 6 patients and the left hepatic artery in one. All the late bleeds were associated with a POPF, with a median presentation at 12 days (range 10-25 days). In this group of patients, 3 presented with extraluminal haemorrhage, 3 with intraluminal haemorrhage and 1 with both intra- and extraluminal haemorrhage.
Intervention
The three patients who presented intermediately with intraluminal haemorrhage were all successfully managed endoscopically. The endoscopic interventions included adrenaline injection, electro-cautery with a Gold probe® and haemostatic clips. One patient in this group presented with extraluminal haemorrhage from the uncinate branches of the SMA and required re-operation and suture ligation of the artery. Five of the 7 patients (71.4%) who presented late were managed primarily with radiological intervention and two (28.6%) surgically. One patient who was haemodynamically unstable and in whom angiography was not immediately available, was managed operatively. In the other, attempted surgical control of the haemorrhage failed and haemostasis was achieved with a subsequent embolization of the GDA stump.
Primary radiological intervention was performed in 5 patients with complete haemostasis achieved in 4. A covered stent was used in two patients. One patient in whom surgical control was necessary subsequently died from multi-organ failure. Two of the four patients treated by embolization developed focal liver abscesses and necrosis. One patient who underwent left hepatic artery angiography and coil embolization developed ischaemic cholangiopathy. One of the patients treated with a covered stent developed a liver abscess. This patient had undergone portal vein resection and developed postoperative portal vein thrombosis prior to stenting.
Discussion
Although severe PPH is an uncommon postoperative complication after PD, there is a 17-fold increase in mortality, approaching 50% in some reports. The diagnostic modality of choice and subsequent method of intervention are dictated by the time of onset and presentation. The differentiation of PPH into early, intermediate and late is helpful as this distinction influences management and predicts outcome. Although early haemorrhage is usually due to technical haemostatic factors, none occurred in this study. Intermediate bleeds were due to ulcers, anastomotic bleeds or bleeding from the resection bed, whereas all late bleeds were arterial and associated with a POPF. Angiographic intervention achieved control of bleeding in 80% of patients. Early PPH, as opposed to late, has been reported as having a better prognosis. In this study the overall mortality of patients with severe bleeding (9.1%) was lower than in previous reports. In the pre-angiographic intervention era, late PPH was treated by re-operation and attempted ligation or suturing of the bleeding vessel, which can be difficult due to dense inter-loop adhesions, the overlying jejunum, immature anastomoses and vessel wall friability.11-13
Recent advances in interventional radiological techniques and new generation guidewires and micro-catheters facilitate access to individual vessels and treatment by accurate coiling and stenting, avoiding the morbidity of surgery. The major limitations of embolization are re-bleeding due to incomplete vascular occlusion or coil migration, complications related to subsequent ischaemia with liver necrosis and abscess formation and/or biliary ischemia. To avoid these severe complications, covered stents have been used to maintain perfusion, which is particularly important in patients at risk of portal vein thrombosis. However, vessel kinking and anatomical variations may preclude placement of the bulkier and more rigid stent delivery system.14-17
Based on our revised classification and the findings of this study we propose an algorithm for the treatment of severe PPH (Figure 1). Patients with early haemorrhage should have an urgent re-operation. In patients with intermediate presentation, the investigation of choice depends on the presentation (intra- versus extraluminal). Patients with an intraluminal bleed should undergo an endoscopy and if the source is identified, endoscopic treatment should be attempted. If the source is not identified, angiography should be considered. If endoscopic treatment fails, surgical or angiographic intervention would be the next step. Patients presenting with extraluminal bleeds should undergo angiography and if the source is identified, angiographic intervention should be performed. Patients with a late PPH should undergo angiography and angiographic treatment. Surgery is indicated if angiography does not establish the source or if angiographic treatment fails.

In conclusion, while severe PPH is encountered relatively infrequently, it remains a serious complication with a significant mortality. We propose that patients should be classified into three distinct groups based on the time of onset of bleeding, and suggest a pragmatic treatment algorithm based on the most likely source of bleeding to guide the choice of diagnostic and therapeutic modalities.
REFERENCES
1. Pugalenthi A, Protic M, Gonen M, et al. Postoperative complications and overall survival after pancreaticoduodenectomy for pancreatic ductal adenocarcinoma. J Surg Oncol. 2016;113(2):188-193. http://dx.doi.org/10.1002/jso.24125 [ Links ]
2. Wente MN, Veit JA, Bassi C, et al. Postpancreatectomy hemorrhage (PPH): An international study group of pancreatic surgery (ISGPS) definition. Surg. 2007;142(1):20-25. http://dx.doi.org/10.1016/j.surg.2007.02.001 [ Links ]
3. Grutzmann R, Ruckert F, Hippe-Davies N, Distler M, Saeger HD. Evaluation of the international study group of pancreatic surgery definition of post-pancreatectomy hemorrhage in a high-volume center. Surg. 2012;151(4):612-620. http://dx.doi.org/10.1016/j.surg.2011.09.039 [ Links ]
4. Yekebas EF, Wolfram L, Cataldegirmen G, et al. Postpancreatectomy hemorrhage: Diagnosis and treatment: An analysis in 1669 consecutive pancreatic resections. Ann Surg. 2007;246(2):269-280. http://dx.doi.org/10.1097/01.sla.0000262953.77735.db [ Links ]
5. Asari S, Matsumoto I, Toyama H, et al. Recommendation of treatment strategy for postpancreatectomy hemorrhage: Lessons from a single-center experience in 35 patients. Pancreatol. 2016;16(3):454-463. http://dx.doi.org/10.1016/j.pan.2016.02.003 [ Links ]
6. Wellner UF, Kulemann B, Lapshyn H, et al. Postpancreatectomy hemorrhage--incidence, treatment, and risk factors in over 1,000 pancreatic resections. J Gastrointest Surg. 2014;18(3):464-475. http://dx.doi.org/10.1007/s11605-013-2437-5 [ Links ]
7. Roulin D, Cerantola Y, Demartines N, Schafer M. Systematic review of delayed postoperative hemorrhage after pancreatic resection. J Gastrointest Surg. 2011;15(6):1055-1062. http://dx.doi.org/10.1007/s11605-011-1427-8 [ Links ]
8. Choi SH, Moon HJ, Heo JS, Joh JW, Kim YI. Delayed hemorrhage after pancreaticoduodenectomy. J Am Coll Surg. 2004;199(2):186-191. [ Links ]
9. Sanjay P, Fawzi A, Fulke JL, et al. Late post pancreatectomy haemorrhage. risk factors and modern management. JOP. 2010;11(3):220-225. [ Links ]
10. Bassi C, Dervenis C, Butturini G, et al. Postoperative pancreatic fistula: An international study group (ISGPF) definition. Surg. 2005;138(1):8-13. http://dx.doi.org/10.1016/j.surg.2005.05.001 [ Links ]
11. van Berge Henegouwen MI, Allema JH, van Gulik TM, Verbeek PC, Obertop H, Gouma DJ. Delayed massive haemorrhage after pancreatic and biliary surgery. Br J Surg. 1995;82(11):1527-1531. http://dx.doi.org/10.1002/bjs.1800821124 [ Links ]
12. Blanc T, Cortes A, Goere D, et al. Hemorrhage after pancreaticoduodenectomy: When is surgery still indicated? Am J Surg. 2007;194(1):3-9. http://dx.doi.org/10.1016/j.amjsurg.2006.08.088 [ Links ]
13. Ellison EC. Evidence-based management of hemorrhage after pancreaticoduodenectomy. Am J Surg. 2007;194(1):10-12. http://dx.doi.org/10.1016/j.amjsurg.2006.12.034 [ Links ]
14. Mansueto G, D'Onofrio M, Iacono C, Rozzanigo U, Serio G, Procacci C. Gastroduodenal artery stump haemorrhage following pylorus-sparing whipple procedure: Treatment with covered stents. Dig Surg. 2002;19(3):237-240. http://dx.doi.org/10.1159/000064219 [ Links ]
15. Huo Y, Chi J, Zhang J, et al. Endovascular intervention for delayed post-pancreaticoduodenectomy hemorrhage: Clinical features and outcomes of transcatheter arterial embolization and covered stent placement. Int J Clin Exp Med. 2015;8(5):7457- 7466. [ Links ]
16. Khalsa BS, Imagawa DK, Chen JI, Dermirjian AN, Yim DB, Findeiss LK. Evolution in the treatment of delayed postpancreatectomy hemorrhage: Surgery to interventional radiology. Pancreas. 2015;44(6):953-958. http://dx.doi.org/10.1097/MPA.0000000000000347 [ Links ]
17. Asai K, Zaydfudim V, Truty M, et al. Management of a delayed post-pancreatoduodenectomy haemorrhage using endovascular techniques. HPB (Oxford). 2015;17(10):902-908. http://dx.doi.org/10.1111/hpb.12464 [ Links ]
 Correspondence:
Correspondence:
MM Bernon
marcbernon@mail.com


{kind=link}
{kind=link}
{kind=link}