










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.54 n.3 Cape Town Sep. 2016
GENERAL SURGERY
Laparoscopic management of hydatid cyst of the liver
Y YağmurI; S AkbulutII; S GümüşIII; M BabürIII; M A CanIII
IProfessor and Chief of Surgery, University of Health Sciences Diyarbakir Gazi Yasargil Teaching and Research Hospital
IIAssistant Professor, Department of Surgery, Inönü University Malatya
IIIResident, Department of Surgery University of Health Sciences Diyarbakir Gazi Yasargil Teaching and Research Hospital
ABSTRACT
BACKGROUND: Hydatid liver disease management has evolved from traditional operative approaches to the increasing application of laparoscopic treatments. We aimed to prospectively assess the early outcomes of laparoscopic treatment at our institution.
PATIENTS AND METHODS: Forty-four patients with hydatid disease of liver were screened with ultrasonography and computed tomography of the abdomen to exclude Gharbi type V cysts. The distribution of cyst sizes was: 1-4 cm, 10; 5-10 cm, 24; 10-15 cm, 8; > 15 cm, 2 patients. The following laparoscopy therapies were performed: 30 patients had cystectomy alone, 14 patients had partial pericystectomy. Pericystectomy was performed using a hook and harmonic tissue sealers with the resection made through normal liver tissue.
RESULTS: Three patients were converted to open surgery. Seven patients had biliary leakage through their cystic cavity drains. Five stopped spontaneously by the 7th postoperative day and 2 responded to ERCP sphincterotomy. There were no deaths and no recurrence of disease noted by 6 months
CONCLUSION: In selected patients with hepatic hydatid disease, a laparoscopic treatment is feasible and safe with low conversion rate and short term recurrences.
Key words: Hydatid cyst of liver, laparoscopic treatment
Introduction
Hydatid disease, a zoonotic disease caused by Echinococcus. spp of helminths. E. granulosus, is the commonest cause of cystic hydatidosis, a disease which continues to be a serious public problem causing morbidity and mortality in China, Eastern Europe, Turkey, the Far East and South Africa.1,2 Hydatid cysts may develop in any organ of the body, but occur most frequently in the liver (50-80%) and lung (15-47%), occasionally in the spleen, kidney, pancreas and intraperitoneal space, and infrequently at other sites.2-13
The traditional operative approach is an open surgical one to drain the cysts and remove their germinal layer by either controlled evacuation of the cystic cavity or resectional surgery. Since the first laparoscopic treatment of hydatid disease was described in 1992,14 there has been a steady growth in reports of the laparoscopic treatment of hydatid cysts of liver. Although early reported laparoscopic treatment of liver hydatid disease was confined to simple drainage, more advanced laparoscopic methods are now possible, including pericystectomy and hepatic resection.1
The purpose of this study was to analyse the safety and early outcomes of laparoscopic treatment of liver hydatid cysts at our institution.
Patients and methods
Forty-four patients diagnosed with hydatid cysts of liver had laparoscopic treatment at Diyarbakir Gazi Yas.argil Education and Research Hospital between 2013 and 2014. Fourteen patients were male and 30 were female. Their age ranged from 16 to 71 years. Indirect haemagglutination tests were performed in 20 patients and were elevated in 18. Initial evaluation was by ultrasonography and computed tomography of the abdomen. Patients with Gharbi type V hydatid cysts were excluded from the study. The cyst diameter ranged from 4 to 16 cm. The distribution of mean cyst diameter was as follows: 1-4 cm (10 patients); 5-10 cm (24); 10-15 cm (8); > 15 cm (2). The distribution of cysts to liver segment was as follows: segment 2 (2); segment 3 (6), segment 4 (12), segment 5 (6), segment 6 (6), segment 7 (20) and segment 8 (6). Fourteen patients had multiple cysts. Patients were treated with albendazole 10 mg/kg/day for at least 2 weeks preoperatively and continued postoperatively for 4 weeks. The diagnosis of hydatid disease was confirmed by postoperative histological examination.
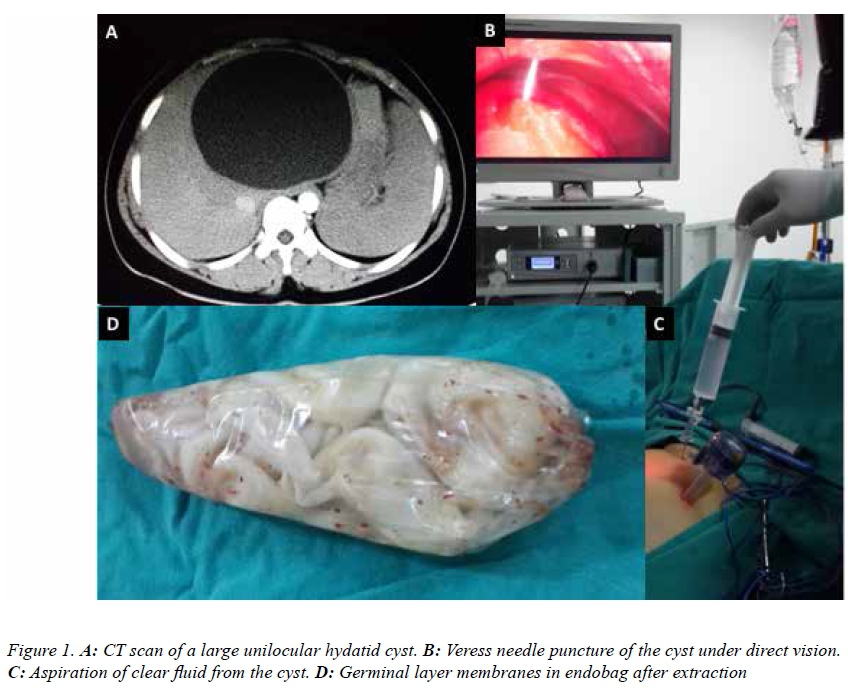
The pneumoperitoneum was achieved through a 10 mm trocar placed in the umbilicus which served as the optical port for a 30 degree telescope. Other port sites were varied according to the cyst location but were usually placed in the epigastrium (10 mm) and in the midclavicular line and anterior axillary lines (5 mm). After locating the cyst it was packed off with 10% povidone iodine as a scolicidal agent to reduce the risk of intraperitoneal seeding caused by accidental spillage. The Veress needle was introduced through subcostal margin into the cyst, with care taken not to injure the diaphragm and cause a pneumothorax. The content of the cyst was aspirated and the cavity was filled with povidone iodine for 10 minutes to ensure the death of all viable scolices. The cyst was then opened with the hook dissector and the content of the cyst including pericyst were aspirated and dissected free. The germinal membranes were put into an endobag and removed. The cyst cavity was cleaned with normal saline solution prior to inspection to ensure complete germinal membrane removal and to identify any bile leaks. When necessary, partial resection of the pericyst was performed through normal liver tissue with the harmonic scalpel®. A Foley catheter was put into the cyst cavity for drainage and another was put into the subhepatic place through a 5 mm trocar.
Results
Three patients were converted to open laparotomy due to restricted access for safe isolation. Thirty patients had cystectomy alone, and 14 patients had a partial pericystectomy. Five patients had an omentoplasty to fill the cavity. The median operation time was 90 minutes, range (60-190 minutes). The mean hospital stay was 3 days (range 2-10 days). Seven patients had biliary leakage through their cystic cavity drains. Five stopped spontaneously by the 7th postoperative day. In 2 patients, endoscopic retrograde cholangiopancreatography (ERCP) and sphincterotomy were performed and biliary leakage ceased after 48 hours. There were no deaths. Ultrasonography and an indirect haemagglutinin test were performed at the 6-month follow-up. The titers returned to normal in patients who presented with elevated titers, and no recurrence of the disease was observed.
Discussion
Laparoscopic treatment of liver hydatid cystic disease has gained ground despite initial exaggerated fear of complications such as anaphylaxis. The techniques applied at open surgery can all be performed laparoscopically and include puncture and aspiration, marsupialization, unroofing and drainage, unroofing and omentoplasty, partial and complete pericystectomy.15 Tuxan et al. reviewed the world literature on laparoscopic treatment of liver hydatid cyst.1 They reported on data from 57 published articles with a total of 914 patients who had 1116 hydatid cysts. Eighty-nine per cent were completed laparoscopically. The most common procedure was cystectomy (60%), followed by partial pericystectomy (15%) and pericystectomy (8%). The rest were segmental liver resections. Conversion to open laparotomy occurred in 45 patients (5%) predominantly due to anatomical inaccessibility of the cyst. The morbidity was 15%, with the most common complication being bile leakage (6%). There were no intraoperative deaths with two in-hospital deaths reported (0.22%). They concluded that the laparoscopic approach is safe with an acceptable mortality and morbidity for both conservative and radical resections in selected patients. These findings are generally in keeping with those from our study except that our bile leakage rate was 16%. Despite this fairly high rate, most settled spontaneously and those who did not responded well to sphincterotomy.
Ramia et al.16 reported 37 patients with hydatid diseases of whom one third underwent more radical resective procedures - 12 left lateral sectionectomies and 4 formal liver resections. Their median operating time was 185 minutes, which was twice as long as in this study, attesting to the magnitude of the surgery. Their conversion rate of 8% was similar to ours as was their zero cyst recurrence rate. Their longer follow-up of 30.6 months attests to the durability of this cure, which we observed in the short term.
One early concern was whether the laparoscopic approach would result in an increased incidence of intraoperative spillage, particularly in laparoscopic cystectomy. When laparoscopic surgery, both conservative and radical, is performed for hydatid cysts, there must be no compromise in the principle of avoiding cyst content spillage and maintaining the integrity of the cyst wall. During laparoscopic treatment, one of the problems is difficulty in evacuation of cyst content, the daughter cysts and laminated membrane.
Several laparoscopic systems have been devised to minimize the spillage of hydatid fluid and facilitate evacuation.1718 Palanivelu described a new special trocar-cannula device for laparoscopic management of hepatic hydatid disease. The device allows complete evacuation of the cysts and its contents and facilitates intracystic inspection. The innovators who designed this device reported on its use in 105 patients with a 14% bile leak rate and recurrences in only 2 patients after 36 months.19 A perforator-grinder aspirator apparatus for evacuation of the hydatid cyst has also been described by Saglam.20 Zain Al-Shareef et al.21 treated 10 patients with hepatic hydatid cysts laparoscopically using a liposuction device for aspiration of cyst content. He also utilized the same betadine scolicidal method of partial aspiration of cyst fluid and replacement that we used in our study.
We believe that these devices are likely to be more useful in the very large complex multilocular cysts which are under extreme pressure than in the less complex smaller cysts where scolicidal methods provide sufficient protection.
We have shown in this series that not only simple hepatic hydatid cysts but an array of intermediate size complex cysts can be safely managed laparoscopically with a high technical success rate, a low recurrence rate and an acceptable biliary fistula rate which did not require repeat surgery.
REFERENCES
1. Tuxun T, Zhang JH, Zhao JM, Tai QW, Abudurexti M, Ma HZ, et al. World review of laparoscopic treatment of liver cystic echinococcosis -914 patients. Int J Infect Dis. July 2014;24C:43-50. Review Epub 16 April 2014. doi:10.1016/j.ijid.2014.01.012 [ Links ]
2. Yagmur Y, Akbulut S. Unusual location of hydatid cysts: a case report and literature review. Int Surg. January-March 2012;97(1):23-6. [ Links ]
3. Akbulut S, Senol A, Ekin A, Bakir S, Bayan K, Dursun M. Primary retroperitoneal hydatid cyst: report of 2 cases and review of 41 published cases. Int Surg 2010;95(3):189-196. [ Links ]
4. Akbulut S, Senol A, Sezgin A, Cakabay B, Dursun M, Satici O. Radical vs. conservative surgery for hydatid liver cysts: Experience from single center. W J Gastroenterol. 2010;16(8): 953-959. [ Links ]
5. Yang G, Wang X, Mao Y, Liu W. Case report of primary retroperitoneal hydatid cyst. Parasitol Int. 2011;60(3):333-334. [ Links ]
6. Unalp HR, Kamer E, Rezanko T, Kilic O, Tunakan M, Onal MA. Primary hydatid cyst of the axillary region: a case report. Balkan Med J. 2011;28(2):209-211. [ Links ]
7. Yeola-Pate M, Banode PJ, Bhole AM, Golhar KB, Shahapurkar VV, Joharapurkar SR. Different locations of hydatid cysts: Case illustrations and literature review. Infect Dis Clin Pract. 2008;16(6):379Y384. [ Links ]
8. Borovik A, Massasso D, Gibson K. Axillary hydatid disease. MJA 2006;184(11):585. [ Links ]
9. Losanoff JE, Richman BW, Jones JW. Primary hydatid cyst of the axilla. ANZ J Surg. 2004;74(5):393-394. [ Links ]
10. Dilege S, Aksoy M, Okan I, Toker A, Kalayci G, Demiryont M. Hydatid cystic disease of the soft tissues with pulmonary and hepatic involvement: report of a case. Surg Today. 2003;33(1):69-71. [ Links ]
11. Unal AE, Ulukent SC, Bayar S, Demirkan A, Akgul H. Primary hydatid cyst of the axillary region: report of a case. Surg Today. 2001;31(9):803-805. [ Links ]
12. Versaci A, Scuderi G, Rosato A, Angio LG, Oliva G, Sfuncia G, et al. Rare localizations of echinococcosis: personal experience. ANZ J Surg. 2005;75(11):986-991. [ Links ]
13. Gümüş, M, Yagmur Y, Gümüş, H, Kapan M, under A, Böyük A. Primary hydatid disease of diaphragm with subcutaneous extension. J Infect Dev Ctries. 12 August 2011;5(8):599-602. [ Links ]
14. Katkhouda N, Fabiani P, Benizri E, Mouiel J. Laser resection of a liver hydatid cyst under video laparoscopy. Br J Surg. 1992;79:560-1. [ Links ]
15. Anand S, Rajagopalan S, Raj Mohan R. Management of liver hydatid cysts - Current perspectives. Med J Armed Forces India. July 2012;68(3):304-309. [ Links ]
16. Ramia JM, Poves I, Castellón C, Diez-Valladares L, Loinaz C, Serrablo A, et al. Radical laparoscopic treatment for liver hydatidosis. World J Surg. October 2013;37(10):2387-92. doi: 10.1007/s00268-013-2150-2 [ Links ]
17. Palanivelu C, Senthilkumar R, Jani K, Rajan PS, Sendhilkumar K, Parthasarthi R, et al. Palanivelu hydatid system for safe and efficacious laparoscopic management of hepatic hydatid disease. Surg Endosc. December 2006;20(12):1909-13. [ Links ]
18. Jani K. Spillage-free laparoscopic management of hepatic hydatid disease using the hydatid trocar canula. J Minim Access Surg. July 2014;10(3):113-8. [ Links ]
19. Senthilnathan P, Inamdar S, Nalankilli VP, Vijay A, Rajapandian S, Parthsarathi R, et al. Long-term results of hepatic hydatid disease managed using Palanivelu hydatid system: Indian experience in tertiary center. Surg Endosc. 6 June 2014. [Epub ahead of print] [ Links ]
20. Saglam A. Laparoscopic treatment of liver hydatid cysts. Surg Laparosc Endosc. February 1996;6(1):16-21. [ Links ]
21. Zain Al-Shareef, Osman A. Hamour, Saud Al-Shlash, Inam Ahmed, Abbas A. Mohamed. Laparoscopic Treatment of Hepatic Hydatid Cysts with a Liposuction Device. JSLS. October-December 2002;6(4):327-330. [ Links ]
 Correspondence:
Correspondence:
Yusuf Yagmur
yusufyagmur@hotmail.com


{kind=link}