










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.54 n.2 Cape Town Jun. 2016
ABSTRACTS
Abstracts of the 44th Annual Meeting Surgical Research Society of Southern Africa
Hosted by the Department of Surgery, Groote Schuur Hospital and University of Cape Town, DoubleTree by Hilton, Cape Town, 14 & 15 July 2016
FACTORS INFLUENCING MEDICAL STUDENTS IN PURSUING A CAREER IN SURGERY: A CROSS-SECTIONAL SURVEY
A J Scott1 & D Kahn1
1 UCT Faculty of Health Sciences;
2 UCT Department of Surgery
Introduction: Many factors play a role in a medical student's decision to pursue a career in surgery. With a decline in numbers of applications into surgical programs, determining the factors that influence an interest in surgery is imperative.
Aim: To determine the factors that influence medical students in pursuing a career in surgery.
Methods: A descriptive, cross-sectional survey was distributed online. The population studied included all UCT MBChB students, from year one to six, who were currently enrolled in 2016. Survey items obtained demographic data, and included; closed ended and multiple choice questions, as well as five-point Likert items. Data was imported and analysed using Excel and STATA SE software. Ethical approval was obtained from the UCT HREC (926/2015).
Results: A total of 245 medical students responded, of which 137 (56%) were female. The majority (69%) stated they were interested in pursuing a career in surgery. Seventy-five percent thought that South Africa was a good place for surgical training, whereas 19% thought training overseas would be better. Overall, 20% were undecided on what surgical specialty they would pursue. No significant association was found between respondents with parents in the medical profession, and those exposed to healthcare prior to medical school (p=0.0819). The largest proportion of respondents (33%) stated that 'length of training' was the main barrier to pursuing a career in surgery, whereas (36%) stated that 'hands-on work' was the greatest motivator.
Conclusions/Recommendations: Though length of surgical training was deemed the principal barrier, the majority of students indicated they would pursue a career in surgery. Furthermore, respondents held South African surgical training in high esteem, and were motivated by a clinically hands-on approach. These factors may play an important role in determining methods of improving numbers of surgical applications in South Africa.
MULTIDISCIPLINARY APPROACH TO PELVIC FLOOR DISORDERS: A SINGLE INSTITUTION'S EXPERIENCE
F R Rademan1, I Conradie2, A J Vermeulen2
1 Mediclinic, Durbanville
2 Division of Surgery, Stellenbosch University
Introduction: Pelvic floor disorders (PFD) are a burdern to females of all ages. Mordern management of pelvic floor disorders depends on the recognisiton of the dominant complaint, which is then investigated with dynamic imaging. The underlying pathlogy is then corrected with minimally invasive techniques.
Study Aim: To investigate the relationship between presenting complaint and special investigations, as well as the outcomes for surgeries performed for the disorders.
Methodology: Retrospective audit of a cohort of patients with PFD. Managed by a multidisciplinary team, in a single private sector institution. Data was collected between 1 February 2012 and 31 October 2015.
Data Analysis: Continuous variables, such as age, were summarised using median and range where as categorical data were summarised using percentages. Data was analysed using STATA version 3.1 and p-value of less than 0.05 will be used to define statistical significance.
Ethics: Approval from HREC Stellenbosch University (S16/01/013)
Results: 66 female patients were operated with an avarage age of 65 years (36-83). The most common main complaints were urinary tract incontinence and feacal incontinence (42%), followed by pelvic organ prolapse (35%), obstructive defacation (32%), digitalisation (24%) and rectal prolapsed (21%). Most wrere multiparous woment (89%), with 42% reporting perineal damage. All patients completed a pre-operative Pelvic Floor Distress Inventory (PFDI) short form with an avarage score of 155.3. Most patients underwent a Sacral Colpopexy (86%). One patient had a small bowel leak and three cases of post-operative urinary retention were reported. No mesh related complication to date. All patients followed up one month and six months post-operatively. Only six patietns reported the procedure to be unsatisfactory at initial follow-up. Post-operative PFDI forms were completed in 61 patients (92%), with an avarage improvement in the score of 61 points.
Conclusion/Recommendation: The outcome of the surgery for PFD is satisfactory, if investigated appropriately and managed in a multidisciplinary environment.
MORBIDITY AND MORTALITY OF HEPATECTOMY FOR BENIGN LIVER TUMOURS
A Booth, J E J Krige, U K Kotze, M M Bernon, E Jonas
Department of Surgery, University of Cape Town Health Sciences Faculty, Surgical Gastroenterology and HPB Unit, Groote Schuur Hospital, Observatory, Cape Town, South Africa
Introduction: Benign tumours of the liver are increasingly diagnosed and constitute a substantial component of hepatic tumours evaluated and resected at tertiary referral centres.
Aim: This study assessed the safety and outcome of resection of benign liver tumours at a major academic referral centre.
Method: All patients with symptomatic benign liver tumours who underwent resection were identified from a prospective departmental database of liver resection patients. Demographic data, operative management, mortality, morbidity using the Accordion classification, and follow-up were analyzed.
Results: Sixty two patients (56 women, 6 men, median age 45 years, range 17-82) underwent resection for haemangiomas n=23 (37.1%), FNH n=19 (30.6%), biliary cystadenoma n=16 (25.8%) and adenoma n=4 (6.5%). Major anatomical liver resections were necessary for large central tumours in 25 patients. Fourteen patients had 4 segments resected, 11 had 3 segments and 37 had 2 or less segments resected. Median operating time was 169min (range 80-410min). Median blood loss was 300ml (range 50-4500ml). Intra-operative blood transfusion was required in 6 patients. Intermittent portal inflow occlusion (80 mins longest, range 12-90) was used in 28 patients. The median length of post-operative hospital stay was 7 days (range 4-32). Complications occurred in 11 (17.7%) patients, Accordion grades 1 n=3, 2 n=4, 4 n= 3, and 6 n=1. Four patients required a re-operation (bleeding n=2, bile leak n=1, SBO n=1). One patient died on day 16 after a post-operative CVA (mortality 1.6%).
Conclusion: Clinically relevant symptomatic benign liver tumours comprise a substantial proportion of tertiary HPB liver resectional practice. Our data suggest that anatomically based resections can be performed safely with minimal blood loss and transfusion requirements. We advocate selective resection in symptomatic patients with benign liver tumours.
A COMPARATIVE AUDIT OF GUNSHOT WOUNDS AND STAB WOUNDS TO THE NECK IN A SOUTH AFRICAN METROPOLITAN TRAUMA SERVICE
A S Madsen, G L Laing, J L Bruce, D L Clarke
Pietermaritzburg Metropolitan Trauma Service Pietermaritzburg Metropolitan Hospital Complex University of KwaZulu-Natal Nelson R Mandela School of Medicine, South Africa
Introduction: This comparative study of gunshot wounds (GSW) and stab wounds (SW) to the neck, quantified the impact of the mechanism of injury to the outcome and management of penetrating neck injury (PNI).
Methods and Patients: A prospective trauma registry was retrospectively interrogated. Data pertaining to the following criteria was analysed: demographics and injury severity score (ISS), physiology on presentation, anatomical site of wounds and injuries sustained, investigations, management, outcome and complications.
Results: There were 452 (89%) SW and 58 (11%) GSW. Patients with GSW were more likely than SW (69% vs 63%) to have extra-cervical injuries. The incidence of a "significant cervical injury" was almost twice as high in the GSW cohort (55%) compared to the SW cohort (31%). For patients with transcervical GSW (TCGSW) this increased to 80%. The mean ISS was 17 for GSW and 11 for SW. Patients in the GSW cohort, as compared to patients in the SW cohort, presented with threatened airways (24% vs 7%) and a requirement for an emergency airway (13,8% vs 4,5%) 3 times as often as patients in the SW cohort. The incidence of injury for GSW and SW to the following structures was as follows: airway (5% vs 6%), digestive tract (12% vs 8%), vascular structures (21% vs 16%), associated cervical structures (59% vs 10 %), max-fax structures (36,2% vs 14,2%), head (16% vs 9%) and chest (35% vs 45%). In the GSW cohort 91% underwent computer tomography angiography (CTA) with 23% of these being positive for a vascular injury. In the SW cohort 74% of patients underwent CTA with 17% positive for a vascular injury. Slightly more patients with GSWs (29%) than patients with SWs (26%) required operative intervention.
Conclusion: GSWs to the neck have a worse outcome compared to patients with injuries secondary to SWs. However, the rate of neck injury actually requiring direct surgical intervention is not increased and most patients with PNI secondary to GSWs can be managed conservatively with good outcome. All GSW to the neck require imaging.
THE ROLE OF COMPUTED TOMOGRAPHIC ANGIOGRAPHY FOR THE INVESTIGATION OF VASCULAR TRAUMA SECONDARY TO PENETRATING NECK INJURY: AN AUDIT OF 380 PATIENTS
A S Madsen, J L Bruce, G V Oosthuizen, G L Laing, D L Clarke
Pietermaritzburg Metropolitan Trauma Service University of KwaZulu-Natal Nelson R Mandela School of Medicine
Background: This study investigates a large single-center experience with computed tomographic angiography (CTA) for the investigation of vascular trauma following penetrating neck injury (PNI) and attempts to develop clear algorithms for the use of this modality.
Aims: This study aimed to review the role of CTA in the assessment of PNI.
Patients and Methods: A prospectively kept trauma registry at the Pietermaritzburg Metropolitan Trauma Service (PMTS), Pietermaritzburg, South Africa was retrospectively interrogated. All patients who sustained PNI and were investigate with CTA over the four-year period January 2011 to November 2014 were included.
Results: A total of 380 patients were included in the study. The indications for imaging were as follows: Hard signs (13), Soft signs (201), no-signs (141). Seven out of 380 (1,8%) scans were indeterminate, 299 (78,7%) scans were negative and 74 (19,5%) positive for a vascular injury, of which 54 (14,2%) demonstrated arterial injury and 20 (5,3%) an isolated venous injury (IVI). Ninety vascular injuries were identified on the 74 positive CTA studies, constituting 33 venous and 57 arterial injuries. A total of eight CTAs were false positive for a vascular injury and four were false negative. The sensitivity, specificity, positive predicting value and negative predictive value of CTA in detecting an arterial injury was 93,9% (46/(46+3)), 97,5% (316/(316+8)), 85,2% (46/(46+8)) and 99,1% (316/(316+3)) respectively.
Conclusion: CTA for PNI is safe and highly sensitive and specific for demonstrating arterial injury. The rate of false negative investigation is very low although there is a significant incidence of false positive studies. All stable patients with a GSW of the neck should be imaged as there is a twenty per cent chance of an injury and clinical assessment is difficult. The management of stable patients with a SW of the neck is clinically driven. All stable patients with a soft sign should be imaged as the yield is in the order of twenty percent. All stable patients with a hard sign should be imaged. Although the yield is very high in this group in up to twenty percent of cases the injury may not require operative intervention. CTA in the absence of hard or soft signs of vascular injury has a very low yield and should not be done.
THE ROLE OF COMPUTED TOMOGRAPHY IN THE DETECTION OF AERO-DIGESTIVE TRACT INJURY FOLLOWING PENETRATING NECK INJURY
A S Madsen, J L Bruce, G L Laing, D L Clarke
Pietermaritzburg Metropolitan Trauma Service University of KwaZulu-Natal Nelson R Mandela School of Medicine, South Africa
Aims: The purpose of this study was to audit our experience with Computed Tomography (CT) for Aero-Digestive Tract Injury (ADTI) following Penetrating Neck Injury (PNI) and to assess the significance of Deep Tissue Emphysema (DTE) on CT.
Patients and Methods: A prospectively maintained trauma registry maintained by the Pietermaritzburg Metropolitan Trauma Service (PMTS), in the city of Pietermaritzburg, South Africa was retrospectively interrogated. The data of all patients with PNI investigated with computed tomography angiography (CTA) for the suspicion of vascular injury over a four-year period was reviewed. Findings of DTE on CT, defined as any tissue emphysema deep to the middle layer of the deep cervical fascia/fascia and/or mediastinal emphysema, were correlated with an aggregate standard of reference for ADTI as demonstrated by either surgical neck exploration, endoscopy, contrasted oesophagography or by direct visualisation of the injury. Using this aggregate standard of reference we determined the sensitivity, specificity, positive predictive value and negative predictive value of DTE for ADTI.
Results: A total of 383 out of 510 (75,1%) patients underwent a CTA to exclude a vascular injury following a PNI. Among the 383 CT scanned patients, were 38 patients with a Digestive Tract Injury (DTI) and all of these patients were found to have DTE on CT, except for one patient with a clinically insignificant oral cavity injury. Another 126 patients also had DTE on CT but no DTI. The sensitivity, specificity, positive predictive value and negative predictive value of DTE for the diagnosis of confirmed DTI in PNI were 97,4%, 63,5%, 22,7% and 99,5% respectively. The sensitivity and NPV were however 100% when clinically insignificant injuries were excluded. Including the group of patients with ADTI and excluding all patients with a pneumothorax, yielded a sensitivity, specificity, PPV and NPV of 94,1%, 71,9%, 30,0% and 98,9% respectively for the identification of any ADTI. When excluding clinically insignificant injuries the sensitivity and NPV were again both 100%.
Conclusion: The absence of DTE on CT for PNI seems to virtually exclude surgically significant ADTI. The presence of DTE is a non-specific finding but warrants further investigation.
A HOSPITAL BASED SURVEILLANCE SYSTEM TO ASSESS THE BURDEN OF TRAUMA IN KWA ZULU-NATAL PROVINCE SOUTH AFRICA
E Lutgeb,c N Moodleya, A Teferab, B Sartoriusc, T Hardcastled,f D Clarkee,f
a Data Management Unit, KZN Department of Health
b Epidemiology Unit, KZN Department of Health
c Department of Public Health, University of KwaZulu-Natal, School of Nursing and Public Health, Durban, South Africa
d Trauma Service, Inkosi Albert Luthuli Central Hospital, Durban, South Africa
e Pietermaritzburg Metropolitan Trauma Service, Pieter-maritzburg, South Africa
f Department of Surgery, University of KwaZulu-Natal, Durban, South Africa
Introduction: In response to the ongoing excessive burden of trauma in South Africa the Data Management and Epidemiology Units of the Department of Health in conjunction with a group of trauma specialists developed a number of trauma data variables for inclusion on the routine District Health Information System (DHIS).
Aim: The aim of this study is to describe the process followed in established i the trauma indicators and to review the 20122014 trauma data.
Methodology: The variables collected included: total patient numbers assessed in the emergency room with a diagnosis of trauma; the mechanisms of trauma (blunt assault, motor vehicle accident, pedestrian vehicle accident, stab, gunshot wound, other); any trauma patient admitted to a health facility ward/ICU for longer than 12 h; and whether the patient required transfer to a higher centre of care. All trauma deaths in hospital were recorded. The severity of trauma was measured using the Emergency Medical Services (EMS) classification of blue code (dead), red code (stretcher case with deranged physiology), yellow code (stretcher case with normal physiology) and green code (able to walk with normal physiology. The DHIS trauma data from April 2012 to March 2014 was reviewed.
Results: There were 197,219 emergency room visits for trauma in KZN in the 2013/2014 financial year. This constitutes 27.0% of all emergency room visits. The ratio of intentional to non-intentional injury is 45:55. There were 18,716 admissions to public sector hospitals for trauma in KZN in the 2013/2014 financial year. This constitutes 2.4% of all admissions in the province. There were 1045 inpatient deaths due to trauma in the same period, constituting 2.5% of all inpatient deaths. The overall rate of trauma in KZN was 17 per 1000 population.
Conclusion: The adapted DHIS has successfully collected essential data that quantify the hospital burden of trauma in KZN province. This has provided the most complete overview of the burden of trauma in the Province. These trauma indicators should remain a permanent part of the DHIS to allow planners to track the trauma epidemic and to institute informed management strategies.
MORTALITY RATES INCREASE DRAMATICALLY BELOW A SYSTOLIC BLOOD PRESSURE OF 105MM HG IN SEPTIC SURGICAL PATIENTS
D L Clarke1, P Brysiewicz2, B Sartorius2, JL Bruce1, GL Laing1
1 Pietermaritzburg Metropolitan Trauma Service, School of Clinical Medicine, South Africa
2 School of Nursing & Public Health, University of KwaZulu-Natal Nelson R Mandela School of Medicine, South Africa
Introduction: This study used a prospective surgical data base, to investigate the level of SBP at which mortality rates begin to increase in septic surgical patients. Aims This study aimed to critically evaluate the traditional use of a sBSP of < 90 MmHg to diagnose septic shock.
Methodology: All acute, septic general surgical patients older than fifteen years of age admitted between January 2012-January 2015 were included in these analyses.
Results: Of a total of 6020 adult surgical patients on the database 3053 elective patients, 1664 non-septic, 52 duplicates and 11 patients with missing systolic BP were excluded to leave a cohort of 1232 acute, septic surgical patients. The Median age (IQR): 48 (32-62) and roughly 50:50 gender ratio (620 female: 609 male). The majority of patients were African: 988 (80.2%) followed by Asians (128 or 10.4%). Over two-thirds (852 or 69.2%) of the patient cohort underwent some form of surgery and 152 or 12.3% required ICU admission. The median length of ICU stay (IQR) was 2 (1-4.5) days. The median length of total hospital stay (IQR) was 4 (2-9) days. The median systolic BP (IQR) on admission was 122 (107-138). A total of 167patients died (13.6%). Those that died did have a significantly lower mean systolic BP compared to the survivors (116 vs 125, p<0.001). Six out of 10 patients (60%) with a systolic BP <70 died. The ROC analysis suggests an optimal systolic BP cut-off of 111 when predicting mortality [area under the ROC curve (AUC): 0.6 (0.551, 0.65)]. This cut-off yields a moderate sensitivity (70%), high PPV (90%) but low specificity and NPV when predicting mortality. Based on this optimal cut-off 388 or 31.5% of patients would be classified as shocked. The inflection curve below with fitted non-linear curve (95% confidence intervals) clearly shows the upward change in observed mortality frequency at lower systolic and BE (i.e. base deficit) values. Shocked patients had a significantly higher frequency of mortality (20% vs 11%, p<0.001),a significantly higher median lactate (1.9 vs 1.5, p<0.001), and mean base deficit (-2.8 vs -1.0, p=0.001). No significant difference in mean age, ICU admission, duration of ICU admission and total length of hospital stay was observed by shocked status.
Conclusion: Our data suggests that patients who die have a significantly lower systolic BP and clinically significant hypotension in sepsis with regards to increased mortality risk begins at a level of mm Hg and this finding needs to be incorporated into bundles of care for surgical sepsis.
SHOCK BEGINS AT A SYSTOLIC BLOOD PRESSURE OF 110 MM HG IN SOUTH AFRICAN TRAUMA PATIENTS.
D L Clarke, P Brysiewiczb, B Sartorius, JL Bruce, G L Lainga
Pietermaritzburg Metropolitan Trauma Service, Pietermaritzburg Metropolitan Hospital Complex, College of Health Sciences, School of Clinical Medicine University of
Kwa Zulu-Natal Nelson R Mandela School of Medicine, South Africa
School of Nursing & Public Health, University of Kwa Zulu-Natal, South Africa
Faculty of Health Sciences, School of Clinical Medicine, University of the Witwatersrand, Johannesburg, South Africa
Introduction: This study used data from a prospectively maintained trauma database to assess the level of systolic blood pressure (SBP) at which mortality rates for trauma begin to increase and to compare SBP with BD as a predictors of outcome.
Aims: This study aimed to critically evaluate the traditional use of a sBSP of < 90 MmHg to diagnose shock.
Methodology: The Pietermaritzburg Metropolitan Trauma Service (PMTS) maintains a prospective digital trauma registry. All trauma patients admitted to the service for the period January 2012- January 2015 were included. Analysis was performed on SBP relative to a number of selected markers of outcome and a variety of physiological parameters. Results: Out of an original dataset of 2974 trauma patients a total of 169 elective patients, 799 patients with isolated TBI and 27 patients with incomplete data were excluded to leave a sample size of 2148 patients. Of this 1830 (85.2%) were male and 318 (14.8%) were female. The mean age (SD) was 31.8 (12.0). The median age and (IQR) was 29 (23-37). There were 89 deaths in this cohort (4.1%). The Median systolic BP and (IQR) was 123 mm Hg (112-136). The median base deficit was -1.4 (interquartile range: -4.5 to 1). The inflection curves below with fitted non-linear curve clearly shows the upward change in mortality frequency around a SBP of 110 mm Hg and lower as well as for a base deficit below -5. A cut-off of less than 110 for SBP yields a high sensitivity and very high Positive Predictive Value (PPV) of 82% (95%CI: 81-84) and 98% (95% CI: 97-98) but low specificity (56%) and Negative Predictive Value NPV (12%) respectively. Similar optimal cutoff analysis for base deficit (BD) vs mortality suggests BD>4.8 as a good predictor AUC (0.82, 95% CI: 0.75-0.88). This cutoff yields a high sensitivity of 80% (95% CI: 78-82), moderate specificity of 75% (95% CI: 62-85), very high PPV of 98% (95% CI: 97-99) but low NPV of 17% (15-28).
Conclusion: The data suggests that traumatic shock starts to become manifest at a SBP of 110mm Hg and that a SBP reading of 90mmHg represents an advanced state of shock. SBP by itself is a poor predictor of mortality and outcome. BD appears to be a far better predictor of mortality than SBP.
CLASSIFICATION OF SHOCK USING BASE DEFICIT AT PRESENTATION OUTPERFORMS TRADITIONAL MODEL BASED ON VITAL SIGNS IN PREDICTING MORTALITY IN A COHORT OF 3047 SOUTH AFRICAN TRAUMA PATIENTS
M P Dunham1, D L Clarke1, P Brysiewicz2, B Sartorius2, J L Bruce1, G L Laing1
1 St Helen's & Knowsley NHS Trust, United Kingdom Pietermaritzburg Metropolitan Trauma Service, School of Clinical Medicine, South Africa
2 School of Nursing & Public Health, University of KwaZulu-Natal Nelson R Mandela School of Medicine, South Africa
Background: An assessment of the physiological status is a key step in the immediate assessment of the trauma patient. Vital signs are frequently used to help achieve this. Base deficit has been shown to predict outcomes in trauma patients and is now a feasible alternative as a "front door" assessment tool given its increasingly widespread availability as a point of care test.
Aims: This study compared the traditional ARTSL classification of shock with a base deficit based classification to see which was the better predictor of mortality
Methods: 3047 adult trauma patients presenting to the Pietermaritzburg Complex of Hospitals, KwaZulu Natal, Republic of South Africa were categorised into four classes of shock based on either base deficit or vital signs. The mortality rates using each classification were compared.
Results: There was a step-wise increase in mortality from Class 1 (1.8%) to Class 4 (23.5%) when patients were classified into four groups using base deficit. The difference in mortality between each shock class group when classified by base deficit was statistically significant. Mortality increased from Class 1 (0.7%) to Class 4 (19.2%) when classified by ATLS criteria but the difference between groups was only statistically significant between Class 3 (2.4%) and Class 4 (19.2%) where there appeared to be a large "jump" in mortality. The population studied involved 47% penetrating trauma patients and 50% blunt trauma patients.
Conclusion: Where blood gas measurement is immediately available classification of shock using base deficit at hospital presentation should be considered in preference to the traditional approach based on vital signs.
TOWARD A STANDARD APPROACH TO MEASUREMENT AND REPORTING OF PERIOPERATIVE MORTALITY RATE AS A GLOBAL INDICATOR FOR SURGERY
R Ariyaratnam1, C L Palmqvist2, P Hider3, G L. Laing4, D Stupart5, L Wilson6, D L Clarke4, L Hagander2, D A Watters7 and R L. Gruen8,9
1 Monash University & Barwon Health, Melbourne, Australia
2 Department of Clinical Sciences in Lund, Paediatric Surgery and Global Paediatrics, Faculty of Medicine, Lund University, Children's Hos- pital, Lund, Sweden
3 Perioperative Mortality Review Committee, Health Quality and Safety Commission, Department of Population Health, University of Otago, Christchurch, New Zealand
4 Department of Surgery, Pietermaritzburg Metropolitan Trauma Service, Pietermaritzburg Metropolitan Hospital Complex, Nelson R. Mandela School of Medicine, University of KwaZuluNatal, Pietermaritzburg, South Africa;
5 Deakin Univer- sity and Barwon Health, University Hospital Geelong, Geelong, Australia
6 Perioperative Mortality Review Committee, Health Quality and Safety Commission New Zealand, Department of Anaesthesia, Hutt Valley District Health Board, Lower Hutt, New Zealand
7 Department of Surgery, Deakin University and Barwon Health, University Hospital Geelong, Geelong, Australia
8 The Alfred Hospital & Monash University, Melbourne, Australia; and Lee Kong Chian School of Medicine
9 Nanyang Technological University, Singapore
Introduction: The proportion of patients who die during or after surgery, otherwise known as the perioperative mortality rate (POMR), is a credible indicator of the safety and quality of operative care. Its accuracy and usefulness as a metric, however, particularly one that enables valid comparisons over time or between jurisdictions, has been limited by lack of a standardized approach to measurement and calculation, poor understanding of when in relation to surgery it is best measured, and whether risk- adjustment is needed. Our aim was to evaluate the value of POMR as a global surgery metric by addressing these issues using 4, large, mixed, surgical datasets that represent high-, middle-, and low- income countries.
Methods: We obtained data from the New Zealand National Minimum Dataset, the Geelong Hospital patient management system in Australia, and purpose-built surgical databases in Pietermaritzburg, South Africa, and Port Moresby, Papua New Guinea. For each site, we calculated the POMR overall as well as for nonemergency and emergency admissions. We assessed the effect of admission episodes and procedures as the denominator and the difference between in-hospital POMR and POMR, including postdischarge deaths up to 30 days. To determine the need for risk-adjustment for age and admission urgency, we used univariate and multivariate logistic regression to assess the effect on relative POMR for each site.
Results: A total of 1,362,635 patient admissions involving 1,514,242 procedures were included. More than 60% of admissions in Pietermaritzburg and Port Moresby were emergencies, compared with less than 30% in New Zealand and Geelong. Also, Pietermaritzburg and Port Moresby had much younger patient populations (P < .001). A total of 8,655 deaths were recorded within 30 days, and 8-20% of in-hospital deaths occurred on the same day as the first operation. In-hospital POMR ranged approximately 9-fold, from 0.38 per 100 admissions in New Zealand to 3.44 per 100 admissions in Pietermaritzburg. In New Zealand, inhospital 30-day POMR underestimated total 30-day POMR by approximately one third. The difference in POMR if procedures were used instead of admission episodes ranged from 7 to 70%, although this difference was less when central line and pacemaker insertions were excluded. Age older than 65 years and emergency admission had large, independent effects on POMR but relatively little effect in multivariate analysis on the relative odds of in-hospital death at each site.
Conclusion: It is possible to collect POMR in countries at all level of development. Although age and admission urgency are strong, independent associations with POMR, a substantial amount of its variance is site-specific and may reflect the safety of operative and anesthetic facilities and processes. Risk-adjustment is desirable but not essential for monitoring system performance. POMR varies depending on the choice of denominator, and in-hospital deaths appear to underestimate 30-day mortality by up to one third. Standardized approaches to reporting and analysis will strengthen the validity of POMR as the principal indicator of the safety of surgery and anesthesia care.
INCIDENCE AND MANAGEMENT OF POSTOPERATIVE BILE LEAKS. A PROSPECTIVE ANALYSIS OF 467 LIVER RESECTIONS
A J Dell, S A Tromp, J E J Krige, S J Beningfield, U K Kotze, P C Bornman, S Burmeister, M M Bernon, G E Chinnery, S R Thomson, E Jonas.
Surgical Gastroenterology and HPB Surgical Unit, Department of Surgery, University of Cape Town Health Sciences Faculty
Background: Recent advances in management have reduced the morbidity and mortality following major liver resections.
However, bile leaks from the liver transection margin remain a major cause of morbidity. Our hypothesis was that detailed knowledge of risk factors for bile leakage after liver resection could reduce the incidence.
Aim: The aim of this study was to identify the incidence and risk factors for postoperative bile leakage after hepatic resection and to propose a management algorithm
Methods: The analysis was based on a prospective database of 467 consecutive liver resections completed in the HPB surgical unit at Groote Schuur Hospital between January 1988 and January 2016. Peri-operative risk factors related to the development of bile leakage were identified. Data analysis included demographics, indication for resection, total operative time, total segments resected, duration of Pringle manoeuvre, blood loss, total hospital stay as well as other 'non-leak' complications. All patients had routine closed suction drainage postoperatively. Clinical presentation of the bile leak, the need for intervention (whether minimally invasive or open) and the outcome were evaluated. Severity of bile leaks were graded according to the International Study Group of Liver Surgery and other post-operative complications according to the Expanded Accordion classification. For statistical analysis the Fischer's exact test p <0.05 was regarded as significant.
Results: Overall morbidity was 24% (n=112), with bile leaks occurring in 25 (5.4 %) patients. Severity of bile leaks were graded as A=5, B=17 and C=3. Significantly more bile leaks occurred in patients who had major resections (>3 segments) and longer total operative times (p<0.05). Bile drainage stopped spontaneously in 4 patients. In 21 patients percutaneous drainage (n=15), endoscopic biliary stenting (n=8), PTC drainage (n=3) or laparotomy (n=3) were needed. Some patients required more than one type of intervention. Median hospital stay in the 442 patients without a bile leak was 8 days (IQR 1-98) compared with 12 days (IQR 6-30) for the 26 with bile leaks (p<0.05).
Conclusion: Incidence of bile leakage was 5.4 %. These occurred after complex or major liver resections with long operative times and resulted in significantly longer hospitalisation. Most were effectively treated non-operatively by percutaneous or endoscopic biliary drainage and did not lead to death.
SURGICAL RESOURCES IN SOUTH AFRICA - A REVIEW
A J Dell, D Kahn
Department of Surgery, University of Cape Town Health Sciences Faculty
Introduction: Surgically treatable diseases comprise upward of 30% of the burden of disease globally and an estimated 5 billion people do not have safe access to surgical care. Little research around surgical resources exist in the developing world and further data are needed. No large scale formal data collection efforts have been published in South Africa.
Aim: To quantify the surgical resources in South Africa and perform an international comparison.
Methods: All hospitals were contacted telephonically and via email, between September and December 2014, and estimates of hospital number and type, surgical bed number, number of general surgeons, as well as operating theatres in all public and private hospitals were obtained. Data analysis included assessment of absolute number of resources and distribution per capita (100 000 people) for all 52 district municipalities. An international comparison was performed.
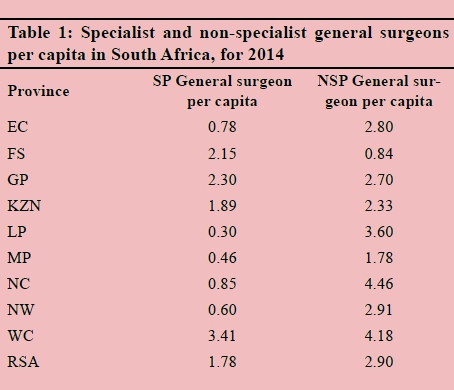
Results: Results are summarized in table 1. The largest number of public hospitals per capita are found in the Eastern Cape, with most private facilities being located in Gauteng. The Western Cape has the largest number of specialist general surgeons per capita, with a national average of 1.78 per capita. The UK has over 30 general surgeons per capita, compared with South Africa (1.78 per 100 000), where most are working in the private sector. South Africa has 3.50 theatres per capita, with the majority situated in Gauteng and the Western Cape. High income countries have between 15 and 25 theatres per capita.
Conclusion: A large and persistent disparity in surgical resources exists between provinces. Urban provinces tend to have a greater density of surgical resources, however, not necessarily when it comes to public sector resources. Further research is needed to evaluate the rest of the surgical workforce. South Africa's growing population has far fewer surgical resources than high income countries.
AN INTERNATIONAL COMPARISON OF SURGICAL RESOURCES
A J Dell, D Kahn
Department of Surgery, University of Cape Town Health Sciences Faculty
Introduction: Surgically treatable diseases comprise upward of 30% of the burden of disease globally and an estimated 5 billion people do not have safe access to surgical care. Little research around surgical resources exist in the developing world and further data are needed.
Aim: To perform an international comparison of surgical resources in South Africa.
Methods: All hospitals were contacted telephonically and via email, between September and December 2014, and estimates of hospital number and type, surgical bed number, number of general surgeons, as well as operating theatres in all public and private hospitals were obtained. Data analysis included assessment of absolute number of resources and distribution per capita (100 000 people) for all 52 district municipalities. An international comparison was performed.
Results: Results are summarized in table 1. High income countries such as the UK, USA and Australia have the most beds, theatres and general surgeons, and are the richest in surgical resources. Low income countries such as Uganda and Tanzania have fewer than 100 hospital beds per 100 000, whereas South Africa and Brazil (UMICs), have nearly 200 hospital beds per 100 000. Surgical beds are currently not used as a measure of surgical resources and no global data exist as a comparative.
Conclusion: A large and persistent disparity in surgical resources exists between countries. More work is needed regarding workforce mapping in order to determine the exact global distribution of resource number. South Africa's growing population has far fewer surgical resources than high income countries.
SURGICAL RESOURCES IN SOUTH AFRICA -MAPPING THE NUMBER OF GENERAL SURGEONS
A J Dell, D Kahn
Department of Surgery, University of Cape Town Health Sciences Faculty
Introduction: Surgically treatable diseases comprise upward of 30% of the burden of disease globally and an estimated 5 billion people do not have safe access to surgical care. Little research around surgical resources exist in the developing world and further data are needed. No large scale formal data collection efforts have been published in South Africa. Aim: To quantify the surgical workforce in South Africa, specifically general surgeon number.
Methods: All public hospitals were contacted telephonically and via email, between September and December 2014, and estimates of number of specialist general surgeons, as well as non-specialist general surgeon numbers obtained. Data analysis included assessment of absolute number of surgeons and distribution per capita (100 000 people) for all 52 district municipalities.
Results: The Western Cape has the largest number of specialist general surgeons per capita. The national average of specialist general surgeons is 1.78 per capita, where the majority are working in the private sector.
Conclusion: Urban provinces tend to have a greater density of specialist general surgeons, however, not necessarily when it comes to non-specialist general surgeons. Further research is needed to evaluate the rest of the surgical workforce. Regional hospital are poorly staffed when it comes to both specialist and non-specialist surgeons.
SURGICAL RESOURCES IN SOUTH AFRICA - PUBLIC VS PRIVATE SECTOR. A J Dell, D Kahn
Department of Surgery, University of Cape Town Health Sciences Faculty
Introduction: Surgically treatable diseases comprise upward of 30% of the burden of disease globally and an estimated 5 billion people do not have safe access to surgical care. Little research around surgical resources exist in the developing world and further data are needed. No large scale formal data collection efforts have been published in South Africa.
Aim: To quantify the surgical resources in South Africa and perform a comparison between the public and private sector.
Methods: All hospitals were contacted telephonically and via email, between September and December 2014, and estimates of hospital number and type, surgical bed number, number of general surgeons, as well as operating theatres in all public and private hospitals were obtained. Data analysis included assessment of absolute number of resources and distribution per capita (100 000 people) for all 52 district municipalities. A comparison between public and private sector was performed.
Results: Results are summarized in Table 1 (next page). The largest number of public hospitals per capita are found in the Eastern Cape, with most private facilities being located in Gauteng. There are more than twice as many public sector beds per capita than private sector beds, however surgical beds per capita are roughly the same for both sectors. The Western Cape has the largest number of specialist general surgeons per capita, with a national average of 1.78 per capita. South Africa has 3.50 theatres per capita, with the largest number of public theatres per capita in Gauteng and the Western Cape, and private theatres in Gauteng and Mpumalanga.
Conclusion: A large and persistent disparity in surgical resources exists between the public and private sector as well as between provinces. Urban provinces tend to have a greater density of surgical resources, however, not necessarily when it comes to public sector resources.
PENETRATING ABDOMINAL TRAUMA: SPECTRUM OF DISEASE IN A LEVEL 1 TRUAMA CENTRE
A N Sander,.P H Navsaria
Department of Trauma Surgery, University of Cape Town
Introduction: Penetrating abdominal trauma (PAT) in South Africa is amongst the most prevalent worldwide, representing a significant burden on the local health system. Fully understanding the spectrum of disease is the first step to equipping ourselves with the tools to optimize management.
Aim: The aim of this study was to not only describe the injury presentations and management, but their outcomes too.
Methods: The study consisted of a retrospective descriptive audit of all penetrating abdominal trauma, presenting between 1 May 2015 and 31 March 2016 to Groote Schuur Hospital Trauma Unit, Cape Town. All patients presenting to the department with PAT within these dates were included, with no exclusions. The following data was captured from the electronic trauma records (eTHR): mechanism of injury; admission vital signs; admission and discharge times; treatment modality; injury description; injury scoring; morbidity and mortality. Using this data, the Injury Severity Score was calculated.
Results: 437 patients were included which had a overall mortality of 7.5%. 152 of these were stabs, 273 gunshot wounds, and 2 were other forms of penetrating injuries. Breakdown of the mortalities were as follows: Stabs 6 (3.9%), GSW 27 (9.8%). The total morbities were 109 (24% of all patients) of which 81 were following GSW (29% of this subgroup), and 28 were following stab injuries (18% of this subgroup)
Conclusion: Trauma remains a major cause of both mortality and morbidity in South Africa and continuous efforts on all fronts are necessary to address this.
THE FATE OF PROXIMALLY EXCLUDED ILIAC ARTERIES FOLLOWING OPEN BIFURCATED REPAIR OF ABDOMINAL AORTIC ANEURYSMS
B Dube1, N G Naidoo2
1 Department of Vascular & Endovascular Surgery, Livingstone Tertiary Hospital, Port Elizabeth
2 Vascular & Endovascular Unit, Department of Surgery, Groote Schuur Hospital, University of Cape Town
Introduction: Concomitant iliac artery aneurysms have been noted to occur in 15-40% of patients with abdominal aortic aneurysms (AAAs). As a result, following open AAA repair, there is a concern regarding the progressive enlargement of the iliac arteries.
Purpose: The aim of this study was to investigate the long term outcome of proximally excluded common iliac arteries (CIAs) following open bifurcated AAA repair.
Methods: Clinical and demographic data of 165 consecutive patients undergoing open AAA repair between April 2004 and April 2014 was collected after ethics approval (HREC REF:756/2014). The aorta and iliac segments were measured in the 120 available preoperative Computed Tomographic (CT) angiograms. A single postoperative CT scan was performed and measurements recorded in 46 patients available for follow-up. The patients were grouped according to the type of surgical repair, open tube graft repair or bifurcated graft repair to the common iliac (CIA), external iliac artery (EIA) or common femoral artery (CFA). Parametric (t-test) assessment for iliac artery growth was performed.
Results: Entered into the study were 165 patients (133 men, 32 women) with a mean age of 66 years and a mean AAA diameter of 6.7cm (range 5.1 - 10.3cm). After a median follow-up of 49 months, 46 patients (88 CIAs) were available for a single postoperative CT scan. There was an overall significant decrease in the CIA diameter for proximally excluded iliacs, with a t-statistic: 3.005 (critical value at 5% significance 2.021) for CFA reconstruction and a t-statistic: 2.267 (critical value at 5% significance 2.021) for EIA reconstructions. In contrast, open tube graft repair was associated with significant CIA growth, t-statistic: -2.583 (critical value at 5% significance 2.0).
Conclusion: Open bifurcated AAA repair with proximal exclusion of CIAs appears safe and effective in intermediate and long term follow-up with no observed CIA growth.
THE ASSESSMENT OF THE RELATIONSHIP BETWEEN C -REACTIVE PROTEIN AND PREALBUMIN IN THE MONITORING OF THE INFLAMMATORY STATE IN CRITICALLY ILL SURGICAL PATIENTS
B M Mabaso, J P Pretorius, F Paruk
Departments of Surgery and Critical Care, Steve Biko Academic Hospital
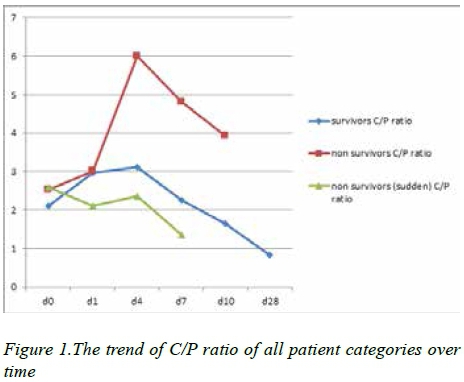
Introduction: Multiple organ dysfunction syndrome (MODS) is considered to be the leading cause of mortality in ICU patients. An uncontrolled systemic inflammatory response has been shown to be the predominant underlying mechanism. The ratio of C-reactive protein (CRP) and prealbumin (C/P) has previously been found to be promising in identifying inflammatory changes.
Aim(s): The aim of the study was to assess the ability of the C/P ratio as a tool to monitor the inflammatory state in critically ill surgical patients.
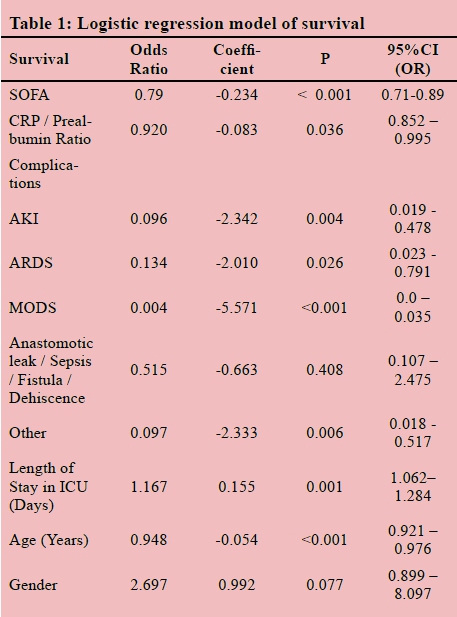
Methods: A prospective cohort study was conducted among 170 consecutive patients admitted to surgical critical care units in 2 academic hospitals. Patients aged 18 and above with a diagnosis of trauma, intra-abdominal sepsis, malignancy or other inflammatory abdominal conditions were enrolled. Sequential organ failure assessment (SOFA) scores were assessed daily and serial measurements of CRP and prealbumin performed on days 0, 1, 4, 7, 10 and 28. Spearman's correlations were tested for the SOFA, CRP, prealbumin and the C/P ratio in relation to morbidities and mortality. Ethical approval was granted by the UP Faculty of Health Sciences Research Ethics Committee.
Results: The mortality rate in this study was 25.9%. Statistical analysis demonstrated that the mortality was high in patients with acute kidney injury (AKI) (p=0.004) and highest with MODS (p<0.001). The trends of C/P ratio, SOFA and CRP over time were statistically significant for survivors compared with non-survivors across the 4 diagnostic categories. CRP and the C/P ratio showed correlations with morbidities and mortality from day 4.
Conclusion: The trend of the C/P ratio observed in critically ill surgical patients reaffirms the notion that persistent inflammation leads to organ dysfunction and morbidity. The significant differences between survivors with and without complications indicate that a C/P ratio guided therapy may reduce complications.
COMPARISON OF OUTCOMES OF MANAGEMENT OF NECROTIZING SOFT TISSUE INFECTIONS IN PATIENTS WITH OR WITHOUT HIV INFECTION
B Lawrence, T Mokoena
Department of General Surgery, Faculty of Health Sciences, University of Pretoria
Introduction: Necrotizing soft tissue infections(NSTI's) is an uncommon yet severe form of sepsis requiring urgent surgical intervention. Immunosuppression in various forms is one of the main risk factors for NSTI development and its associated mortality. The high prevalence of HIV/AIDS infection in South Africa, provides an opportunity to investigate the association between HIV/AIDS and mortality in NSTI patients.
Aim(s): To evaluate the impact of HIV on mortality and morbidity in patients admitted with NSTI's.
Methods:
• Design: Comparative cross-sectional retrospective review.
• Setting: Steve Biko and Kalafong Academic Hospital's between 2008 and 2015.
• Inclusion/Exclusion Criteria: All patients admitted with NSTI's at the above hospitals were included. Patients under the age of 18 years or with incomplete data were excluded.
• Data collected: Patients were identified using admission or discharge diagnosis, a detailed medical record review was performed by the investigator using a standardised data sheet..
• Data analysis: Data was analysed using Stata v12 system. Categorical variables were compared using Fisher's exact test with two-way tables. Factors associated with mortality were identified using univariate/multivariate analysis. P-value of <0.05 was considered statistically relevant.
• Ethical considerations: Permission was obtained from the University of Pretoria Faculty of Health Sciences Research Ethics Committee to conduct the study.
Results: A total of, 135 patients NSTI's were identified with, 60.0% (n=81) were tested for HIV of which 23.7% (n=32) were HIV positive. Overall mortality rate was 23.7%. Only 6.2% (n=2/32) died in the HIV positive group in comparison to 22.4% (n=11/49) in the HIV negative. Hypotension, pyrexia and an elevated creatinine on presentation was statistically significant predictors of mortality.
Conclusion/Recommendations: This study failed to show that HIV positive NSTI patients had a higher mortality. There is tendency for better outcomes in HIV positive patients. A prospective study investigating CD4 counts, use of ARV drugs and associated mortality in NSTI patients is recommended.
QUESTIONING THE VALUE OF ASKING RISK FACTORS IN WOMEN DIAGNOSED WITH BREAST CANCER
C Benn, S Rayne
University of the Witwatersrand; Department of Surgery, University of the Witwatersrand
Introduction: The asking of modifiable and nonmodifiable risk factors for breast cancer is taught, and executed in most breast clinics. Studies vary as to the importance of different risk factors, and the value of documentation and interpretation once a diagnosis has been made
Aim(s): This study from a single multidisciplinary breast centre randomly sampled 248 patients with breast cancer analyzing the risk factors of these women with a view to assessing routinely asked risk factors and their documented incidences
Methods: Random files over a 10year period were selected for testing a REDCAP database system. 248 patient records with detailed documentation of risk factors were analysed. Statistical data analysis and interpretation was done with the REDCAP system. Ethics approval for the database has been obtained.
Results: The average age range at diagnosis was 55 years(std dev 12) , with the youngest age 24, oldest at 83, 90% falling bet 4064yrs. Less than 2% of women started menarche at <10yrs of age,90% (1016yrs), 40% (1013yrs). Menopause Age divided into 5 yrs groups: 6% (3035yrs), 9% (5055yrs) ;40% of the women consumed alcohol; 48% used Hormone Replacement Therapy; Contraceptive Use although not a risk was seen in 95% of patients. Both groups for over a minum of 5 and the majoprity over 10yrs.Family history of cancer was documented in 70% of women, 50% of those being breast cancer. Other cancers (GIT, ovary, melanoma) accounting for less than 10%.:Mother (28%,) Maternal gran (18%), maternal aunt (25%), other (7%). Age of first pregnancy ranged from
1642yrs., 76,5 %.
Conclusion: 80% of patients had 2 or more identifiable risk factors. Whilst Menarche or age of menopause may not be extremely relevant trends were identifiable. Use of OCP was high, as was that of HRT and alcohol Cancer family history was significant thus allowing for further possible genetic assessment. Asking of risk factors is therefore critical so as to educate communities about modifiable risk factors.
RESECTION OF BILIARY CYSTADENOMAS
J C Kloppers1, JEJ Krige1, P C Bornman1, S J Beningfield2, E Jonas1, S R Thomson3
1 HPB Surgery, University of Cape Town, South Africa
2 Radiology, University of Cape Town, South Africa
3 Gastroenterology, University of Cape Town, South Africa
Introduction: Biliary cystadenomas (BCA) are rare neoplastic, septated intrahepatic cysts which are often incorrectly diagnosed and have the potential for malignant transformation. Management of biliary cystadenomas is complicated because accurate differentiation from cystadenocarcinomas before surgery is seldom possible.
Aim: The aim of this study was to assess the outcome of surgical resection of biliary cystadenomas.
Methods: Data from a departmental and faculty registered prospective liver resection database was used to identify patients who underwent surgery for biliary cystadenomas in the HPB Surgical Unit at Groote Schuur Hospital during a 15 year period from 1999 to -2015. Standard demographic variables including age and gender were documented as well as detailed pre-operative imaging, location and size of BCA, operative treatment, extent of resection, histology, post-operative complications using the Clavien-Dindo classification and long-term outcome.
Results: Thirteen patients (mean age 45 years) had surgery during the study period. All were woman. Most (11/13) were diagnosed by CT scan after investigation of abdominal pain or a palpable mass. Jaundice was uncommon (2/13). One cyst was found incidentally during elective cholecystectomy. Most cysts were located centrally. Before referral three cysts were treated with percutaneous aspiration or drainage and two were treated with operative deroofing. Four patients had liver resections by enucleation of cysts, two patients had deroofing and six had a formal liver resection. One patient needed a biliary-enteric reconstruction for an involved left duct. Mean operative time was 201 minute. No invasive carcinoma was found on histology. There was no operative mortality. One patient developed a liver abscess one month post-operatively. Two patients recurred after 24 months.
Conclusion: Biliary cystadenomas are complex problems and should be the primary diagnostic consideration in middle aged women who have well encapsulated multilocular cystic liver tumours. Surgical resection offers optimal treatment.
ASSESSMENT OF THE MICROBIOLOGICAL PROFILE OF BREAST ABSCESSES TREATED AT A TERTIARY HOSPITAL IN BLOEMFONTEIN, SOUTH AFRICA
D Menge, C Wu
Faculty of Health Sciences, Department of Surgery, University of the Free State.
Introduction: The predominant bacterial isolate in patients with breast abscess is Staphylococcus aureus. Recent data show that a proportion of Staphylococcus aureus isolates are methicillin resistant, having implications for empiric antibiotic therapy. There are no recent data on the microbiological profile of breast abscesses in South Africa.
Aims: To determine the microbiological profile of breast abscesses referred to our department and the differences in the microbiological profile between lactational and non-lactational breast abscesses.
Methods:
• Study design: Retrospective analytic cohort study.
• Setting and sampling: Stratified random sampling.
• Inclusion and exclusion criteria: Women treated for breast abscess at Surgery clinic in 2014 and had a pus sample sent for culture were included. Those without pus samples or presented before and after 2014 were excluded.
• Data collected: Dependant variables were age, bacterial isolates and findings of additional pathology after initial management. The independent variable was lactational versus non-lactational status.
• Data analysis and statistical analysis used: Continuous variables were compared using the Mann-Whitney U test. Categorical variables were compared using Fisher's exact test. Correction for multiple comparisons was done using the Bonferroni correction. P values are two-tailed. A p value of <0.05 is considered statistically significant.
• Ethical considerations: Ethical approval was obtained from the Ethics Committee and Free State Department of Health (ECUFS 63/2015).
Results: 38 women met inclusion criteria; 17 lactational and 21 non-lactational. 63 % had a positive culture: 38% Staphylococcus aureus, 13% Staphylococcus epidermidis, 13% anaerobes, 13% Mycobacterium tuberculosis, 13% Candida albicans, 8% α haemolytic streptococci and 4% Enterobacter cloacae. Staphylococcus aureus, was the most common isolate, predominated in lactating women (70% vs. 14%; p=0.03). S. aureus isolates were methicillin sensitive (MSSA). Three lactational breast abscesses cultured C. albicans. Five additional cases of tuberculosis and one carcinoma, were found on histology in the non-lactational group. No lactating patient had either tuberculosis or carcinoma of the breast (p=0.005).
Conclusion: Drainage and antibiotic cover will suffice for the majority of lactational breast abscesses. Non-lactational breast abscesses require follow up until abscess resolution or definitive microbiological or histological diagnosis.
MEETING WOMEN'S NEEDS: COST EVALUATION OF PROCEDURES FOR DIAGNOSIS OF BREAST-RELATED CONDITIONS AT A COMPREHENSIVE, PUBLIC FACILITY IN JOHANNESBURG, SOUTH AFRICA
N Lince-Deroche1, C Van Rensburg1, C Firnhaber2,3, C Benn4,5, G Rubin4,6, P Michelow7,8, S Rayne4,5
1 Health Economics and Epidemiology Research Office, Department of Internal Medicine, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
2 Right to Care, Johannesburg, South Africa
3 Clinical HIV Research Unit, Department of Internal Medicine, Faculty of Health Sciences, University of Witwatersrand, Johannesburg, South Africa
4 Helen Joseph Breast Care Clinic, Helen Joseph Hospital, Johannesburg, South Africa
5 Department of Surgery, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
6 Department of Radiology, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
7 Cytology Unit, National Health Laboratory Service
8 Department of Anatomical Pathology, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
Introduction: Access to comprehensive breast care services is a critical component of primary health care; however, it is uncommon in low-resource settings. Some literature suggests ultrasound, rather than mammography, should be routinely used to investigate breast conditions, potentially increasing access and reducing costs. However, limited information exists on the costs of breast condition management in low-resource settings.
Aim(s): To estimate the average cost per patient seen and per procedure used for the diagnosis of breast conditions in a large, outpatient clinic in a tertiary hospital in Johannesburg, South Africa, and to determine the potential cost savings of replacing mammography with ultrasound.
Methods: From August 2013-June 2014, we conducted a retrospective file review to document service delivery at the clinic. Patients were eligible for inclusion if they had a first visit between April 2011-June 2012 and were >18 years old. Micro-costing was used to estimate the costs of each procedure from the provider perspective. We calculated costs in an Excel model, using service delivery data from the review and economic inputs (staff time, supplies, equipment, labs and overhead). Costs are presented in 2014 Rands. Ethical approval was granted by HREC (Medical).
Results: During the study period, 4,834 individuals attended the clinic; 365 (356 women) were included in the sample. The average cost per breast exam was R109 when offered by a doctor. Mammography was more costly than ultrasound at R738 and R224 respectively. Stereotactic core biopsy cost an average of R3,904; ultrasound-guided biopsy was R3,219. The average cost per patient seen was R1,337. Hypothetically replacing mammography with ultrasound lowers the average cost per patient.
Conclusion/Recommendations: Comprehensive breast care service delivery would likely be less costly if ultrasound replaced mammography and stereotactic procedures as the routine first investigation for breast conditions. Lessons learned from this clinic could improve access in low-resource settings.
LEVELS OF CIRCULATING CYTOKINES IN SOUTH AFRICAN PANCREATIC DUCTAL ADENOCARCINOMA PATIENTS: A PRELIMINARY REPORT
YY Yako1, M Brand1,2, J Devar1,2, N Lahoud1, M Smith1,2, D Kruger1
1 Department of Surgery, School of Clinical Medicine, Faculty of Health Sciences, University of Witwatersrand.
2 General Surgery, Chris Hani Baragwanath Academic Hospital
Introduction: Several studies have investigated the association of differentially expressed cytokines with pancreatic ductal adenocarcinoma (PDAC), but none in African countries.
Aim(s): The study aimed at investigating T-helper (Th) cell and angiogenic cytokines as diagnostic or prognostic biomarkers for PDAC in Black South Africans.
Methods: We conducted a prospective, case-control study that included 34 PDAC patients and 27 control participants with either abdominal aortic aneurysm or acute abdomens from causes other than HPB. Plasma levels of IL-2, IL-4, IL-6, IL-10, TNF, IFN-Y, IL-17A, VEGF, sVEGF-R1, FGF, PIGF, PDGF and P-selectin were measured using the commercially available Th1/Th2/Th17 BDTM cytometric bead array, single ELISA and multi-analyte Luminex kits.
Results: Significantly higher levels of IFN-γ (p<0.001), TNF (p<0.001), IL-2 (p=0.001), IL-4 (p=<0.01), IL-10 (p<0.01), IL-17A (p<0.01), PIGF (p<0.0001) and bFGF (p<0.0001) were found in PDAC patients compared to control participants. A sub-group analysis of PDAC patients demonstrated that those with irresectable tumours had higher plasma levels of VEGF (p=0.026), IL-10 (p=0.046), and IL-6 (p= 0.01). Lower levels TNF (p=0.028) were associated with 12-months survival. A univariate analysis showed an association between sVEGF-R1, IFN-γ and PDAC: odds ratio (95% CI) 0.998 (0.997- 0.999) (p=0.032) and 2.307 (1.119 - 4.755) (p=0.023), respectively. However the significance was lost in a logistic regression model. .
Conclusion/Recommendations: Our preliminary data suggests a potential role for VEGF, IL-10, IL-6, IFN-γ and TNF as PDAC prognostic biomarkers in South African patients.
THE COMPETENCE AND CONFIDENCE OF RECENTLY GRADUATED SOUTH AFRICAN DOCTOR IN MANAGING A PATIENT WITH BURN INJURIES
D Naudé, E Kuun, N L Allorto
Pietermaritzburg Metropolitan complex, Edendale hospital. Department of general surgery, University of Kwa-Zulu Natal
Introduction: 1,6 million burn injuries occur annually in South Africa. Ninety percent are minor to moderate and will be treated by junior doctors and non specialists. Poor management results in significant morbidity and mortality. No data exists on the quality and quantity of undergraduate teaching.
Aim: To determine the confidence and competence of first year medical interns, regarding the initial management of burn patients.
Methods: A questionnaire was distributed among first year medical interns for 2016 in the Pietermaritzburg Metropolitan Complex on orientation as well as over the following three months. No intern had done their surgery block at that time. The data was captured onto Microsoft Excel 2010 for descriptive analysis.
Results: Seventy-eight questionnaires were completed, which was a response rate of 68.4%. Interns from 7 of the 8 medical schools were represented. Five percent had no clinical exposure and 55% had only one day clinical exposure. Eighty-one percent rated training as poor or average. The Lund and Browder chart was never chosen to calculate total body surface area (TBSA). Fifty-eight percent were not sure what dressings to use for a clean superficial partial thickness wound. One third will give antibiotics prophylactically to burn patients. Surgical exposure is limited with 62% never having observed a split skin graft operation. Rating their own confidence was poor to average in 76% in a variety of areas including depth and TBSA assessment, performing escharotomy, airway management, pain management, diagnosis of infection and choice of dressing.
Conclusion: There is no consistency in the undergraduate training of burns management. Doctors are not confident with burn injuries with serious deficits in basic principles. A standardized curriculum for undergraduate training should be adopted, with additional post graduate teaching during internship in order to equip doctors before commencement of community service.
THE EFFECTS OF VIDEO GAMING ON LAPAROSCOPIC SURGICAL SKILLS
D Kahn, M Omar, M Potter, H Lee, L Mohamed, S Scheidereiter
Department of Surgery, University of Cape Town
Introduction: Video gaming is an ever-increasing industry, progressively becoming incorporated into global culture. There has been considerable interest to whether video game usage correlates with improved laparoscopic ability, as well as the effect of "warming-up" before performing a task. This study aims to explore the influence of different genres of gaming as a "warm-up" to laparoscopic performance, as well as to validate the findings of previous studies that video gaming increases laparoscopic performance.
Methods: 28 undergraduate students from The University of Cape Town participated in this study. All participants were non-gamers (<3 hours of gaming a week). Students were randomly assigned into one of three groups. 2 groups received gaming intervention while the 3rd comprised the control. All groups underwent a baseline test. Thereafter, at the conclusion of the gaming intervention, students repeated the laparoscopic tasks. Assessment was based on time of completion.
Results: Participants who played video games as a warm-up to laparoscopic performance showed better results than those in the control group. Additionally, the Formula 1 group demonstrated a 9,42% better improvement than the Call of Duty group. However, these differences were deemed insignificant as the Student T-test provided values above the significant level (0,05) upon comparison of percentage improvements.
Conclusions/Recommendations: This study showed that those who received gaming intervention showed better improvement than those in the control group, hence validating previous studies that proposed the idea of improved laparoscopic skills after video gaming experience. Moreover, results indicated that Formula 1 (a racing game) proved to be more effective than Call of Duty (a first-person shooter game) as a "warm-up" to laparoscopic performance. Further study is recommended with a more diversified selection of game genres to obtain more accurate information.
THE EFFECT OF STIMULANTS (RED BULL) ON SURGICAL TECHNICAL SKILLS
D Kahn, G Karam, Z Kalbskopf, R Toi, F Lekalakala
Department of Surgery, University of Cape Town
Introduction: Surgeons often make use of stimulants such as red bull to counteract sleep deprivation, tiredness or fatigue. In this view, using stimulants will enable them to perform medical techniques at their optimal level and minimise the risk of putting the life of their patients in danger. Red bull is known to assist with increasing alertness, focus and concentration. This study is aimed at investigating the effects of commonly used stimulants on surgical skills.
Methods: This was an experimental study on medical students without prior experience and training on Minimally Invasive Surgical Trainer-Virtual Reality laparoscopic simulator. Participants were divided into two groups on different days and were given five minutes each to familiarise themselves with the equipment by completing a practice round with a single task. After wards they were given a stimulant and the parameters used to assess them was the time taken to complete the various tasks, the number of errors and level of tremor.
Results: In our study 50% of our experiment completed the assigned tasks in less than 14:24 and 50% of the control group completed in less than 15:08. The experiment group committed more errors and scored higher on the tremor scale compared to the control group. From our student t-test we got a p-value of p=0.73.
Conclusions/Recommendations: From our results that we got from our study we can infer that our stimulant (Red Bull), does not have a significant impact on surgical techniques. However the experiment group committed more errors and experienced more tremors.
Our results had outliers that could have affected our data and skewed it.
THE EFFECT OF FATIGUE ON SURGICAL SKILLS
D Kahn, D Richards, C Cattell, R Chikte, O Rademan, K Pitso
Department of Surgery, University of Cape Town
Introduction: Fatigue is experienced by medical professionals due to their strenuous work schedules and long work hours. Sleep deprivation has negative effects on neuro-behavioural performance. The aim of this study was to determine what effect fatigue has on surgical psychomotor skills and cognitive ability.
Methods: Nineteen 2nd year Medical students were recruited and randomly allocated into either the rested (control) or fatigued (experiment) group. They had to complete a series of five laparoscopic tasks: four psychomotor tasks and one task that included test for memory and cognitive.
Results: The fatigued students took longer to complete the tasks and made more errors, but made less errors in the cognitive task. However, the difference was found to be insignificant between the two groups on the measures of time (p-value = 0.47), and number of errors (p-value <0.05). 77% of the fatigued students scored upper grades for accuracy, while 70% of the rested students scored lower grades.
Conclusions/Recommendations: These results show that fatigue does not have a significant detrimental effect on psychomotor and cognitive skills in the performance of the laparoscopic tasks in this study.
THE EFFECT OF ALCOHOL ON SURGICAL TECHNICAL SKILLS
D Kahn, M Sathekge, E Shorer, Y Msomi, B Walker, K D Shilote
Department of Surgery, University of Cape Town
Introduction: To examine the immediate effect of consuming two to four shots of vodka on laparoscopic surgical performance.
Methods: All participants were trained in all three tasks before alcohol intervention. Then they all did a baseline test. Participants were then randomized to either consume alcohol (two shots) or lemon twist. Thirty minutes after liquid consumption, subjects were assessed. Similar procedure was done after another two shots of vodka. Therefore participants either consumed four shots of vodka or lemon twist in total. Comparison between the two groups was evaluated using the Student's T test.
Results: Both groups performed similar at baseline, but the alcohol group showed deterioration on all performance measures except time after alcohol consumption. After four shots of vodka, the alcohol group performed worse. However in all outcome measures, score differences between the two groups were not statistically significant (P>.005) except for accuracy (P<.02) after two shots and (P=.006) after four shots.
Conclusions/Recommendations: Two shots appeared to degrade surgical performance thirty minutes after consumption. After four shots, the surgical performance was worse especially accuracy, suggesting the need to regulate alcohol consumption when surgeons are on call.
CHALLENGING THE THRESHOLD FOR INTERVENTION IN BREAST CANCER RELATED LYMPHOEDEMA
C D Ness1, S S Maharaj2, I Buccimazza3
1 Physiotherapy Dept. Health Sciences, UKZN
2 Physiotherpay Dept, Health Sciences, UKZN
3 Breast Unit, Dept. of General Surgery, Nelson R Mandela School of Medicine, UKZN
Introduction: Breast Cancer Related Lymphoedema (BRCA Ly) is clinically diagnosed once a 2cm circumferential difference is measured between the affected and unaffected limb, equating to 200ml limb volume difference (LVD). Aim(s):
1. To determine at what limb volume difference (LVD) the lymphatic system starts to fail (pre-clinical) by using Bio Impedance Spectroscopy (BIS).
2. To determine whether this correlates with a different circumferential/LVD measurement?
Methods: This was a prospective study comprising 60 consenting, female BRCA survivors, post adjuvant therapy at the Provincial Oncology Clinic KZN. We included all consenting women up to 18 months post radiation and excluded patients with bilateral BRCA or other primary cancers, previous mantle field radiation.
Data collected included epidemiological information extracted from the patient files, circumferential limb measurements with a tape measure and electrical impedance in the subcutaneous space using the LDEX-U400 BIS unit.
The study was approved by the UKZN Bio-ethics Research Committee BE250/010.
Results: BRCA Ly cut off at >200ml performed fairly well as a diagnostic tool for true abnormality based on BIS sensitivity of 67% and specificity of 93% ( AUC 0.8). Using a cut off of >100ml based on BIS abnormality scores, performed better with sensitivity but specificity was reduced to 69% (AUC 0.84). Optimal break point in actual continuous volume at169ml performed best in terms of diagnostic capability for abnormal/normal BIS, PPV of 71% and NPV of 93%, 95% CI: 0.86-0.99.
Conclusion/Recommendations: This study shows that the lymphatic systems optimal breakpoint for lymphatic system failure is 169ml LVD, which corresponds significantly to abnormal BIS readings. Using a clinical threshold of 100ml/1cm LVD provides 100%NPV but only 52% PPV versus NPV of 93% and PPV of 71% if 169ml LVD is used as a threshold for intervention of lymphatic drainage therapy. Early intervention of risk reducing strategies for patients improves quality of life, function and reduces costs for patients and stakeholders in a low resource setting.
IS THERE A ROLE FOR LAPAROSCOPY IN RELOOK SURGERY POST LAPAROSCOPIC APPENDECTOMY?
F Mosai, MZ Koto
Minimal Invasive Unit, Department of General Surgery, Sefako Makgatho Health Sciences University
Introduction: Intra-abdominal collections post laparoscopic appendectomy is a well-recognized complication. The approach in the management thereafter is controversial, with some people advocating percutaneous drainage and others laparotomy. Currently there is no literature that has looked at the role of laparoscopy this patients.
Aim: To assess the role of laparoscopy in relook on demand post laparoscopic appendectomy.
Methods: All patients who received laparoscopic appendectomy from June 2012- October 2015 at DGMAH were reviewed. Data was collected retrospectively from the database. A sub-group analysis of all patients who went for relook was done. Patients were grouped in to four categories based on their initial intra-operative findings: uncomplicated appendicitis, localised pus, appendix mass and 4 quadrant pus. Data regarding intra-operative findings on relook was collected and patients overall outcomes were recorded.
Results: Of the 746 patients who were reviewed, 576 were included in the study. Overall relook rate was 7% (43 cases) and all patients were relooked on demand. Uncomplicated appendicitis 1% (6 cases), Intra-operative findings were: port site bleeding =1, port site hernia =1, negative findings =4. Localised pus 1.4% (8 cases), Intra-operative findings were: pelvic collection =2, port site sepsis =1, negative findings =5. Appendix mass 0 %( none). Four quadrant pus 5% (29 cases), Intra-operative findings were: pelvic collections =22, port site sepsis =2, sub-phrenic collection =3, liver abscess =1, SBO =1.
Outcome: Conversion rate 0%. Procedure related complications 0%. Negative relook 21% (9 cases) and positive relook 79%.
Conclusion: Zero conversion rate and complication rate suggest that laparoscopy might have a role in relook surgery. The high negative relook rate means unnecessary laparotomies were avoided and on the other hand maybe our thresh-hold for relook was too low. However more research is needed to answer this question adequately, especially prospective studies.
LOW COST LAPAROSCOPIC APPENDECOTOMY IN AFRICA: SINGLE CENTRE EXPERIENCE
F Mosai, M Z Koto
Minimal Invasive Unit, Department of General Surgery, Sefako Makgatho Health Sciences University
Introduction: There have been several studies recently which looked at the cost-effectiveness of Laparoscopic Appendectomy compared with open appendectomy. But there are no studies which compared the cost of LA using commercially available consumables and using 'hand-made" alternative consumables.
Aim: To share our experience and techniques in using handmade consumables to make Laparoscopic Appendectomy cost-effective.
Methods: Retrospective analysis of a prospectively collected data from June 2012- October 2015 was reviewed. The total costs for hand-made consumables per patient were calculated. Data regarding the technique of handling the mesoappendix, appendicular stump, retrieving the specimen was collected. Intraoperative complications such as excessive bleeding from appendicular artery and iatrogenic bowel injury were noted.
Results: 746 patients were reviewed and 576 were included in the study. All patients were offered Laparoscopic appendectomy using hand-made consumables. The age group ranged from 4 to 82 with a mean of 26.37. The sex ratio was 380 males: 196 females. Uncomplicated cases were 355, complicated cases with: four quadrant pus were 116, localised pus was 95, appendix mass were 10. The total costs of handmade consumables and commercially made consumables were $1.30 and $1,397.33 per patient respectively. The conversion rate was 1.4% (uncomplicated cases), 13.7% (in four quadrant pus), and 3.1% in localised pus, none in appendicular mass. Complications: iatrogenic bowel in jury were 2 cases (one with localised pus and one with four quadrant pus), both were offered an ileostomy. No excessive bleeding was noted in all cases.
Conclusion: This study suggests that hand-made consumables are safe and feasible cost-saving alternative measure in performing LA.
LAPAROSCOPIC APPENDECTOMY AS A STANDARD OF CARE FOR BOTH COMPLICATED AND UNCOMPLICATED APPENDICITIS, IS IT SAFE AND FEASIBLE? : SINGLE CENTER EXPERIENCE
F Mosai, K Z Koto, MZ
Minimal Invasive Unit, Department of General Surgery, Sefako Makgatho Health Sciences University
Introduction: Laparoscopic Appendectomy has been widely accepted as safe and feasible when used in carefully selected patients. However acceptance of the procedure as a standard of care has been surrounded by many controversies, with the main concern been around the safety and feasibility of the approach in complicated cases.
Aim: The purpose of this study was to describe our single centre experience in using laparoscopic appendectomy (LA) as the standard of care for both complicated and uncomplicated appendicitis in South Africa as a developing country with limited resources in public sector.
Methods: A retrospective analysis of all patients diagnosed with appendicitis who received laparoscopic appendectomy over a 3 year period (June 2012- October 2015) at DGMAH were considered for the study. Data was retrieved from the database and analysed using a descriptive and analytical statistics.
Results: 746 patients were reviewed and 576 were included in the study. All patients were offered Laparoscopic appendectomy. The mean age was 26.37. Ratio: 66% males and 34% females. Uncomplicated cases were 355, four quadrant pus were 116, localised pus were 95, appendix mass were 10 cases. The length of hospital stay was averaged at 1.1 days for uncomplicated cases, 2.3 days for localised pus, 1.3 days for appendix mass, and 4.8 days for four quadrant pus cases. The difference in operating times was noted as 45-65 min for uncomplicated cases, 55-80 min for localised pus and appendix mass, and 59-240 min for four quadrant pus cases. The overall conversion rate was 4%, with procedure related complication rate of 0.5%, post-op complication rate of 5% and 7% relooks. Morbidity was 2% and mortality was 1.7%.
Conclusion: A relatively low conversion rate (4%) and procedure related complication rate (0.5%) suggest that LA is relatively safe and feasible to use even in complicated cases.
EFFECT OF METFORMIN ON ARGININE UPTAKE IN PANCREATIC DUCTAL CANCER CELLS
M J Nel, M Brand, J Devar, J Omoshoro-Jones, M D Smith, G P Candy
Department of Surgery, School of Clinical Medicine, Faculty of Heath Sciences, University of the Witwatersrand, Johannesburg
Inroduction: Cancer and type 2 diabetes share risk factors including age, sex, obesity, diet, use of alcohol, smoking and physical inactivity. Low-grade inflammation and oxidative stress from elevated glucose concentrations are implicated in the development of cancer. Pancreatic cancer ranks amongst cancers with the poorest outcomes and rapid development of type 2 diabetes is a risk factor for this cancer. Accumulating evidence suggests that the use of metformin, not other drugs used to treat type 2 diabetes, may inhibit cancer cell growth and proliferation. Metformin is believed to inhibit the mTORC1 pathway, the mammalian target of rapamycin complex 1, a central controller of growth which responds to the availability of nutrients. Metformin has a chemical structure similar to arginine.
Aim: We determined the effect of metformin on arginine uptake in a pancreatic adenocarcinoma cell line.
Methods: MIA PACA-2 cells were grown to confluence, depleted of arginine and exposed to metformin for 30 minutes. 3H-Arginine uptake was then measured over 30sec and accumulated radiolabel determined by scintillation counting.
Results: Metformin enhanced arginine uptake into the cells up to 170±7% with a bell-shaped dose-dependency curve on the concentration of arginine and metformin.
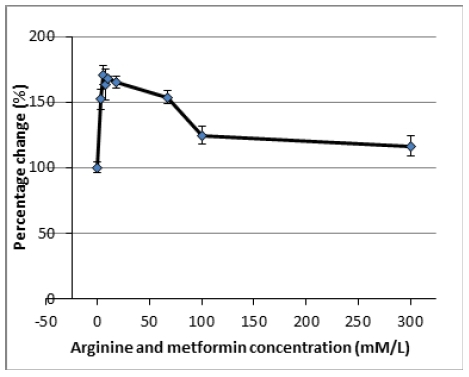
Conclusion: The data suggested metformin enhanced arginine uptake by y+L rather than y+ transport. As dietary arginine increases mTORC1 signaling, these data do not explain the beneficial effect of metformin in cancer.
DETERMINING THE FACTORS INFLUENCING TRANSFUSION TRIGGERS FOR SURGICAL PATIENTS ADMITTED TO WORCESTER HOSPITAL (WPH)
HP Mouton1,2, O Swart2,3, B G De John1, R C Duvenage1,3
1 Department of General Surgery, Worcester Provincial Hospital
2 Department of Surgery, Tygerberg Hospital, Stellenbosch University
3 Ukwanda, Rural Clinical School, Stellenbosch University
Introduction: Blood transfusions are an integral part of managing surgical patients. However, the use of blood products has transfusion-associated mortality and morbidity. Blood products are also an expensive and scarce commodity making strict application of transfusion indications essential.
Aim(s): To determine the factors that influence the decision to transfuse blood products to surgical patients admitted to WPH.
Methods: The study is a retrospective review of all 321 patients receiving blood products or services from Western Province Blood Transfusion Services (WPBTS) out of 2488 surgical admissions during June 2013 to May 2014. Data was obtained from surgery discharge and WPBTS billing databases of WPH. 477 transfusion events, defined as each individual service request to WPBTS, were identified. Patient records were reviewed to identify the motivation for transfusion events. All patients incorrectly diagnosed with surgical pathology were excluded. Ethical approval was obtained from Stellenbosch University Health Research Ethics Committee (#N14/09/125). Statistical analyses were performed using Microsoft Excel.
Results: Hospital records of 302 of the 477 transfusion events were available for review. 816 units of red blood cells were transfused: 22.7% for trauma, 64.2% for non-trauma surgical emergencies, 6% for burns and 7.1% for elective surgery. Upper gastro-intestinal bleeding was responsible for 51.2% of transfusions in non-trauma surgical emergencies. 61.3% of red blood cells transfused were transfused to haemodynamically unstable or symptomatic patients. This group received a median of 2 Units with an average Hb of 7.1g/dl. Fresh frozen plasma was used 75% as part of a massive transfusion. Only three patients received platelets.
Conclusion: In general the transfusion practices in trauma were appropriate. Stricter adherence to minimum transfusion thresholds in elective and non-trauma surgical emergencies, especially in the peri-operative setting, is needed. A hospital specific transfusion policy, in conjunction with anaesthetics, with appropriate oversite of junior staff must be prioritised.
BREAST PAIN IS NOT ASSOCIATED TO BRA-FITTING IN AN URBAN SOUTH AFRICAN POPULATION
H Adam, A Kopke, T Amukoto, C Nieuwenhuizen, N Dlamini, E Orsmond, S Weinstein, A J Murray, C Sahd, J Parrish, T Magagula, N Mallick, D Mathew, A Philip, C Benn, S Rayne
Department of Surgery, University of the Witwatersrand
Introduction: Mastalgia is a common presenting complaint requiring referral to breast clinics. The relationship between bra size, bra-fitting and breast pain is poorly described in the literature.
Aim: To determine whether an association exists between incorrectly fitted bras and breast pain in South African women.
Methods: This was a cohort study which included 195 adult female patients with a convenience sample of patients from sampled from the general medical wards of two public hospitals. Lactating and pregnant women were excluded. Data was collected using a questionnaire which the participants answered regarding the fit of their brassiere and measurement of their correct bra size using a recognised method of measurement. Data was tabulated and interpreted using Microsoft Excel® software. The study was approved by the HREC (Medical).
Results: Of the 169 included patients between 18 and 76 years, 37% experienced breast pain. 36.7% of participants were wearing incorrectly sized bras however, only 12% of participants who experienced breast pain wore the incorrect bra size (p=0.486). 48% of the sample had large breasts (above a C-cup) and 46% of these women experienced mastalgia. This was not significant. In total 40.5% of women experienced bra-related pain. Women who wore underwire bras reported more pain. There was an association between the use of combined oral contraceptives and the presence of breast pain (p=0.048).
Conclusion/Recommendations: Fewer women in our study wore the incorrect bra size when compared to previous literature, however, women who wore underwired bras reported more pain. There was no statistically significant association noted between breast pain and incorrectly fitted bras, but there was to the use of hormonal contraceptives and the presence of breast pain. Further research is needed to clarify whether there is a relationship between breast pain and the use of hormonal treatment.
PENTRATING CARDIAC INJURY AT A REGIONAL HOSPITAL: REFER ON OR MANAGE?
I I Sardiwalla, M Z Koto MZ
Department of General Surgery, Sefako Makgatho Health Sciences University
Introduction: Penetrating trauma to the heart is commonly encountered in South Africa. Rapid diagnosis and management of patients can salvage patients that would otherwise die. The presence of cardiothoracic surgeons with the ability to perform cardiac bypass is useful especially with complex injuries. This service is only available in certain large urban academic centers. In regional hospitals general surgeons must embark to repair these injuries in an attempt to save lives.
Aim: To review the technique of repair and mortality outcomes of penetrating cardiac injury performed at a regional hospital.
Methods: All patients with a preoperative diagnosis of penetrating cardiac injury that underwent operative repair between January 2000 and December 2010 at Sebokeng Regional Hospital were included. Patients were resuscitated according to ATLS protocol. If the patient was stable a FAST was performed. If pericardial fluid was detected a pericardial window was done followed by a median sternotomy. If unstable the patient proceeded to have a left lateral thoracotomy. Operations were performed by surgeons of varying levels of experience from medical officer to consultant.
Results: 46 patients with penetrating cardiac injury were identified. 40 (86%) were male. Median sternotomy was the incision used in 33 patients (71%). One patient had a laparoscopic exploration for a thoraco-abdominal gunshot wound with a laparoscopic pericardial window. Operating time averaged 114 mins (45-225). Injuries to the left ventricle occurred in 24 (53%) cases and to the right ventricle in 22 (47%) cases. The injuries averaged 1,5cm in length (0,5-4). There were two mortalities (4%). One patient died in ICU and the other died on the table.
Conclusion: Penetrating cardiac injuries can be managed safely at a regional hospital with levels of mortality comparable to major urban trauma centers. Key to successful management of these patients is rapid diagnosis and prompt intervention.
PAEDIATRIC ENDOSCOPE FOR DEPLOYING SELF EXPANDING METAL STENTS IN CANCER OF THE OESOPHAGUS
I I Sardiwalla, C C Osuagwu, M Govender, M Z Koto
Department of General Surgery: Sefako Makgatho Health Sciences University
Introduction: Oesophageal carcinoma is a major cause of cancer related deaths. Metal stents are considered an established treatment option for palliation of dysphagia. These stents are classically deployed using endoscopy with fluoroscopic control. A guidewire is passed through the stricture using fluoroscopy to control the deployment of the stent. This entails exposure of the staff to radiation. An alternative technique is using the paediatric endoscope. The Olympus Evis Exera III Scope GIF-XP190N has a small 5,4mm external diameter. This means that often the stricture can be negotiated using the scope. The guidewire is passed into the stomach under direct vision. The length of the stricture can be measured on withdrawal and a stent of appropriate dimension deployed.
Aim: To determine if it is feasible and safe to use a paediatric endoscope to stent carcinoma of the oesophagus.
Methods: The study is a retrospective review of the endoscopy database from March 2015 to May 2016. All cases where the oesophagus was stented underwent review. Those where the paediatric scope was used were further analysed. Failures or complications were documented.
Results: A total of 51 stents were performed of which 31 included use of the paediatric scope. The procedure was successfully completed in 25 out of 31 attempts (80,6%) of the patients. Four tracheooesophageal fistulas and one oesophageal perforation was stented successfully. The length of the stricture averaged 9,6 cm (5-15). There were no complications related to stent insertion. In the six cases that failed the reason was inability to negotiate the stricture. All these cases were subsequently completed successfully using a guidewire with fluoroscopy.
Conclusion: It is safe and feasible to use the paediatric endoscope to stent tumours of the middle and distal oesophagus. If the procedure is successful it prevents the exposure of the staff to radiation.
ERCP-GUIDED CHOLANGIOSCOPY USING A SINGLE USE SYSTEM: NATIONWIDE REGISTER-BASED STUDY OF ITS USE IN CLINICAL PRACTICE
J Lubbe1, U Arnelo2, L Lundell2, F Swahn2, B Tornqvist2, E Jonas2, M Lohr2, L Enochsson2
1 Division of Surgery, Tygerberg Hospital and University of Stellenbosch, Parow, South Africa
2 Division of Surgery, department of Clinical Science, Intervention and Technology, Karolinska Institutet, Stockholm, Sweden
Introduction: Cholangioscopy during ERCP (endoscopic retrograde cholangio-pancreatography) has gained widespread application in recent years. Various systems are available for use, but the SpyGlass® System enables direct duct visualization and intervention, by a single operator. There are no studies available scrutinizing its more widespread clinical application and possible accompanying adverse events.
Aim: The present report aims to address the use of SpyGlass cholangioscopy in wider clinical practice.
Methods: This was a prospective nationwide case-control study, nested within the cohort of all ERCP procedures performed in sweden, with- or without SpyGlass cholangioscopy, and registered in the GallRiks database, between 2007 and 2012. Data collected included variables such as patient characteristics, indication, therapeutic measures and, as primary outcome, adverse events. Descriptive statistics were used to characterize data. Multivariable logistic regression was used to analyse the impact of SpyGlass compared to conventional ERCP on complications. The effects of analyzed variables were presented as odds ratios with 95% confidence intervals. Ethics approval was obtained from the Regional Research Ethics Committee at Karolinska Institutet Stockholm.
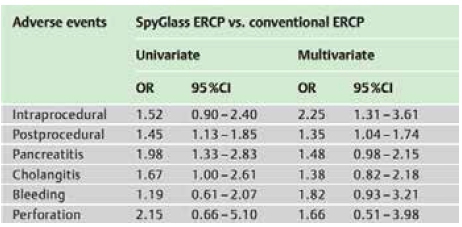
Results: Data from 36,352 ERCP procedures were analyzed including 408 SpyGlass procedures. Postprocedural adverse events were more prevalent when the SpyGlass technique was used (19.1% vs. 14.0%). Pancreatitis (7.4% vs. 3.9%) and cholangitis (4.4% vs. 2.7%) were adverse events elevated in the SpyGlass group. However, in the multivariate analysis the risk of intra- and postprocedural adverse events were significantly increased in the SpyGlass groups. The risk of pancreatitis and cholangitis, when adjusted for confounders, were not.
Recommendations: The SpyGlass technique is an advanced technique for intraluminal visual inspection and therapeutic intervention of the biliary and pancreatic ducts. There is a significantly increased risk for intra- and postoperative adverse events as well as of pancreatitis. Thus, this technique should preferably be used at tertiary centers in carefully selected cases.
RESECTION OF COMPLEX PANCREATIC INJURIES: ANALYSIS OF COMPLICATIONS USING THE ACCORDION CLASSIFICATION
K Mentor, J E J Krige, U K Kotze, P H Navsaria, A J Nicol, S R Thomson, E Jonas
Department of Surgery, University of Cape Town Health Sciences Faculty, Surgical Gastroenterology and HPB Unit, and Trauma Centre, Groote Schuur Hospital, Observatory, Cape Town, South Africa.
Background: Pancreatic injuries are uncommon but may result in substantial morbidity and mortality if inappropriately treated.
Aim: Severity of complications was assessed in patients undergoing resection for severe pancreatic injuries using the expanded Accordion Severity Grading System (ASGS).
Method: All patients who underwent a pancreatic resection for complex pancreatic injuries from 1990 to 2015 were reviewed using a prospective institutional database. AAST injury grades, type of pancreatic resection, need for damage control laparotomy and incidence and ASGS severity of complications was assessed. Validated international pancreas-specific complication grading and definitions were used.
Results: One hundred and thirty patients with AAST grade 3, 4 or 5 pancreatic injuries underwent a pancreatic resection (pancreaticoduodenectomy n=20, distal pancreatectomy n=110), 30 of whom had an initial damage control laparotomy (DCL) and later definitive surgery. Overall 238 complications occurred in 95 (73%) patients of which 73% were ASGS grades 3-6 and resulted in a significantly LOS. Those with no post-operative complications (grade 0, n=35) had a median 9 (range: 5-58) day post-resection hospital stay. Three patients with grade 1 complications (n=3) spent 14, 23 and 34 days in hospital, grade 2 (n=14, median 22, range 6-94 days), grade 3 (n=17, median 24, r 9-58 days), grade 4 (n=40, median 33, r 7-255 days), grade 5 (n=2, 9 and 19 days) and grade 6 (n=19, median 14, r 1- 52). Thirty-six pancreatic complications (fistulas n=24, fluid collections n=8, pseudocysts n=2) occurred in 33 patients and required endoscopic and percutaneous intervention in those that persisted. Fifty-eight (44.6%) patients required a repeat laparotomy (25 for definitive intervention after DCL, 16 for sepsis, 10 for bleeding, 7 for bowel obstruction). Nineteen patients (14.6%) died.
Conclusion: This study accurately benchmarked institutional postoperative morbidity after pancreatic resection for trauma. An increasing ASGS complication severity grade led to escalating intervention and prolonged hospitalisation.
PREVALENCE OF ADENOCARCINOMA OF THE OESOPHAGUS IN TWO TEACHING HOSPITALS IN GAUTENG PROVINCE, SOUTH AFRICA.
K Singh1, A Mannell2, D Bizos2, M Hale3
1 Department of Surgery, Postgraduate Surgery Registrar, University Of Witwatersrand
2 Department of Surgery, Faculty of Health Sciences, University of Witwatersrand, Johannesburg, South Africa
3 Department of Anatomical Pathology, National Health Laboratory Services
Introduction: Oesophageal carcinoma is the eight most common cancers worldwide and sixth most common cause of cancer related mortality6. The incidence varies markedly between race, age, and geographic region, environmental and nutritional factors. In western populations carcinoma of the oesophagus is uncommon whereas endemic areas include China, India, Iran, Russia and South Africa2. The incidence of oesophageal adenocarcinoma has rapidly risen over the past decades however squamous cell carcinoma of the oesophagus remains the most common worldwide1. The prevalence of oesophageal carcinoma is high in South Africa and contributes significantly to the burden of disease. These carcinomas remain asymptomatic during much of their development and once diagnosed is usually at an advanced stage. Hence prevention of carcinogens, exposure to risk factors, education and early detection methods can significantly reduce this burden6. The prevalence of squamous cell carcinoma is greater than that of adenocarcinoma of the oesophagus however no recent data is available thus this study is to evaluate what is currently presenting to our institutions.
Aim(s):
• To compare the demography and prevalence of patients who presented to Witwatersrand Academic Hospitals and were diagnosed with adenocarcinoma of the oesophagus.
• Compare the proportion of adenocarcinoma and squamous cell carcinoma of the oesophagus.
• How many of the patients with adenocarcinoma of the oesophagus underwent resection.
• To determine how often is concomitant Barrett's metaplasia is present in resected specimen.
Methods: Ethical approval M140301. Retrospective study using the NHLS database at CMJAH and CHBAH during 01/01/2001- 31/12/2013. Demographic variables include: Age, gender, and population group ( not specifically recorded).
Results: The prevalence of oesophageal carcinoma in our two teaching hospitals was on a downward trend. There was a significant decrease noted in the SCC subtype. The ACC subtype prevalence was on an upward trend. The results we experienced were consistent with worldwide trends.
Conclusion/Recommendations: This study is showing trends in keeping with western populations. Progress to education and screening to that of western populations is the way forward.

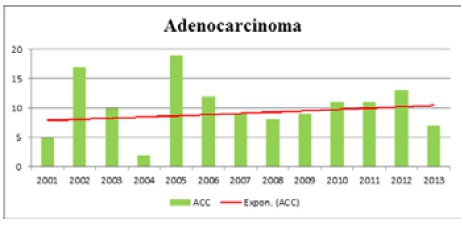
OPERATIVE INTERVENTIONS AT A REGIONAL BURN SERVICE: NOT ENOUGH
L C Naidoo, N L Allorto, D L Clarke
Edendale Hopsital, Pietermaritzburg Metropolitan complex Department of general surgery, University of Kwa-Zulu Natal
Introduction: We have used audit as an ongoing tool for quality improvement of burn care in our institution. Edendale Hospital faces limited resources and infrastructure, so we have chosen to focus on system enhancement. We identified time to first operative intervention as a quality marker, aiming to use this to benchmark our service.
Aim: To determine whether our surgical intervention is in keeping with international standards of care.
Methods: We interrogated the Edendale Hospital burn registry (BCA 106/14) for the months July 2015 to January 2016 as a retrospective analysis of all admissions. Data reviewed was age, total body surface area burned, length of stay, mortality, time to first operative intervention, what operation was done and graft loss using Microsoft Excel. Descriptive statistics were done.
Results: There was a total of 235 admissions, 140 children and 90 adults. Mortality rate was 7% (16 patients). The average total body surface burn admitted was 20%, with an average length of stay of 19 days. One hundred and forty-eight first operations were done (63% of admissions). The average time to first operation was 14 days. Debridement and complete grafting was performed in 94 patients (64%). Forty-eight (51%) patients had partial and six patients (6%) had total graft loss as a complication.
Conclusion: We are not achieving the standard of early excision with immediate and complete skin grafting within 7 days, as would be appropriate for our cohort where the average burn size in 20%. This is a deficit in our care. Limited theatre time as well as restrictions in post-operative care are some of the reasons for this. Late presentation accounts for some patients. Addressing this would result in reduced complications and we should focus on improving this.
AN ANALYSIS OF THE MORTALITY RATES OF ADULT SURGICAL PATIENTS ADMITTED TO THE INTENSIVE CARE UNIT OF A REFERRAL HOSPITAL IN BOTSWANA
L Makoba1, M Walsh2
1 Department of Emergency Medicine, Faculty of Medicine, University of Botswana
2 Department of Surgery, Faculty of Medicine, University of Botswana
Introduction: The outcome from complex surgery and critically ill surgical patients is dependent on a high standard of teamwork and critical care. To be able to improve the care delivered baseline information on outcomes is required so that targets for improvement can be identified.
Aim(s): To analyse the mortality rate of adult surgical patients admitted to the intensive care unit.
Methods: A retrospective chart review of all surgical patients admitted to the intensive care unit for the period 01/01/2016 to 31/12/2015 was performed. Information was obtained from the Intensive Care Admission Log. Referral was also made to the monthly surgical morbidity and mortality meeting records. Data collected included patient demographics, admitting specialty, diagnosis, length of stay in intensive care, survival and cause of death. Mortality rates were calculated for the whole surgical cohort and the surgical specialties.
Results: A total of 126 patient records were available. 79 (63%) were males and 47 (37%) females. 58 (46%) of the 126 surgical admissions died. The numbers of admissions, deaths and mortality rates are given in the table below.
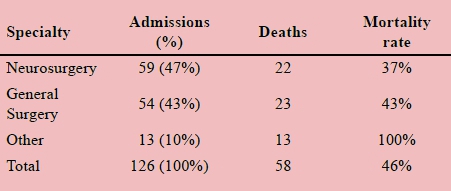
Conclusion/Recommendations: The mortality rate for surgical patients admitted to intensive care was 46%. This is high compared to international standards. Risk scoring was not possible on this data. Therefore an estimate of the number of possibly salvageable patients is not possible. To ensure improvements, in future outcomes for critically ill surgical patients, the surgical teams need to work closely with the intensive care team to identify areas for improvement. We also need to routinely collect data to enable risk scoring and audit of outcomes to be performed.
UPDATE OF NON-OPERATIVE MANAGEMENT OF PENETRATING KIDNEY INJURIES
C G Wiesinger1, L Roodt2, A Nicol2, S Edu2, P H Navsaria 2
1 Department of Urology, Klinikum Wels-Grieskirchen, Austria
2 Trauma Center, GrooteSchuur Hospital and Faculty of Health Sciences, University of Cape Town
Introduction and aim: Nonoperative management (NOM) of penetrating kidney injuries is slowly becoming more acceptable. In this study we review the current standard of care in penetrating kidney injuries in a high volume Level I Trauma Center in South Africa.
Methods: This study is a descriptive, non-interventional, observational study based on the retrospective analysis of data collected over a 11-month period [May 2015 - March 2016] from the electronic Trauma Health Record (e-THR) database (HREC (Ref no. R041/2014). All patients diagnosed with kidney injuries due to penetrating trauma [gunshot wounds (GSW), stab wounds (SW)] were analysed for demographics, injury mechanism, grade of renal trauma, perioperative management, nephrectomy rate and nonoperative success.
Results: There were 62 (17.61%) patients [mean age of 26.9 (13-45) years] with proven kidney injuries [40.32 % (n=25) SW, 59.67% (n=37) GSW] which were stratified for the American Association for the Surgery of Trauma grades (AAST) [grade I: 4.83% (n=3), grade II: 17.74% (n=11), grade III: 35,48% (n=22), grade IV: 33.87% (n=21), grade V: 8.06% (n=5)] and the injury mechanism. 20 (80%) renal injuries due to SW were managed nonoperatively without laparotomy with a success rate of 95% [delayed laparotomy in one patient (5%)]; 20% (n=5) underwent primary surgery but the kidney was not explored in 80% (n=4); nephrectomy was done in one patient (4%). 14 (37.8%) renal injuries due to GSW were managed nonoperatively without laparotomy with a success rate of 85.7% [delayed laparotomy in 14.3% (n=2)]; 62.1% (n=23) of GSW underwent primary surgery but the kidney was not explored in 47.8% (n=11); nephrectomy was performed in 8 patients (21.62%). Overall NOM failed in 8.8% (n=3) and nephrectomy was necessary in 2.94% (n=1).
Conclusion: NOM of penetrating injuries is a safe therapeutic strategy and is associated with a low nephrectomy rate.
NON-ACID GASTRO-OESOPHAGEAL REFLUX IS ASSOCIATED WITH SQUAMOUS CELL CARCINOMA OF THE OESOPHAGUS
M Kgomo 1, T R Mokoena2, J A Ker1
1 Department of Medicine, University of Pretoria
2 Department of Surgery, University of Pretoria
Introduction: Recent studies have consistently reported a significant association between gastric atrophy and oesophageal squamous cell carcinoma. However, causative factors responsible for this linkage remain to be elucidated. Squamous cell carcinoma of oesophagus (SCCO) is very common in SA. A study from Japan showed significant association between non-acid gastro-oesophageal reflux and SCCO. The suggestion is that non-acid oesophageal reflux may be a key factor linking gastric atrophy and SCCO.
Aim: This study sought to investigate the potential role of non-acid gastro-oesophageal reflux in the pathogenesis of SCCO in patients managed at Steve Biko Academic Hospital.
Method: A 24-hour pH-Impedance monitoring was undertaken on 33 patients with SCCO, following diagnostic oesophagoscopy and on 13 control patients with pathology other than SCCO.
Results: The age of the patients ranged from 27 to 85 years. Of the 33 patients with SCCO, 25 were found to have non-acid gastro- oesophageal reflux , and of the 8 negative for non-acid reflux, 4 had acid reflux and 4 were normal. Of the 13 control patients, 6 had non-acid reflux, 5 acid reflux and 2 were normal.
Conclusion: Although the study is in its infancy, preliminary results suggest that SCCO may be associated with non-acid reflux in a majority of our patient population. It could be speculated that prevention and treatment of non-acid reflux may reduce the incidence of SCCO in this group of patients.
The study continues to recruit a larger sample of patients to further validate this observation.
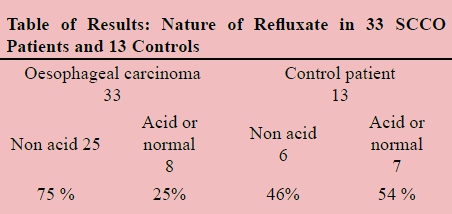
THE BURDEN OF GUNSHOT AND STAB INJURIES ON EMERGENCY GENERAL SURGICAL REFERRAL CENTRE
M Fleet, T Bottomley, R Stewart
Naewelezane Hospital, KwaZulu-Natal
Introduction: Voilence is a significant burden on health resources and society within South Africa. A major proportion present to emergency surgical departments in the form of gunshot wounds (GSW) and stab injuries. This study looks to highlight the magnitude of this burden on a trauma uniti in north KZN.
Aim: To quantify burden through the number and proportion of patients requiring surgical input secondary to stab or GSW in the form of review, CT investigation and operative intervention.
Methods: A retrospective study of emergency surgical reviews at Ngwelezane Hospital was conducted using daily admission reports between 1 December 2015 and 29 February 2016. The reports by admitting medical officers included patient demographics, investigations, diagnoses, and management. Patients that sustained any stab or GSW were identified. Admission and CT investigations were noted. Theatre logbooks were reviewed for patients then requiring operative intervention. Approval was obtained from the hospital ethics committee.
Results: Over the three month period a total of 1 260 patients required emergency surgial review. Of these, GSW and stab injuries accounted for 14.8% (187). Stab injuries were the most prevalent cause at 10.4% (131), of which 69.5% (91) were admitted, while 22.9% (30) required CT investigation and 17.6% (23) operative intervention. GSW reviews constituted the remaining 4.4% (56), of which 75% (42) were admitted, 51.8 % (29) required CT investigation and 25% (14) operative intervention.
Conclussion: Assult injuries in the form of GSW and stabs compromise a significan workload within emergency surgery.
Taking into account the likes of inpatient stay, investigations, interventions, materials and follow up, these accrue a major cost on health resources within KZN. In times of tight budgets and a drive to save on hospital spending, it is a clear primary prevention is paramoutn of alleviating this burden in the future.
PREDICTING THE FORREST GRADE IN PEPTIC ULCER DISEASE IN PATIENTS PRESENTING WITH UPPER GASTRO-INTESTINAL HAEMORRHAGE. WHAT INFORMATION ARE WE NOT OPTIMALLY UTILIZING?
M De Kock, N E Pearce
Department of Surgery, University of the Free State
Introduction: We hypothesized that patients presenting with upper Gastrointestinal (GIT) bleeding can be triaged for emergency scope based on routine investigations i.e. blood tests.
Aim and Objectives: Our aim was to establish if we can use baseline blood investigations to predict if the patient has got a significant risk of rebleeding (defined as a Forrest 1-2b).
Methodology: We designed a retrospective cross sectional study. 200 adult patients, seen at Universitas Hospital Referrals with a primary diagnosis of upper GIT bleeding, with complete data were included.
Results: The mean patient age was 55.6 years. Out of the 200 patients 88 patients had ulcers. (n=88/200 46%) The ulcer group had a mean Haemoglobin of 7.9mol/L, the non-ulcer group had a mean of 10,2mmol/L (p<0.0001). We found a haemoglobin value of <10.0mmol/L gave us a sensitivity of 75.0% and a specificity of 49.6% in its ability to determine whether a significant risk of rebleeding was present. The Urea values in the ulcer group had a mean value of 9.0 g/dL and the non-ulcer group had a mean value of 6.0g/dL (p=0.03662). We found a urea value of > 8.0g/dL gave us a sensitivity of 58.3% and a specificity of 65.6% in its ability to determine whether a significant risk of rebleeding was present. A low haemoglobin and high urea was compared to a high Rockall score (>3) and a clinical significance was found (p=0.00096 and p=0.0198 respectively).
Conclusion: After statistical analysis we found that by adding certain blood tests to patient workup we can improve our accuracy in predicting the patient's Forrest classification. We would like to prospectively validate our results in a follow up study.
OUTCOMES OF FCS (GENERAL SURGERY) FINAL EXAMINATIONS: PREDICTORS OF OUTCOME
M Kahn, P Navsaria, D Kahn
Division of General Surgery, Groote Schuur Hospital and University of Cape Town
Background and aim: An audit of the FCS (General Surgery) examinations has not been previously performed. The purpose of this study was therefore to review the results, and determine any predictors of outcome (pass or fail).
Methods: The results of the FCS (General Surgery) examinations, from October 2005 till September 2014, were retrieved from the College of Medicine of South Africa. The current format of the examinations consists of: two written essay question papers, an OSCE, two patient cases and two vivas. These were retrospectively reviewed and analysed. Predictors of failure or success were determined.
Results: During the 10-year study period, 472 candidates attempted the examinations. Of these, 84 (17.8%) were not invited to attend the oral examination. The overall pass-rate was 76.3% [296 / 388]. Nineteen candidates were invited to the orals despite failing both the written papers having achieved > 45% but < 50%. The failure rate in this group was 80% [15 failed]. There were eighty-eight candidates who passed one and failed one written paper. The failure rate in this group overall was 50%. Fortty-nine candidates failed the OSCE; and of these 40 (82%) failed overall.
Conclusion: Failing both written papers and failing one written paper resulted in 80% and 50% failure rate, respectively. Failing the OSCE examination was the highest predictor of overall failure at a rate of 82%.
ANTIBIOTIC PRESCRIPTION IN THE SURGICAL INTENSIVE CARE UNIT AT STEVE BIKO ACADEMIC HOSPITAL (SBAH)
I M Joubert1, J P Pretorius2, F Paruk2
1 Department of Surgery, Faculty of Health Sciences, School of Medicine, University of Pretoria.
2 Critical Care Unit, Department of Surgery, Faculty of Health Sciences, School of Medicine, University of Pretoria.
Introduction: Indiscriminate prescription of empiric antibiotic therapy and inappropriate use of antimicrobial prophylaxis contributes to the development of antimicrobial resistance. Inappropriate withholding of empiric antibiotic therapy can increase morbidity and mortality. Appropriate antibiotic prescription is important to ensure optimal clinical outcome and prevent antimicrobial resistance. Evaluating current prescription practices identifies problem areas to be addressed in formulating appropriate antibiotic usage guidelines.
Aims: The pattern of antibiotic prescription was evaluated by looking at:
• Percentage of patients receiving antibiotics as therapy or prophylaxis
• Antibiotics chosen empirically or based on microbial culture results
• Prophylaxis limited to 24 hours
• Correlation between prolonged stay, multiple antibiotic courses and mortality
• Correlation between antibiotic prescription and mortality
Methods: This is a retrospective descriptive study utilising data sheets on antibiotic prescription practices completed for all patients on discharge from the surgical ICU at SBAH from January 2011 to December 2014. ICU admission records were used to determine length of stay and survival until ICU discharge. Patients receiving antibiotics for tuberculosis treatment and pneumocystis jirovecii pneumonia prophylaxis and those younger than 18 years were excluded from the study. Ethical approval was obtained.
Results: Data from 201 patients analysed thus far. 79.6% of patients admitted to ICU receive antibiotics, the majority therapeutic. Nearly half received multiple antibiotic courses. Therapeutic antibiotics were prescribed empirically in 60%. Prophylaxis was prescribed for > 24 hours in 21%. Mortalities tended to be prescribed antibiotics more often, receive multiple courses of antibiotics and have a prolonged ICU stay.
Conclusion: Antibiotics are commonly prescribed in the ICU. An unacceptably high number of patients receive antimicrobial prophylaxis for > 24 hours. There appears to be a correlation between receiving multiple antibiotic courses, prolonged ICU stay and mortality. This could point to nosocomial infection with resistant microorganisms contributing to mortality and emphasises the need for appropriate antibiotic prescription.
NOVEL, SAFE TECHNIQUES IN IMMEDIATE BREAST RECONSTRUCTION, LOCALLY ADVANCED BREAST CANCER
M Venter, C A Benn
Breast Care Centre, Netcare Milpark Hospital, Johannesburg, South Africa
Background: Locally advanced breast cancer poses unique surgical dilemmas. Studies involving reconstruction are few, most units do not reconstruct immediately if local surgery is performed. In our unit we perform a two part surgery apart in order to facilitate immediate reconstruction in these patients.
Objective: To demonstrate that breast reconstruction is possible in advanced breast cancer.
Methods: A prospective study of patients with locally advanced breast cancer treated in our unit from October 2013 to January 2016. Patients with inflammatory breast cancer, extensive DCIS with invasion and nodal disease, unknown primary disease were included in the study. Standard oncological protocol for locally advanced breast cancer (primary chemotherapy) was observed. We evaluated the patient demographics, histological features, tumor biology, oncological and reconstructive procedures.
Results: 101 patients were referred to a single reconstructive surgeon during this period; 2 patients had bilateral breast cancer, 21% inflammatory cancers, 8% unknown primary, 37% multi-centric disease, 17% extensive DCIS , with invasive and nodal disease and 17% large tumors post primary chemotherapy. The average patient age was 47 years. All patients received radiation post-surgery. Chemotherapy protocols were initially decided in the MDM. The majority of patients underwent reconstruction to the affected breast with an opposite side matching procedure. The average duration of the first procedure was 25 min and the reconstructive procedure was 133 min. Surgery and reconstructive outcomes were evaluated photographically. More than 50% of patients had a complete histological response.
Conclusion: Breast reconstruction is possible in locally advanced breast cancer. The procedure allows for adequate histological assessment and clear margins prior to immediate reconstruction and facilitates a better cosmetic result. Advances in chemotherapeutic regimes have improved the survival of these patients and breast reconstruction improves their quality of life.
POST-OPERATIVE ANALGESIA: ARE PATIENTS RECEIVING ADEQUATE COVER?
K Masehla, S Mkhwanazi, R Mokhothu, R Molehe, K Motiang, M Mpe, N Mshayisa, M Mukoma, T Mushosho, Y Nokwe, K Ntjana, N Ntshangase, C Phiri, K Tambudze, T E Luvhengo
Department of Surgery; University of the Witwatersrand
Introduction: Adequate post-operative pain control is imperative to the recovery of patients.
Aim: This research investigated whether patients are receiving adequate post-operative analgesia.
Methods: This prospective study was conducted over one month on adult patients who were within 48 hours post-operative at CHBAH and CMJAH. Data collected included patients' demography, types of operations, nature of anaesthesia and type of analgesia. The Universal Pain Assessment Tool was used to compare pain before and after administration of post-operative analgesia. Only patients who had elective procedures were included and patients with diminished level of consciousness were excluded. Permission to conduct the study was received from HREC of University of the Witwatersrand.
Results: A total of 153 patients were studied, of which 70 were at CHBAH and 83 at CMJAH. Majority were females (62.8%). Their average age was 38.5 (range: 18-60 years). Most of the operations were general surgical procedures (41.8%) and orthopaedics (36.6%), with others accounting for 21.67%. Majority (79.1%) were performed under general anaesthesia. A combination of tramal and paracetamol was the preferred type of post-operative analgesia in 30.7%.
The average pain scores before and after analgesics were 6.39 and 2.84, respectively. ANOVA parametric test for inequality was used to compare the scores and the p-value of 0.00001 was found. The p-values were the same irrespective of analgesic type. The difference in average pain scores before and after analgesia was higher in females compared to males, but was not statistically significant (p<0.1048).
Conclusion: Patients in both hospitals are receiving adequate post-operative analgesia irrespective of analgesic type. Average pain difference was highest after urological and least after gynaecological operations.
ORGANIZED TRAUMA SYSTEMS AND DESIGNATED TRAUMA CENTERS FOR IMPROVING OUTCOME IN THE INJURED, TREND OF PRIMARY STUDIES.
M Mwandri1,3, B Stewart2, T Hardcastle3,4, A Rubiano5, J Alarcon6, J Puyana7, R Gruen8
1 Department of Surgery, Temeke Municipal Hospital, Dar Es Salaam, Tanzania
2 Department of Surgery, University of Washington, Seattle, Washington, USA
3 Department of Surgery, University of Kwazulu-Natal, South Africa
4 Trauma Service and Trauma ICU, Inkosi Albert Luthuli Central Hospital, Malvern, Durban, South Africa
5 MEDITECH Foundation, Neiva, Colombia
6 Iberoamerican Cochrane Network. IIB-Sant Pau. Surcolombian University, Barcelona, Spain
7 Surgery and Critical Care Medicine, University of Pitssburgh Medical Center, Pittsburgh, Pennsylvania, USA
8 Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore, Singapore
Introduction: Several studies report reductions in the burden of injury and improvements in injury care after the creation of a trauma system. Successful trauma systems in the United States have not been widely replicated in other regions, particularly in low-middle income countries (LMICs). The lack of support for trauma system in LMICs may be, in part, due to the dearth of evidence for their effectiveness in low-resource settings. A quality evaluation of trauma system effectiveness could inform health policy and resource allocation decisions and ultimately lead to improved care for the injured.
Aim: To assess the effects of trauma systems and designated trauma centers by systematically reviewing available evidence for their effectiveness.
Methods: This is a Cochrane review under the Effective Practice and Organization of Care (EPOC) group. A search strategy was developed and included Cochrane Central Register of Controlled Trials, MEDLINE, Embase, CINAHL, EbscoHost, and DOAJ, grey literature and trial registries. We included Randomized Control Trials (RCTs), non-RCTs, Controlled-Before-After (CBA) and Interrupted Time Series(ITS), comparing trauma and non-trauma systems caring for adults and pediatric patients with injury severity score >15. We excluded fragility fractures. Two authors independently screened studies at title, abstract and full-text levels, the third author intervened where there was disagreement.
Results: Final search yielded 4453 studies, 4290 were excluded at title/abstract level. Among 163 full-text studies reviewed 41% are observational, 23% before-after studies (without control group), 19% ITS, 16% CBA and 1% non-RCT.
Conclusion/recommendation: About only 36% of all research on the effectiveness of trauma systems provide primary studies for high quality evidence as defined by the EPOC group. Exposing fundamental deficiencies in designing primary trauma research will entice robust research in trauma surgery.
AN INVESTIGATION OF DIVERTICULAR DISEASE AMONG AFRICAN PATIENTS UNDERGOING COLONOSCOPY AT DR. GEORGE MUKHARI ACADEMIC HOSPITAL
M Vally, M Z Koto, M Govender
Department of General Surgery, Sefako Makgatho Health Sciences University (SMU)
Introduction: Diverticular disease was previously thought to be non-existent in the African population. Previous studies over the past four decades, however, have shown a steady increase in the prevalence of the disease. There has not been any recent data describing diverticular disease in South Africa for over twenty years.
Aim(s): The aim of this study was to report on the profile and current prevalence of diverticular disease in the African population at Dr. George Mukhari Academic Hospital.
Methods: A retrospective descriptive study was performed of African patients who were diagnosed with diverticular disease on colonoscopy between 1 January and 31 December 2015. Inclusion criteria were adult black African patients diagnosed with Diverticular disease on colonoscopy. Exclusion criteria were non-black patients and patients with incomplete colonoscopies. Date was collected from colonoscopy reports which described demographics, indications for colonoscopy and findings. Data was analysed and presented descriptively. Ethical approval was obtained from SMU research ethics committee.
Results: Out of 348 colonoscopies eligible for inclusion in this study, 47 patients were diagnosed with diverticular disease with a prevalence of 13.5% (95% CI: 10.3% - 17.5%). The highest number of patients diagnosed was in their seventh and eighth decades with a range between 46-86 years, (mean 67 years). There was a female to male predominance of 57.45% to 42.55% respectively. Lower gastrointestinal Bleeding was the commonest (65.96%) indication for colonoscopy. The Left colon was most commonly involved (72.34%) followed by the right colon (55.31%). A significant number of patients had pancolonic involvement (27.65%).
Conclusion/Recommendations: This retrospective study suggests that there has been a significant increase in the prevalence of diverticular disease among black Africans in a South African cohort. This is likely due to changes in dietary habits and socio-economic status. Diverticular Disease should no longer be considered rare in African patients.
CAUSES, INCIDENCE AND OUTCOMES OF VASCULAR TRAUMA TO THE EXTREMITIES AT DR. GEORGE MUKHARI ACADEMIC HOSPITAL
N Singh1, Z Koto2, N Cloete3
1 Department of General Surgery, Sefako Makgatho Health Sciences University
2 Department of General Surgery, Sefako Makgatho Health Sciences University
3 Department of General Surgery, Vascular Unit, Sefako Makgatho Health Sciences University
Introduction: The public health sector in South Africa is burdened with an array of traumatic injuries, which demand considerable resources. Vascular injuries of the extremities require special consideration because they can be threatening to both limb and life. These injuries are seen regularly at Dr. George Mukhari Academic Hospital (DGMAH) but the incidence is not known.
Aim: To describe the causes, incidence and outcomes of vascular trauma to the extremities at DGMAH
Methods: This is a cross sectional observational study. Hospital records of patients presenting to DGMAH between 01/03/2012 and 28/02/2016 with peripheral vascular trauma requiring surgical intervention were reviewed retrospectively and the necessary data was collected using a proforma. Iatrogenic injuries were excluded. Local ethics approval was obtained.
Results: 48 patients were identified. 93.8% were male with a mean age of 30 (range 16-56). Mechanism of injury was penetrating in the majority of cases with 45.8% (22/48) from stabs or cuts and 41.7% (20/48) from gunshot wounds. Blunt trauma accounted for 6 cases. Both the upper and lower limbs had an equal incidence of injury. The limb salvage rate was 89.6% (43/48). There were no mortalities however morbidity secondary to associated nerve injury occurred in 18.6% (9/48).
Conclusion/Recommendations: The results presented in this series are in keeping with national standards and trends. Vascular injuries to the extremities need to be managed by a multidisciplinary team due to associated injuries that may impair functionality of the preserved limb.
ETIOLOGY OF PORTAL HYPERTENSION AT DR. GEORGE MUKHARI ACADEMIC HOSPITAL
N Singh1, M Govender2
1 Department of General Surgery, Sefako Makgatho Health Science University
2 Department of General Surgery, Hepatobiliary Unit, Sefako Makgatho Health Science University
Introduction: The etiology of portal hypertension varies in different parts of the world with cirrhosis being reported as the most common cause reaching approximately 80% in the west. Schistosomiasis, on the other hand, is report it to be the most common cause in areas endemic to this parasite. Treatment and prognosis of portal hypertension are dependent on etiology thus compelling us to understand the disease pattern in our environment.
Aim: To describe the etiology of portal hypertension in patients managed at Dr. George Mukhari Academic Hospital (DGMAH).
Methods: This is a retrospective observational study. All patients with portal hypertension treated by the Hepatobiliary Unit at DGMAH during the period November 2013 till December 2015 were included. Data collected comprised of patient demographics, alcohol history, viral hepatitis and schistosomiasis blood results, special investigation results and final etiological diagnosis.
Results: 47 patients with portal hypertension were identified, 29 male and 18 female with a mean age of 39.3 years. The most common etiology was schistosomiasis 16/47 (34%) followed by cryptogenic cirrhosis 9/47 (19%). Portal vein thrombosis and Hepatitis B liver cirrhosis had an equal prevalence of 12.8% (6/47) each. 1 patient tested positive for both schistosomiasis and Hepatitis B. Other causes included Alcoholic cirrhosis, 10.6% (5/47), splenic vein thrombosis 6.4% (3/47) and 1 case of Klippel-Trenaunay Syndrome.
Conclusion/Recommendations: Although this is a small series, Schistosomiasis is the most common cause of portal hypertension in our environment. Public health awareness is recommended as an attempt to decrease the number of new cases.
CRUSH SYNDROME AND ACUTE KIDNEY INJURY (AKI) AT THE DR GEORGE MUKHARI ACADEMIC HOSPITAL (DGMAH)
N Kumar, O Y Matsevych, M Z Koto, L D Mashego
Trauma Unit, Department of General Surgery, Sefako Makgatho Health Science University, Dr George Mukhari Hospital, Pretoria
Introduction: Crush (myonephropathic) syndrome is a frequent cause of AKI in South Africa. Varying values of serum creatinine kinase (CK) exist in the literature as predictive for the development of AKI.
Aim: To identify prognostic markers for the development of AKI, progression to dialysis and mortality in patients presenting with crush injury.
Methods: Data was collected prospectively on a proforma from January 2014 to December 2015. All patients presenting to DGMAH trauma unit with crush injury and a CK value > 500 U/L on admission were included in the study. All patients with a CK < 500 U/L on presentation were excluded. Data collected included patient demographics, CK levels, serum creatinine and arterial blood gas values. Renal failure was defined as per the RIFLE criteria. Multivariate analysis was
done using IBM SPSS Statistics 22 software.
Results: A total of 255 patients were included in the study of which 96.9% were males. CK level on admission > 9000U/L was predictive of progression to dialysis (p<0.05). CK level on day 1 > 10,000U/L correlated with the development of AKI (p<0.05). The development of AKI also correlated with pH on admission of < 7.2, bicarbonate level on admission of < 17, Shock Index (SI) > 0.9 and Injury Severity Score (ISS) > 15 (all p values <0.05). Correlations with mortality were noted with a CK level > 10,000 U/L, ISS > 22, SI > 0.9 and the presence of a traumatic brain injury (all p values <0.05). No significant correlations were noted between lactate levels and potassium levels and the development of AKI.
Conclusion: CK, pH and bicarbonate can be used as markers for the development of AKI. CK, SI and ISS have predictive value for both AKI and mortality. CK is a marker for progression to dialysis.
THE CONSEQUENCES OF MAJOR VISCERAL VASCULAR INJURIES ON OUTCOME IN PATIENTS WITH PANCREATIC INJURIES: A CASE-MATCHED ANALYSIS
N B Leech1, J E J Krige1, U K Kotze1, A J Nicol2, P H Navsaria2, E Jonas1
1 Departments of Surgery, University of Cape Town Health Sciences Faculty, Surgical Gastroenterology and HPB Unit
2 Trauma Centre, Groote Schuur Hospital, Observatory, Cape Town, South Africa
Introduction: Major pancreatic injuries are among the most complex of the intra-abdominal solid organ injuries to treat, especially when combined with vascular and adjacent organ injuries.
Aim: This study assessed the influence of associated vascular injuries in pancreatic injuries on outcome in a case-matched analysis.
Method: The study design was a case-matched comparative analysis using a faculty approved and registered prospective database of 461 consecutive patients with pancreatic injuries. Sixty-eight patients with a pancreatic injury combined with a major visceral vascular injury (PIVI group) were identified and manually matched one-to-one to 68 similar pancreatic injury patients without a vascular injury (PI group) by an independent blinded reviewer using a validated individual matching method. The two groups were compared using univariate and bivariate logistic regression analysis to assess significance at p<0.05. The main measures and outcomes were complication rates, hospital stay length, and 90 day mortality rate.
Results: The two groups were matched according to surgical intervention (pancreatoduodenectomy n 10+10=20, distal pancreatectomy n 16+16=32, non-resection n 42+42=84), mechanism of injury and AAST injury grade. The PIVI group had sustained injuries to IVC n=39, renal A+V n=17, SMA+V n=9, portal vein n=7, aorta n=7, splenic A+V n=7. Mortality in the PIVI group was 41% compared to 13% in the PI alone group. On univariate analysis the PIVI group were significantly more likely to be (i) shocked on admission, (ii) have a RTS <7.8, (iii) require damage control surgery, (iv) require a blood transfusion, both in frequency and volume, (v) develop a major postoperative complication and (vi) die. On logistic regression analysis, the need for damage control surgery was a significant variable (p=0.015, OR 7.95, CI 1.50-42.0).
Conclusion: Despite rapid operative intervention, pancreatic injuries associated with major visceral vascular injuries had a significantly higher complication and mortality rate.
DOES A HIGH PREVALENCE OF HELICOBACTER PYLORI IN PATIENTS WITH PEPTIC ULCER DISEASE AT CHARLOTTE MAXEKE JOHANNESBURG ACADEMIC HOSPITAL JUSTIFY EMPIRIRIC H.PYLORI ERADICATION?
N T Sishuba1, A Mahomed2, G Candy1, T E Luvhengo1
1 Department of Surgery, University of the Witwatersrand
2 Department of Internal Medicine Pathology; University of the Witwatersrand
Introduction: Helicobacter pylori infection is a major risk factor for peptic ulcer disease. Empiric eradication therapy is justified in areas where prevalence of infection is high.
Aim: To determine if empiric eradication therapy in patients presenting with PUD at CMJAH is justifiable.
Methods: Records of patients who had upper GIT complaints and had upper GIT endoscopy in the Endoscopic Unit of CMJAH between 1st October 2012 and 31st December 2012 were reviewed. Patients who had previous gastric operations, interventional endoscopy, confirmed or suspected malignancy and incomplete endoscopy were excluded. Data collected included patients' demography, indication for endoscopy, endoscopic findings, and histology results including H.pylori status. Permission to conduct the study was received from Wits HREC (M130668)
Results: 311 records were found of which 91.6% (285/311) were diagnostic but only 196 met inclusion criteria. The mean age in years of included patients was 52.5 +/- 16SD. The commonest endoscopic diagnosis was gastritis (35%) and peptic ulcer was diagnosed in 30% of the patients, and 45% of the ulcers were complex. H.pylori testing was performed in 74% of the records and H-pylori positivity was more prevalent in individuals below 20 years regardless of endoscopic diagnosis. Prevalence of H.pylori infection in endoscopically diagnosed PUD patients was 50% for DU and pyloric channel ulcers, and 47% for GUs. H-pylori was more prevalent in females (67.0%) with PUD compared to males (32.6%).
Conclusion: Less than 50% of patients who have PUD and presenting at CMJAH test positive H.pylori therefore empirical eradication therapy is not justified.
WHAT IS THE CLINICOPATHOLOGICAL SPECTRUM OF LOCALLY ADVANCEC COLORECTAL CANCER IN KWAZULU-NATAL TEACHING HOSPITAL?
N Manzini1, T E Madiba2
1 Department of General Surgery, Ngwelezane Hospital
2 Emeritus Professor, Department of General Surgery, University of KwaZulu-Natal
Introduction: Colorectal cancer is the second leading cause of cancer-related deaths in the world. Locally advanced colorectal cancer has been a challenge to treat due to its high recurrence rate.
Aim: To document presentation, staging, management and outcome of patients with locally advanced colorectal cancer
Method:
• Setting: Colorectal unit in a tertiary Hospital
• Design: Retrospective analysis of prospectively collected data for patients with locally advanced colorectal cancer.
• Data collected were demographics, clinical presentation, staging, management and outcome.
• Ethical approval: (E198/04).
Results: Of 1449 patients with colorectal cancer, 693(48%) patients had locally advanced colorectal cancer. Mean age was 57.96+15.5 years. Median ages for Africans, Indians, Coloureds, and Whites were 50, 62, 62.5 and 67 years respectively.
One hundred and two (25%) of patients presented at the age of < 40 years [76(31.8%) Africans, 20(6.9%) Indians, 4 (3.9%) Coloureds and 2(2%) Whites]
Colonic cancer occurred in 126(18%) patients, with 34.9% and 65% involving the proximal and distal colon respectively. Eighty nine (70, 6%) patients received resection while 37 (29%) did not. Thirty patients have been confirmed dead.
Rectal cancer was seen in 567(81.9%) patients. A total of 326(57.5%) received resection and 239 (42%) did not have surgery. Resection was preceded by neo-adjuvant therapy in 238(41%) and 126(22%) received adjuvant therapy. Seventy three (13%) received palliation and 127(22%) did not receive oncological treatment. One hundred and twenty (21%) five patients have been confirmed dead.
Conclusion: Locally advanced colorectal cancer is common in our setting. More young patients are seen with colorectal cancer. Rectal cancer is more common and is associated with higher mortality.
LAPAROSCOPY FOR BLUNT ABDOMINAL TRAUMA: A CHALLENGING ENDEAVOR
O Y Matsevych, M Z Koto, M Balabyeki, D Mashego
Department of Surgery, Dr George Mukhari Academic Hospital, Sefako Makgatho Health Sciences University
Introduction: Diagnostic and therapeutic laparoscopy is safe and effective in management of penetrating abdominal trauma. However, laparoscopic management of blunt abdominal trauma is still rarely used. There is paucity of data in the literature.
Aim: Our aim was to analyze our experience with laparoscopy for blunt abdominal trauma and to compare the converted to laparotomy and laparoscopic groups.
Methods: The prospectively collected records of all patients managed with laparoscopy for blunt abdominal trauma from January 2012 to December 2015 were retrospectively reviewed. Patients with primary laparotomy, missing records were excluded. The patients' age, mechanism of injury, trauma scores, laboratory results, intraoperative findings, outcomes and length of hospital stay were analyzed in laparoscopic and converted to laparotomy groups. The study was approved by our institutional ethical committee.
Results: Thirty five patients were included into the study. Eight (23%) patients were converted to laparotomy. Out of 27 patients in laparoscopy group 13 (48%) patients had diagnostic laparoscopy and 14 (52%) patients had therapeutic laparoscopy. Twenty patients were assaulted, 14 were involved in MVA and one patient fell from the height. The mean ISS was 12.25 in converted group and 11.3 in laparoscopic group. There were no significant difference in initial haemodynamic or metabolic values, length of hospital stay and complication rate between the two groups. No complications were recorded in 29 patients, four patients suffered Clavien-Dindo grade 3 complication and two patients had grade 5 complication. The higher ISS score was related to the higher rate of complications.
Conclusion: Laparoscopy for blunt abdominal trauma remains a challenging approach. It is feasible and safe in expert hands. However, the conversion rate is high and it is difficult to identify preoperatively any markers leading to conversion. The expertise and clinical judgment are the cornerstones of selecting appropriate management.
DIAGNOSTIC LAPAROSCOPY VERSUS NON-OPERATIVE MANAGEMENT IN PENETRATING ABDOMINAL TRAUMA: A RETROSPECTIVE COMPARISON
O Y Matsevych, M Z Koto, M Balabyeki, D Mashego
Department of Surgery, Dr George Mukhari Academic Hospital, Sefako Makgatho Health Sciences University
Introduction: Selective nonoperative management (NOM) of penetrating abdominal trauma (PAT) is successfully practiced for more than 30 years. Diagnostic laparoscopy is currently used more frequently in the setting of PAT and it helps to avoid nontherapeutic laparotomy in 36%. These two approaches were not compared in the literature. The aim of our study was to compare primary diagnostic laparoscopy to NOM approach in the setting of PAT.
Methods: The prospectively collected data were retrospectively analyzed. Patients with PAT who were successfully managed nonoperatively or with diagnostic laparoscopy from January to December of 2015 were included into the study. Patients who failed NOM or converted to laparotomy were excluded. The patients' age, mechanism and location of injury, trauma scores and outcomes were compared in two groups. The Fisher exact test and t-test were used to calculate p-value. The study was approved by the institutional ethical committee.
Results: Thirty five patients in laparoscopy group and 36 in NOM group were analyzed. The laparoscopy group had a higher ISS (6.8 versus 5.08) but had less CT scans done (17.1% versus 75%). More patients with stab wounds underwent laparoscopy (85.7% vs 52.8%). Eleven patients in laparoscopy group had pneumothorax (11 versus 2) and eight of them underwent thoracoscopy. Two patients had iatrogenic injuries during laparoscopic dissection which were successfully managed laparoscopically. No serious postoperative complications were recorded in both groups. The hospital stay was longer in laparoscopy group (3.1 versus 2).
Conclusion: Primary laparoscopy is a safe alternative to NOM for PAT. It accurately visualizes intraabdominal injuries, selects patients for therapeutic procedures, protects patients from radiation exposure and avoids nontherapeutic laparotomies. Although after diagnostic laparoscopy a surgeon sleeps better, the patient may stay in hospital longer. More studies are needed to establish the role of primary laparoscopy as an alternative to NOM of PAT.
T-LYMPHOCYTE IMMUNE SUBSETS PROFILE AS A PREDICTOR OF SURVIVAL IN PATIENTS PRESENTING WITH BREAST OR OESOPHAGEAL CANCER
O O Wedi1,3, R Cockeran1, C Durandt1, V Moodly2, T Mokoena3
1 Department of Immunology, University of Pretoria, South Africa
2 Department of Hematological Pathology, University of Limpopo, South Africa
3 Department of Surgery, University of Pretoria, South Africa
Introduction: In recent years the host T-cell immune status has been implicated in the development and eradication of cancer. It has been suggested that alterations in the T-cell immune profile may serve as a prognostic factor in the management of cancer patients.
Aim: This study sought to investigate the prognostic value of CD4+ and CD8+ Treg and non-Treg T-cell subsets in patients presenting with breast or oesophageal cancer in an African setting.
Experimental design: Venous blood was obtained from consenting adult patients with histologically proven cancer; 25 with breast carcinoma and 10 with oesophageal squamous cell carcinoma, before initiation of anticancer treatment and at day 1 post-treatment. The absolute numbers and percentages of circulating CD4+ and CD8+ non-Treg and Treg T-lymphocytes subsets were determined at both time points. The T-cell immune profiles were compared in patients who survived and those who died at 7 weeks post receipt of anti-cancer treatment.
Results: Patients who survived displayed a higher CD4: CD8 T-cell ratio (2.2 vs. 1.2; p= 0.044) before treatment, and a higher CD4+ (390 cells/μl vs. 111 cells/μl; p=0.0046) and CD8+ (160 cells/μl vs. 88 cells/μl; p=0.058) T-cell count at day 1 post treatment. Patients who survived also displayed a higher CD8+CD25+CD127+ Treg cell percentage (28.42% vs. 15.24; p=0.019) before treatment, higher CD4+CD25+CD127+ Treg cell count at day 1 post-treatment (9 vs. 2; p= 0.047) and higher CD8+ Treg: total CD8+ T-cell ratio (1.48 vs. 0.53; p=0.0126) before treatment.
Conclusion: The circulating T-cell immune profile may serve as a feasible and reliable method of identifying patients at high risk of death during the early post-treatment period. A study with larger patient sample is necessary to validate these preliminary findings.
OUTCOME AND SEVERITY OF SURGICAL PATIENTS ADMITTED TO A NON-TERTIARY MULTIDISCIPLINARY CRITICAL CARE UNIT
0 Swart1,2, R C Duvenage1,2
1 Department of General Surgery, Worcester Hospital
2 Ukwanda, Rural Clinical School, Stellenbosch University
Introduction: Demand for critical care services exceeds availability. Limited published public health sector Critical Care Unit (CCU) data, outside of academic institutions, is available. Worcester Provincial Hospital's (WPH) 5-bed multidisciplinary open CCU is classified as a high care unit (HCU) and services a rural population of approximately 600 000 in the Cape Winelands East and Overberg district of the Western Cape.
Aim(s): To describe the severity and in-hospital all-cause mortality of surgical patients admitted to the WPH CCU.
Methods: A descriptive study of all surgical patients admitted to WPH CCU from Jan - Dec 2014. Data regarding pathology, severity (Apache II), organ failure and outcome were prospectively collected. Statistical analysis was done in STATA v13.1. Ethical approval was obtained from Stellenbosch University Health Research Ethics Committee (#N14/09/124).
Results: The WPH CCU had 114 (8 re-admissions) surgical admissions out of a total of 610 during 2014. The mean (standard deviation) age and median length of stay were 46.0 (SD 18.7) years and 2 (range 0.5-13.5) days respectively. The mortality rate was 17.0% (18/106) with a mean Apache II score of 10.9 (SD 6.5). 68.4% (78/114) of admissions required ventilatory support with 156 ventilation and 67 CPAP days. 28.9% (33/114) required both ventilation and inotropic support (total of 70 inotrope days) indicating multi-organ failure. Only 18.9% (20/106) of patients were referred to a tertiary CCU.
Conclusion/Recommendations: Disease severity and mortality were similar to the only non-tertiary, although non-surgical, CCU data published. Almost a third of the CCU admissions had multi-organ failure that is deemed to be beyond the scope of a HCU.
THE VALUE OF NEUTROPHIL LYMPHOCYTE RATIO (NLR) IN THE DIAGNOSIS OF ACUTE APPENDICITIS
P Asafo-Adjei, T E Luvhengo, G P Candy
Department of Surgery, University of the Witwatersrand.
Introduction: White cell count (WCC) and C-ractive protein (CRP) are of limited value in the early detection of acute appendicitis (AA). The neutrophil lymphocyte ratio (NLR) has been proposed as a novel cost effective marker that could play this role.
Aim: To evaluate reliability of NLR in the diagnosis of acute appendicitis in the African setting
Methods: Retrospective review of recalls of patients treated for AA from January 2003 to June 2015. Data retrieved included patients demography, pre-operative WCC, differential counts, CRP and appendix histology. NLR was calculated for each patient. ROC curves were used to determine the cut-off value for each test. Sensitivity, specificity, PPV and NPV were calculated. Permission to conduct the study was the Human Research Ethics Committee of University of the Witwatersrand.
Results: 1098 records were found of which 590 were excluded. Majority were male (56.7%). Average age was 28. The cut off NLR value for the diagnosis of AA was 2.55 with sensitivity, specificity, PPV, NPV of 81.1%, 47.5%, 94.4%, 18.8% respectively. A WCC and CRP of 9.16 and 13 were diagnostic of AA with a sensitivity of 67.9%, specificity of 55.0%, PPV of 94.4%, NPV of 13.7% for WCC and 89.8%, 42.50%, 94.4% and 27.9% for CRP in the same order. An NLR of 4.94 differentiated complicated from uncomplicated AA while 10.09 was diagnostic of serosal AA. AUC for NLR, WCC and CRP were 0.662, 0.622 and 0.687 respectively.
Conclusion: Although NLR is less sensitive compared to CRP it is more specific for diagnosis of AA. A cut off of 4.90 differentiates complicated from uncomplicated AA.
LOWER EXTREMITY A MPUTATION AT NMAH: RISK FACTORS AND OUTCOME
S Z Molaoa, P Gaju
Department of Surgery, Walter Sisulu University and Nelson Mandela Academic Hospital
Introduction: Advances in surgical techniques and anaesthesia, and use of antibiotics have reduced the amputation related mortality. Amputation is the intervention of choice for fulminant diabetic foot sepsis, irreconstructable arterial disease, gangrene from chronic or acute arterial occlusion, trauma and malignancy. In our institution 125 emergency amputations were performed over a 24 months' period. However, risk factors and post-amputation outcome have not been determined.
Aim of the study: The purpose of this study, therefore, was to determine magnitude of limb loss in our patient population; risk factors; indications and the outcome of amputations at NMAH.
Methods: A retrospective chart review of both elective and emergency patients who underwent lower extremity amputation over a six months- period; from November 2015 to April 2016; were reviewed. Data on patients' characteristics, risk factors and indication for amputation were collected. Amputee gender difference, risk factors, indications for amputation and outcome were determined.
Results: Data on 105 records were collected. There were 31 (30%) females and 74 (70%) males; with female to male ratio of 1: 2.3. The mean age was 59 ± 15. Patients of 60 years of age and above were more likely to undergo amputation (58%) followed by the 40 to 59 years' age bracket (35%). Risk of amputation was low in the under 40-year age group (6.7%). Diabetes mellitus as a risk factor for amputation in females was almost double that seen in males (71% vs 36.5%). Chronic vascular insufficiency was the most common risk factor for amputation in males than in females (47% vs 6.5%). There was 9.5% amputation related mortality. Of the 10 deaths, 7 (70%) were due to systemic sepsis.
Conclusion: Diabetes mellitus and chronic vascular insufficiency is associated with high risk of limb loss among our patient population. To minimize risk of limb loss, there is a need to develop special diabetic foot services and mandatory screening for peripheral vascular diseases.
RACIAL DISPARITIES IN BREAST CANCER: A RETROSPECTIVE AUDIT OF 1,820 BREAST CANCER PATIENTS PRESENTING TO A BREAST UNIT IN DURBAN, SOUTH AFRICA
P Reddy1, I Buccimazza1, S Ebrahim1, B Sartorius2
1 Department of Surgery, School of Clinical Medicine (NRMSM-UKZN)
2 Discipline of Public Health, Bio-medical and Statistics (UKZN)
Introduction: Breast cancer is the most common cancer affecting women in South Africa. Women have a 1 in 33 chance of developing breast cancer in South Africa. Racial disparities exist with Blacks having a 1 in 49, Coloureds a 1 in 22, Asians a 1 in 17, and Whites a 1 in 18 chance of developing breast cancer (National Cancer Registry (NCR) Statistics from 2009).
Aim: To describe the racial profile and clinic-pathological presentation of breast cancer patients attending a dedicated breast unit in Durban, South Africa.
Methods: A retrospective audit of files of female breast cancer patients presenting to the Addington and Inkosi Albert Luthuli Central Hospitals' breast unit from January 2008 to 31 April 2013 was performed. Permission was granted by the KwaZulu-Natal Department of Health, and ethical approval was obtained from the Biomedical Ethics Research Committee (BREC) of the University of KwaZulu-Natal (BE002/14).
Results: Complete records were available for 1,820 patients. The average age of women in the study was 56.6 years (SD=13.8). The majority of patients were Indian/Asian 47.9% (872/1,820), followed by Blacks 35.1% (639/1,820). Black patients presented at a younger average age of 52.6 years compared to the other racial groups (p<0.005). Among Black patients, 67.8% (433/639) presented with locally advanced disease (Stage III). Additionally, the proportion of Black patients with metastatic breast cancer (Stage IV) was 20% (128/639).
Conclusion: The advanced stage of disease presentation in the population attending our clinic highlights deficiencies in current breast cancer screening and early detection programmes available to the population we serve. A disproportionately large number of Indian/Asian patients were diagnosed with breast cancer, in our clinic. There is a need to review and implement better-quality programmes, aimed at breast cancer awareness with early detection and diagnosis, and to stream-line the implementation of definitive surgical and oncological therapy.
"I HAVE ONE BREAST, SO WHAT?": PERCEPTIONS OF MASTECTOMY AND BREAST RECONSTRUCTION AMONG PATIENTS AND PEER COUNSELLORS
R van der Wiel1, S Rayne2,3
1 Wits Institute for Social and Economic Research - Medical Humanities & Department of Anthropology, University of the Witwatersrand
2 Department of Surgery, University of the Witwatersrand & Netcare Breast Care Centre
3 Sarah Rayne (Department of Surgery, University of the Witwatersrand, Netcare Breast Care Centre)
Introduction: Breast cancer is the most common cancer among South African women. Prevalent assumptions in breast cancer literature are that women, particularly black women, fear mastectomy and that reconstructive surgery is an important part of treatment to reconstruct a woman's sense of self. Yet there is little in-depth, qualitative research about South African women's experiences of breast surgery.
Aims: This project aimed to give an in-depth account of breast cancer patients' and peer counsellors' perceptions of breast surgery.
Methods: This was a qualitative study of patients, peer-counsellors and doctors at a state specialist breast clinic. The study included semi-structured interviews and participant-observation of clinic life: consultations, peer-counselling, waiting in queues, and in-patient ward. While the broader study included approximately 100 patients, this paper is based on the experiences of 20 women (15 patients and 5 peer-counsellors) whom the researcher followed closely over 7 months.
Results: At time of diagnosis or during treatment none of the 15 patients stated any unwillingness to undergo mastectomy. Patients communicated considerable anxiety about survival and chemotherapy side-effects, but not about mastectomy or breast reconstruction. Without prompting, patients explained their willingness to lose a breast to regain their health. Peer-counsellors always emphasised that living with one breast was acceptable and women with one breast could maintain intimate relationships. Patient and counsellor perceptions of breast surgery had no correlation with race group. Only 3 of the 15 patients spoke positively about reconstruction, with 2 patients voicing resentment towards doctors persuading them to have it. Peer-counsellors described their own experiences when discussing surgeries and exhibited some bias against reconstructive surgery.
Conclusions: Overall women's anxieties about survival far outweighed their anxieties about losing a breast. This contradicts most literature on perceptions of mastectomy and breast reconstruction, and points to underlying gendered assumptions about feminine, heterosexual identity in this literature.
DERIVATION, VALIDATION AND APPLICATION OF A LOW TO MIDDLE INCOME COUNTRIES SPECIFIC INDEX TO PREDICT OUTCOME FOLLOWING NONCARDIAC SURGERY
R T Spence1,2, D C Chang1,3, H M A Kaafarani3, E Panieri2, G Andersen3, M M Hutter1,3
1 Codman Center, Massachusetts General Hospital, Boston, USA
2 University of Cape Town, Department of General Surgery, South Africa
3 Havard Medical School, Boston, MA
Introduction: Despite the existence of multiple validated risk-assessment and quality benchmarking tools in surgery, their utility in low resource settings is often limited.
Aim: We sought to derive, validate and apply a scoring system that is both 1) feasible, and 2) reliably predicts mortality in a Low to Middle Income Country (LMIC) context.
Methods:
A 5-step methodology was used:
• Development of a de novo surgical outcomes database modeled around the American College of Surgeons' National Surgical Quality Improvement Program (ACS-NSQIP) in a LMIC (SA dataset)
• Use of the resultant data to identify all predictors of inhospital death with more than 90% capture indicating feasibility of collection
• Derive and validate an integer-based score that reliably predicts in-hospital death in the 2012 ACS-NSQIP database using the identified predictors in the SA dataset
• pply the score in the original SA dataset and demonstrate it's performance
• Identify threshold cutoffs of the score to prompt action and drive quality improvement.
• UCT Ethics approved study (HREC REF 33/2014).
Results: Following Step one-three above, the 13 point Codman's score was derived and validated on 211,737 and 109,079 patients, respectively, and includes: 1) age>65 (1), partially or completely dependent functional status (1), preoperative transfusions >4 units (1), emergency operation (2), sepsis or septic shock (2) American Society of Anesthesia (ASA) score >3 (3) and operative procedure (1-3) (Table 1). Application of the score to the whole ACS-NSQIP, was associated with a stepwise increase in both in-hospital mortality and any morbidity at 30 days (Figure 1). Application of the score to 373 patients in the SA dataset showed good discrimination and calibration to predict an in-hospital death. Preoperatively, a score of greater than 7 should prompt an ICU admission. Postoperatively, a score of 8 is an optimal cutoff point for defining expected and unexpected deaths.
Conclusion: We have designed a novel risk prediction score specific for a LMIC context. The Codman Score can prove useful for both 1) preoperative decision-making and 2) benchmarking the quality of surgical care in LMIC's.
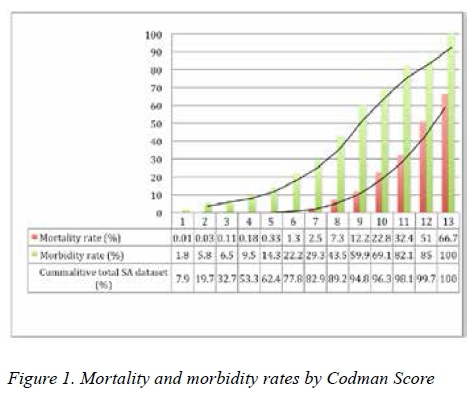

EMERGING M-HEALTH TRANSFORMS INJURY SEVERITY SCORING IN SOUTH AFRICA
R T Spence1,2, E Zargaran3, M Hameed3, P H Navsaria3, A Nicol2
1 Codman Center, Massachusetts General Hospital, Boston, USA
2 University of Cape Town, Department of General Surgery, South Africa
3 Vancouver General Hospital Department of General Surgery, British Columbia, Canada
Introduction: The burden of data collection associated with injury severity scoring has limited its application in areas of the world with the highest incidence of trauma.
Aim: To decrease the data burden associated with injury severity scores in order to increase their predictive performance in a busy trauma unit in South Africa.
Methods: Since January 2014, electronic records (eTHR) replaced all handwritten records at the Groote Schuur Hospital Trauma Unit in South Africa (Figure 1). Data fields required for Glascow Coma Scale (GCS), Revised Trauma Score (RTS), Kampala Trauma Score (KTS), Injury Severity Score (ISS) and Trauma Score-Injury Severity Score (TRISS) calculations are now prospectively collected. Fifteen months following implementation of eTHR, the injury severity scores were compared as predictors of mortality on three accounts:
1. Ability to discriminate (area under receiver operating curve, ROC)
2. Ability to calibrate (observed versus expected ratio, O/E)
3. Associated data burden (rate of missing data) UCT Ethics approved study (HREC REF 33/2014).
Results: A total of 7,460 admissions were recorded by eTHR 1st April 2014- 7th July 2015, including 770 severely injured patients (ISS greater than 15) and 950 operations. The mean age was 33.3 years (range 13-94), 77.6% were male and the mechanism of injury was penetrating in 39.3% of cases. The cohort experienced a mortality rate of 2.5%. Patient reserve predictors required by the scores were 98.7% complete, physiological injury predictors were 95.1% complete and anatomical injury predictors were 86.9% complete. The discrimination and calibration of TRISS was superior for all admissions (ROC 0.9591 and O/E 1.01) and operatively managed patients (ROC 0.8427 and O/E 0.79). In the severely injured cohort, the discriminatory ability of RTS was superior (ROC 0.8315) but no score provided adequate calibration (Table 1).
Conclusions: Emerging m-Health technology enables reliable and sustainable injury severity scoring in a high volume trauma unit in South Africa.
INJURY SEVERITY SCORE CODING: MAN VERSUS EMERGING MOBILE HEALTH TECHNOLOGY
R T Spence1,2, E Zargaran3, M Hameed3, D Fong3, E Shangguan3, R Martinez3,P H Navsaria3, A Nicol2
1 Codman Center, Massachusetts General Hospital, Boston, USA
2 University of Cape Town, Department of General Surgery, South Africa
3 Vancouver General Hospital Department of General Surgery, British Columbia, Canada
Introduction: The cost of Abbreviated Injury Severity coding has limited its utility in areas of the world with the highest incidence of trauma.
Aim: To demonstrate that emerging mobile-health (m-Health) technology could offer a costeffective alternative to the current gold-standard Abbreviated Injury Scoring (AIS) mechanism in a high volume trauma center in South Africa.
Methods: A prospectively collected sample of consecutive patients admitted following a traumatic injury that required an operation during a 1-month period was selected for the study. AIS and Injury Severity Scores (ISS) were generated by clinician-entered data using a mobile-health application (ISS eTHR) as well as by a team of AIS coders at the Vancouver General Hospital, Canada (ISS VGH). Rater agreements for ISS were analysed using Bland-Altman plots with 95% limits of agreement (LoA) and kappa statistics of the ISS grouped into ordinal categories. Reliability was analysed using a two-way mixed model intraclass correlation coefficient (ICC). Calibration and discrimination of univariate logistic regression models built to predict in-hospital complications using ISS coded by the two methods were also compared. UCT Ethics approved study (HREC REF 33/2014).
Results: Fifty seven patients were managed operatively during the study period. The mean age of the cohort was 27.2 years (range 14-62) and 96.3% were male. The mechanism of injury was penetrating in 93.4% of cases of which 52.8% were gunshot injuries (Table 1). The LoA fell within -8.6 to 9.4. The mean ISS difference was 0.4 (95% CI -0.8 - 1.6). The kappa statistic was 0.53. ICC of the individual ISS was 0.88 (95% CI 0.81 - 0.93) and the categorical ISS was 0.81 (95%CI 0.68 -0.87). Model performance to predict in-hospital complications using either ISS eTHR or ISS VGH was equivalent.
Conclusions: ISS calculated by eTHR and gold standard coding were comparable. Emerging m-Health technology provides a cost effective alternative for injury severity scoring.
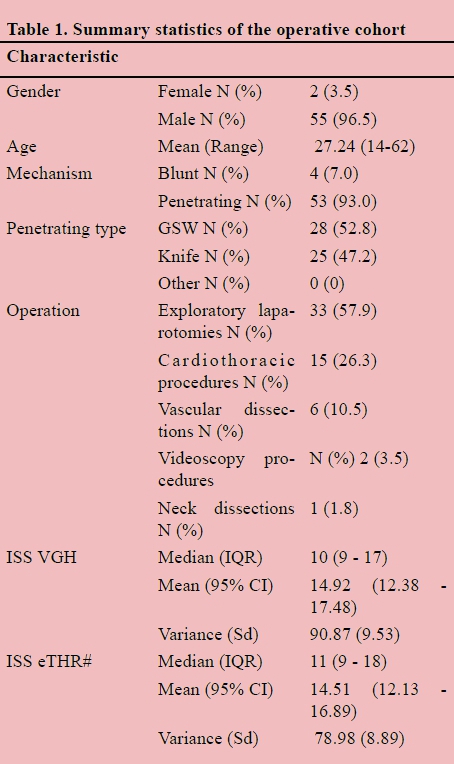
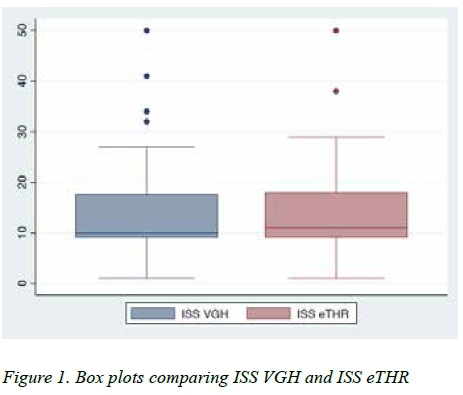
AN OBJECTIVE ASSESSMENT OF THE SURGICAL TRAINEE IN AN URBAN TRAUMA UNIT IN SOUTH AFRICA
R T Spence1,2, E Zargaran3, M Hameed3, P H Navsaria3, A Nicol2
1 Codman Center, Massachusetts General Hospital, Boston, USA
2 University of Cape Town, Department of General Surgery, South Africa
3 Vancouver General Hospital Department of General Surgery, British Columbia, Canada
Introduction: Surgical outcomes are provider specific. This prospective audit describes the surgical activity of five general surgery residents on their trauma surgery rotation.
Aim: To test the hypothesis that the operating surgical trainee is an independent risk factor for adverse outcomes following major trauma.
Methods: This is a prospective cohort study. All patients admitted, over a 6-month period (August 2014- January 2015), following trauma requiring a major operation performed by a surgical trainee at Groote Schuur Hospital's level 1 trauma unit in South Africa were included. Multiple logistic regression models were built to compare risk-adjusted surgical outcomes between trainees. The primary outcome measure was major in-hospital complications.
Results: A total of 320 major operations involving 341 procedures were included (Table 1). The mean age was 28.49 years (range 13-64), 97.2% were male with a mean ISS of 13 (range 4-50). Mechanism of injury was penetrating in 93.42% of cases of which 51.86% were gunshot injuries. Surgeon A consistently had the lowest risk-adjusted outcomes and was used as the reference for all outcomes in the regression models. Surgeon B, D & E had statistically significant higher rates of major in-hospital complications than Surgeon A and C, after adjusting for multiple confounders. The final model used to calculate the risk estimates for the primary outcome had a ROC of 0.8649. UCT Ethics approved study (HREC REF 33/2014).
Conclusions: Risk-adjusted surgical outcomes vary by operating surgical trainee. The analysis thereof can add value to the objective assessment of a surgical trainee.
AN ONLINE TOOL FOR GLOBAL BENCHMARKING OF RISK-ADJUSTED SURGICAL OUTCOMES
R T Spence1,2, D C Chang1,2, C Chu3, E Panieri2, J L Mueller3, M M Hutter1,3
1 Codman Center, Massachusetts General Hospital, Boston, USA
2 University of Cape Town, Department of General Surgery, South Africa
3 Havard Medical School, Boston, MA
Introduction: Increasing evidence demonstrates significant variation in adverse outcomes following surgery between countries.
Aim: In order to better quantify these variations, the aim of this study was to demonstrate that freely available online risk calculators could be used as a tool to generate global benchmarking of risk-adjusted surgical outcomes.
Methods: This is a prospective cohort study conducted at an academic teaching hospital in South Africa (GSH). Consecutive adult patients undergoing major general or vascular surgery that met the American College of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP) inclusion criteria for a 3-month period were included. Data variables required by the ACS-NSQIP risk calculator were prospectively collected (Table 1) and patients were followed for 30 days post surgery for the occurrence of endpoints. Calculating observed-toexpected ratios for 10 outcome measures of interest generated risk-adjusted outcomes benchmarked against the ACS-NSQIP consortium. UCT Ethics approved study (HREC REF 33/2014).
Results: 373 Major general and vascular surgery procedures met the inclusion criteria. The GSH operative cohort varied significantly compared to the 2012 ACS-NSQIP database. The riskadjusted O/E ratios were significant for any complication O/E 1.91 (95% CI 1.57 - 2.31), cardiac complications (O/E= 2.58; 95% CI 1.15 - 5.24), surgical site infections O/E 4.76 (95% CI 3.71 - 6.01), renal failure O/E 3.29 (95 % CI 1.50 -6.24), death O/E 3.43 (95% CI 2.19 - 5.11) and total length of stay (LOS) O/E 2.96 (95% CI 2.89 - 2.99). These ratios were plotted on a caterpillar plot (Figure 1).
Conclusion: Freely available online risk calculators can be utilized as tools for global benchmarking of risk-adjusted surgical outcomes.
Preoperative variables collected
Patient demographics
Age Sex Height Weight
Procedure related
Name of procedure (converted to CPT code by the risk calculator)
Emergency case (Yes/ No) ASA Class (1-5)
Wound class (Clean/ Clean-contaminated/ Contaminated/
Dirty-infected)
Preoperative risk assessment
Steroid use for chronic condition (Yes/ No)
Ascites within 30 days prior to surgery (Yes/ No)
Systemic sepsis within 48 hours prior to surgery (None/ SIRS/
Sepsis/ Septic shock)
Ventilator dependent (Yes/ No)
Disseminated cancer (Yes/ No)
Diabetes (None/ Oral medication/ Insulin medication)
Hypertension requiring medication (Yes/ No)
Previous cardiac event (Yes/ No)
Congestive heart failure in 30 days prior to surgery (Yes/ No) Dyspnea (None/ With moderate exertion/ At rest) Current smoker within 1 year (Yes/ No)
History of severe COPD (Yes/ No)
Dialysis (Yes/ No)
Acute renal failure (Yes/ No)

TB OF THE BREAST: A DIAGNOSTIC CHALLENGE. A SERIES OF 19 CASES FROM CHRIS HANI BARAGWANATH HOSPITAL AND REVIEW OF THE LITERATURE
R Hoffman1, H Cubasch2
1 Department of Surgery, Chris Hani Baragwanath Hospital
2 Head of the Batho Pele Breast Unit, Chris Hani Baragwanath Hospital
Introduction: Tuberculosis (TB) of the breast is considered a rare condition, and like other extra pulmonary manifestations of TB, it is often challenging to confirm.
Aims: To describe the spectrum of clinical presentation, examine the relationship between HIV and TB of the breast, analyse the commonly used diagnostic methods and establish a rational diagnostic approach.
Methods: In this retrospective, consecutive case series, we present 19 cases of TB of the breast encountered in 2015 at the Chris Hani Baragwanath Academic Hospital Batho Pele Breast Clinic. We included all patients who had confirmed TB of the breast.
Results: Thirteen of our cases presented with a breast lump, half of which were thought to be malignant on clinical examination. Five presented with a breast abscess, and one with mastitis. At the time of presentation 73% of the patients were HIV positive, of which 71% were on antiretroviral treatment. The median time before presenting to the health system was two months. A variety of diagnostic tests were utilised including TB microscopy, TB cultures, genotypic tests such as nested PCR and MTB/RIF assays (XperT®), FNA cytology, and histology. After initiation of TB treatment and onward referral, the majority of the patients (74%) have been lost to follow up.
Conclusions and Recommendations: This study emphasises the diagnostic challenge that is posed by TB of the breast, as demonstrated by the large number of falsely negative tests. Despite its availability and cost effectiveness, the MTB/ RIF assay is still an under-utilised diagnostic tool. Our series suggests that the finding of necrotising granulomatous inflammation of the breast is pathognomonic for TB; we recommend initiation of treatment based on this histological finding alone.
TRIPLE NEGATIVE BREAST CANCER PRESENTS AT A YOUNGER AGE, WITH LARGER TUMOURS, AND WITH A MORE ADVANCED STAGE WHEN COMPARED WITH HORMONE POSITIVE BREAST CANCER IN A SINGLE CENTRE BREAST CLINIC IN SOUTH AFRICA
S D Hariparsad,I Buccimazza, P Reddy
Breast, Endocrine and Soft Tissue Unit, Specialised Surgical Services, Inkosi Albert Luthuli Central Hospital
Background and aims: Triple negative breast cancer presents at a younger age, with more aggressive clinical and biologic tumour features, and a high propensity for distant metastases. African-American women have a higher risk of developing this subtype than their White counterparts. The prevalence of this disease varies in the developed world as well as on the African continent. The aim of this study is to characterize triple negative breast cancer in a single centre breast clinic in Durban, South Africa
Methods: An existing database of consecutive breast cases was searched and two cohorts of breast cancer patients were extracted. A triple negative cohort and a hormone positive, but human epidermal growth factor two negative cohort were compared in the form of a retrospective cohort study. A retrospective chart analysis of the triple negative cohort was then performed to complete the analysis.
Results: The prevalence of triple negative breast cancer was 6.5% with 119 patients and 120 breast tumours identified. The median age at presentation of 53 years was lower than the hormone positive group (p<0.001), and the stage at presentation was more advanced for triple negative cancer patients (p=0.002). Black patients were not more likely to have triple negative breast cancer compared to hormone positive breast cancer (p=0.8), but presented at a younger age than White patients (p=0.01), and with larger clinical tumour size at presentation (p=0.001). Distant metastatic sites were most common in the lung and bone, and recurrence occurred most frequently within the first 2 years. Genetic testing results for 6 patients were available with only 2 patients testing positive for BRCA mutations.
Conclusions: The prevalence of triple negative breast cancer is lower in our setting, but many tumour characteristics such as younger age and aggressive biology seen in other studies was also present in our patient cohort.
A PROSPECTIVE EVALUATION OF THE MODIFIED ALVARADO SCORE FOR THE DIAGNOSIS OF ACUTE APPENDICITIS IN HIV-INFECTED PATIENTS
S Sobnach1,2, C Ede1,3, G van Der Linde4, J Klopper2, D Kahn2, A Bhyat1
1 Department of General Surgery, Kimberley Hospital Complex
2 Department of General Surgery, Groote Schuur Hospital and University of Cape Town
3 Department of Surgery, University of Witwatersrand
4 Department of Anatomical Pathology, Kimberley Hospital Complex
Introduction: The Modified Alvarado Score (MAS) is an inexpensive and easily reproducible diagnostic tool for acute appendicitis. A MAS > seven suggests the diagnosis with an accompanying sensitivity and specificity of 98% and 100% respectively.The use of the MAS in the HIV-positive (HIVpos) is controversial since the clinical presentation of appendicitis can be atypical in these patients.
Aim: The aim of this study was to analyse and compare the diagnostic value of the MAS for acute appendicitis in a HIVpos and HIV-negative (HIVneg) patient cohorts.
Methods: After ethical approval, a prospective study including all HIV-tested patients undergoing appendectomy at Kimberley Hospital from March 2010 to March 2011 was performed. The MAS was calculated for all patients, and for the HIVneg and HIVpos groups separately. Two subgroups were considered for each of these: MAS > seven (high likelihood of appendicitis) and MAS < seven (low likelihood of appendicitis). These subgroups were then analysed against histopathological findings of the resected appendix. MAS specificities and sensitivities were determined by comparing Receiver Operator Characteristic (ROC) curves for the various scores.
Results: The study comprised 133 patients. Eighty-six (65%) were men and the median age was 20 years (range: 4-64); 18 patients (14%) were HIVpos. Appendicitis was confirmed histologically in 113 patients, 100 in the HIVneg group and 13 in the HIVpos group. Specificity and sensitivity of a MAS > seven for HIVneg patients was 73% and 85% respectively. Based on the ROC curves, HIVpos patients only showed similar sensitivities (69%) and specificities (80%) at a MAS > eight.
Conclusion: A MAS > seven is a reliable predictor of acute appendicitis in HIVneg patients. In HIVpos patients, the MAS threshold required to accurately predict appendicitis is eight. The use of a MAS > seven in this group of patients will result in unnecessary surgical intervention.
MEDICAL STUDENTS' KNOWLEDGE ABOUT BRAIN DEATH: A SOUTH AFRICAN CONTRIBUTION
S Sobnach, K Wiese, M Tselanyane, M Borkum, D Kahn, R Segobin
Solid Organ Transplant Unit & Department of General Surgery, Groote Schuur Hospital and University of Cape Town
Introduction: Incorporating transplantation into undergraduate medical curricula can improve organ procurement rates. Intricacies related to the assessment of donor suitability, the clinical diagnosis of brain death and relevant legal processes are key challenges for the newly qualified doctor.
Aim: The aim of this study was to describe and analyse the knowledge of medical students regarding the various aspects dealing with the diagnosis of brain death, with a view to designing an undergraduate training module.
Methods: The Human Research Ethics Committee of the Faculty of Health Sciences at the University of Cape Town (UCT) granted ethical approval for this study. A previously validated self-administered 26-item questionnaire was distributed to all medical students at UCT. General data included age, gender, year of study, career interests and organ donor status. Knowledge-specific questions explored the suitability of potential organ donors (eight items), the clinical diagnosis of brain death (seven items) and legal factors thereof (11 items). Statistical analysis was performed using SPSS version 15.0. Chi-square and Fisher exact tests were used to compare the data. A two-sided P < 0.05 was considered statistically significant.
Results: There were 346 participants; 217 (63%) were pre-clinical students and 29 (8%) carried an organ donor card. The mean and median score for the 26-items was 12 (Range: 0-25). Mean scores did not increase significantly with years of medical education: from eight in the first year of study, 10 in the second year and 17 in the final year (P > 0.05). Demographics, year of study, organ donor status and an interest in a surgical career did not influence knowledge levels (P > 0.05).
Conclusion: Medical students have limited knowledge about brain death and identification of potential organ donors. This confirms the need for an educational intervention early in the medical curriculum.
THE PREVALENCE AND CLINICAL PROFILE OF ADULT BURNS DUE TO ASSAULT: A SOUTH AFRICAN ADULT BURN CENTRE REVIEW
S Koonin1, R Moore2, J Fabian3
1 Department of Surgery, Registrar, University Witwatersrand, Discipline of Plastic Surgery.
2 Department of Surgery (Trauma Directorate), Chris Hani Baragwanath Academic Hospital, Discipline Specialist Surgeon (Burns), Fellow in Critical Care.
3 Head Research Unit, Wits Donald Gordon Medical Centre, Discipline of Nephrology.
Introduction: In developing countries it has been shown that burn injuries are one of the most important public health problems and cause of morbidity, disability, mortality, psychosocial problems and decreased quality of life. Previous studies show the prevalence of assault by burns to be variable. Burns are preventable, but require epidemiological and aetiological data, which vary in each country, for planning and implementation of preventative strategies. Currently there is a paucity of data from South Africa.
Aim(s): To determine the prevalence, the epidemiological factors and clinical profile of adults burns patients due to assault.
Methods: A retrospective descriptive study, using hospital records at the Chris Hani Baragwanath Academic Hospital (CHBAH) in the Adult Burns Unit (ABU) on all consecutive acute admissions (elective readmissions were excluded), 18 years and older, from September 2005 to December 2014. The 1928 patients cohort divided into the assault and control group. The inclusion criteria were the requirements for CHBH ABU admission. Descriptive statistics were utilised, including the student t-test and Chi-squared test with p<0.05 being statistically significant. Ethics approval was obtained from University of Witwatersrand's Human Research and Ethics Committee.
Results: The prevalence of burns via assault was 21.42% with the majority from scalding. The data did not show any statistically significant relationship between assault and age, gender, length of hospital stay or inhalation injuries. However, there was a statistical significance correlation with mortality (p<0.010), Intensive care admission (p<0.009) and total body surface area involved assessing severity (p<0.041).
Conclusion/Recommendations: Burns via assault are more severe and have a higher mortality. The prevalence in this study is significantly higher then in developed countries where preventative programs have been effective. These findings are critical to designing and implementing effective prevention strategies to decrease the burden of disease.
PENETRATING FEMORAL ARTERY INJURY- AN URBAN TRAUMA EXPERIENCE
S Rayamajhi, J Klopper, A J Nicol, S Edu, P H Navsaria
Trauma Centre, Groote Schuur hospital, Faculty of Health Sciences, UCT
Introduction and aim: Femoral artery injury is the second most common peripheral vascular injury seen. The aim of this study is to review the outcome of patients with such injuries in a centre with a high incidence of penetrating trauma.
Methodology: This is a retrospective review of all femoral artery injuries from 1 January 2002 to 31 December 2013, a 12 year period. The data collected and analysed were demographics, injury mechanism, peri-operative management, intra-operative findings, type of repair, fasciotomy. Presenting limb status was categorized into viable, threatened and non-viable limbs. Outcome was grossly categorized by limb salvage.
Results: 158 patients presented with femoral artery injury. There were 154 men, mean age was 28 (15-71) years. There were 151 (96%) penetrating injuries. 112 (70%) were low
velocity GSWs and 38 (24%) stab wounds and 8 (4%) blunt injuries. 70 (44%) patients presented with a threatened limb, 85 (54%) with a viable limb and 3(2%) with non-viable limb. There were 4 primary amputations and 10 (6.5%) secondary amputations. 101 patients had investigation prior to surgery and 57 had emergency exploration. 81 primary anastomosis was done, 15 prosthetic graft interposition and 45 vein interposition graft. Of the 10 secondary amputations 8 were done for ischemic necrosis despite revascularization. 1 was done for compartment syndrome post temporary vascular shunt in situ. 1 was a viable limb with anastomotic complication with ongoing bleeding and limb loss. Of the 4 primary amputations 3 presented with a non-viable limb and 1 threatened limb on presentation with delay to surgery.
Conclusion: An initial aggressive approach to femoral artery injury by trauma surgeons is associated with a good limb salvage rate.
IS LAPAROSCOPIC GRAHAM PATCH SAFE IN PATIENTS WITH PERFORATED PEPTIC ULCER DISEASE WHO ARE DELAYED PRESENTERS WITH A HIGH BOEY SCORE?
S Makhadi, M Z Koto
Minimal Invasive Unit, Department of General Surgery, Sefako Makgatho Health Sciences University
Background: Laparoscopic management of perforated peptic ulcer has become an acceptable treatment strategy in selected patients. The traditional indication for this procedure is a patient who presents early with a Boey score of zero or 1.
Most investigators would recommend laparotomy for those patients with a Boey score of 2 or 3. There is paucity of data on outcomes of these patients with a high Boey score.
Aim: The aim of our study was to evaluate the outcome of patients with perforated peptic ulcer with a high Boey score.
Methods: This was a retrospective review of prospectively collected data of patients with perforated peptic ulcer seen between November 2011 and May 2016. We looked at the data of all patients with perforated peptic ulcer that were offered laparoscopic surgery. Of all these patients we looked at the ones with a Boey score of 2 and 3 for analysis.
Results: 125 patients with perforated peptic ulcer were offered laparoscopic Graham patch. Of these patients 50 had a Boey score of 2. 3 had Boey score of 3. Overall conversion rate was 4%, main reason for conversion was poor visibility.2 patients required relook surgery. Mortality rate in this group was zero. Average hospital stay was 5 days.
Conclusion: Laparoscopic Graham patch is feasible and safe even in patients with delayed presentation. The operating time is longer in these patients. Further studies are needed to evaluate the role of laparoscopy in this cohort of patients.
PREVALENCE OF CHEMOTHERAPY-INDUCED NEUTROPENIA IN BREAST CANCER PATIENTS RECEIVING NEO-ADJUVANT CHEMOTHERAPY: COMPARATIVE ANALYSIS BETWEEN HIV INFECTED AND UNINFECTED PATIENTS
S Ngidi1, P A Govender1, T E Madiba2
1 Department of Oncology, University of KwaZulu-Natal, Durban
2 Surgery, University of KwaZulu-Natal, Durban BREC Ethical Approval: BE 094/14
Introduction: Cytotoxic chemotherapy suppresses the body's haemopoietic system. Neutropenia, especially febrile neutropenia is the most serious hematologic toxicity and is associated with the risk of life threatening infections and chemotherapy dose reductions.
Purpose: To describe the prevalence and level of neutropenia in HIV infected patients, compared to HIV uninfected patients receiving neo-adjuvant chemotherapy for breast cancer, and to compare and identify patient dependant factors that may influence the development of neutropenia.
Methods:
• Study setting: Oncology Departments at Inkosi Albert Luthuli Central and Addington Hospitals, Durban.
• Study population: Randomly selected HIV infected and HIV uninfected women with breast cancer stage II-IV who received neo-adjuvant chemotherapy from January 2012 to December 2015.
• Study design: Retrospective chart review and analysis. Demographics, prevalence and level of neutropenia, patient factors and treatment outcome were analysed.
Results: A total of 71 women of mean age 48.1 (12.8) years were enrolled. Twenty-five were HIV positive. 46 were HIV negative with mean CD4 count of 420 cells/mm3.
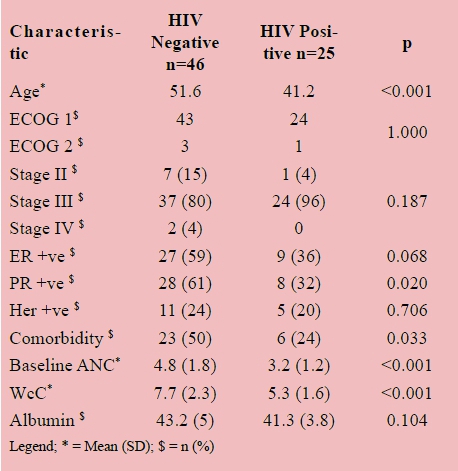
Conclusion: HIV positive patients were younger. Baseline leucopaenia and neutropaenia were strongly associated with HIV positivity. Disease stage had no influence.
THE ACCURACY OF COMPUTERIZED TOMOGRAPHY INVESTIGATION OF HOLLOW VISCOUS INJURY IN PENETRATING ABDOMINAL TRAUMA
S K Makhoba, A V V Lambrechts, B L Warren
Division of surgery, Tygerberg Academic hospital and Stellenbosch University
Introduction: The Tygerberg Academic Hospital Trauma Unit manages in excess of 15 000 patients per year. A high burden of penetrating abdominal trauma due to stab wounds and low velocity gunshot wounds present to the Unit.
Aim(s): Computed Tomography (CT) is commonly utilized to evaluate penetrating abdominal trauma for specific indications. The aim is to evaluate the accuracy of CT in determining the presence of hollow viscous injury in penetrating trauma in the presence of free intra-peritoneal air.
Methods: A prospective cohort study performed at Tygerberg Academic Hospital between January 2011 and December 2014.
Inclusion criteria: Age >13 years, penetrating abdominal trauma, CT scan performed with a finding of free intraperitoneal air, laparotomy based on CT findings.
Exclusion criteria: Laparotomy for penetrating trauma without prior CT scan and patients with CT who underwent laparotomy for other indications. Informed consent was obtained from the patient or next of kin. Ethics approval by the Stellenbosch University HREC.
Results: A total of 150 patients were included in the study. 23 patients were stabbed (15%) and 127(85%) sustained low velocity gunshot wounds. In 17(11%) patients there was no hollow viscous injury at surgery and 133(89%) had an injury. The overall sensitivity of CT scan is 89% in this study. When only gunshot injuries were taken in isolation, the sensitivity was 91%.
Conclusion/Recommendations: CT is accurate in determining hollow viscous injury after penetrating trauma to the abdomen, with a sensitivity of 89%. This study reaffirms the knowledge that CT is the diagnostic modality of choice in penetrating abdominal trauma for suspected hollow viscous injury.
BREASTFEEDING UPTAKE AND BARRIERS IN WOMEN IN JOHANNESBURG, SOUTH AFRICA
S Brandt, M Losper, K Manaka, V Olusola, M Pohl, I Swart, C Benn, S Rayne
Department of Surgery, University of the Witwatersrand
Introduction: Advantages of exclusive breastfeeding to both infants as well as mothers have been proven in numerous studies. While exclusive breastfeeding is promoted by the South African government in all populations, low uptake rates are reported for a variety of reasons.
Aim(s): The study critically assessed and documented breastfeeding practices and identified barriers to the uptake of breastfeeding in women in the greater Johannesburg metropolitan area.
Methods: Women attending a diverse set of hospital and public mall locations in Johannesburg were approached. Using a quantitative data collection method with this convenience sample we asked questions about different notions and beliefs that promote and/or discourage breastfeeding established in the literature. Statistical data analysis and interpretations was done using SPSS software package. Ethics approval was obtained by the institutional HREC (Medical)
Results: The age range of the 175 participants was between 18 and 72 with a median age of 32. They were predominantly black African (79%, with coloured, 14%; white 5%; and indian 2%) and negative HIV status (83%). Most participants had completed secondary education (94%) and 52% earned over R5000. Exclusive breastfeeding was carried out by 58% of participants.
When compared to exclusive formula feeding, women who breastfed believed that breastfeeding helped bonding, and was easier and less expensive. They also agreed it did not affect their relationship with a partner, and disagreed that breast and formula were equally healthy options. Both combined and exclusive breastfeeding groups agreed that "A healthcare worker encouraged me to breastfeed".
Conclusion/Recommendations: Uptake of exclusive breastfeeding was much higher in our study population than the national average. This study showed that the practical and sociological experiences of breastfeeding contributed most significantly to the uptake of breastfeeding in our Johannesburg urban population.
VIDEO-ASSISTED THORACOSCOPIC SURGERY VERSUS TUBE THORACOSTOMY RE-INSERTION FOR THE PERSISTENT / RETAINED TRAUMATIC HAEMOTHORAX: INTERIM RESULTS OF A RANDOMISED PROSPECTIVE STUDY
S Edu, P H Navsaria, A J Nicol
Trauma Centre and Department of General Surgery, Groote Schuur Hospital and University of Cape Town, South Africa
Introduction: The retained haemothorax after first tube thoracostomy insertion is common, with reported incidences of up to 20% in trauma patients. The management of retained haemothoraces varies significantly between institutions and amongst trauma surgeons.
Aim: The aim of this study is to compare the outcomes between the two modalities of treatment for retained haemothoraces, namely Video-Assisted Thoracoscopic Surgery (VATS) and re-insertion of Tube Thoracostomy (TT).
Methods: The Human Research Ethics Committee at the University of Cape Town granted ethical approval for this study (HREC 119/2013). A prospective randomised study of VATS versus TT for retained traumatic haemothoraces was established at the Trauma Centre at Groote Schuur Hospital. A predetermined sample size was generated using PASS 12 software. All stable patients (aged 18-60 years) with a retained haemothorax were included in the study following informed consent. Exclusion criteria included haemodynamic instability, polytrauma and underlying chronic lung disease. Demographics, type of procedure, total hospital stay and complications were documented for each patient. Statistical analyses were performed using the Student t test for normal distributions and Mann-Whitney-Wilcoxon rank sum test where appropriate. A P-Value < 0.05 was considered statistically significant.
Results: The initial sample comprised 30 patients, 14 in the VATS arm and 16 in the TT arm. Three patients were excluded; two in the VATS arm retracted consent and one patient in the TT arm had a delayed pericardial infusion. Thus, data from 27 (12 VATS, 15 TT) patients were subjected to analysis. The length of stay was similar in both groups. The complication rate was significantly higher in the TT group than the VATS group (47% vs. 0%, P = 0.008). Clinical follow up in both patient groups was 50%.
Conclusions: Preliminary results suggest that the use of VATS for retained traumatic haemothoraces is associated with lower morbidity than tube thoracostomy.
NEUTROPHIL LYMPHOCYTE RATIO AS A PROGNOSTIC MARKER IN BURNS PATIENTS
T Muthambi, G P Candy, R Moore, A Mugunza A.
Burns Unit and General Surgery, University of the Witwatersrand, Johannesburg
Introduction: Thermal burns are associated with significant morbidity and mortality. The systemic inflammatory response in a burn patient manifests as changes in the peripheral white cell distribution, depressed lymphocyte counts and a raised neutrophil count. The neutrophil lymphocyte ratio (NLR) has prognostic value in prostate, colorectal and breast cancer, sepsis and cardiovascular disease. The NLR .can be used to measure the systemic inflammatory response and may be a potential marker of prognosis in burns.
Aim: to determine the prognostic value of NLR in burn patients.
Methods: A prospective observational study (Ethics approval M141106) was undertaken at the Chris Hani Baragwanath Burn Centre between February - September 2015. Eighty patients older than 11 years of age were include irrespective of the burn mechanism or depth, ward or ICU. Paediatric patients and those with septic or old wounds were excluded. Patient demographics and burn data (TBSA, IHT) LOS, overall outcome (survival vs mortality) and FBC with a differential count at days 1, 3 and 7 were recorded.
Results: NLR was not elevated and did not change over time. Logistic regression did not show NLR to be an independent predictor of mortality. In contrast the neutrophil count was significantly increased in non-survivors and was shown in logistic regression to have value in predicting survival.
Conclusions: NLR is of little value in predicting outcomes in burn patients. However, neutrophil counts may be of interest in these patients.
USE OF ANORECTAL ENDOSONOGRAPHY FOR ACCURATE ANATOMICAL RECONSTRUCTION OF DESTROYED RECTOVAGINAL SEPTUM WITH ANAL INCONTINENCE OR RECTOVAGINAL FISTULA
T mokoena
Department of Surgery, University of Pretoria
Introduction: Third and 4th degree perineal tears during childbirth remain a problem in South Africa. These perineal tears are usually recognised and repaired primarily by attending midwives and obstetricians or gynaecologists. However some of these repairs breakdown even after repeated attempts. It is the latter group that present to general surgeons for repair.
Aim: To review repair of incontinent anal sphincters and rectovaginal fistulae (RVF) assisted by prior endoluminal ultrasound imaging from 1995 to 2015 at the University of Pretoria Academic Training Hospitals.
Patients and Methods:. Hospital records of patients managed by the author were reviewed. All patients were evaluated with anorectal endosonography to define the exact extent of muscle damage which is replaced by fibrous tissue. All patients also had a barium enema to exclude other or occult fistulae, or sinuses in the rectum. Our surgical technique is based on excision of all fibrous tissue guided by endosonar findings until one encounters healthy muscle tissue followed by meticulous dissection and repair strictly in corresponding layers. During the earlier period protective colostomy was also fashioned but later colostomy was dispensed with.
Result: Sixteen patients were managed between 1995 and 2015. All patients were female with average age of 30 years (range 21 - 63). Thirteen had previous childbirth trauma; 6 presented with faecal incontinence and 10 with rectovaginal fistula. One or more attempts of repair had been done in all prior to referral. One elderly patient had idiopathic RVF, another elderly patient had RVF following repair of rectocoele and in the sixteen patient with anal incontinence the underlying cause was not recorded. Five patients had temporary protective colostomy and needed anal dilation before colostomy closure. One patient developed a post-op haematoma which became infected and resulted in a partial breakdown of the repair which healed on conservative management. Although long term follow up was poor, few patients were seen upto 12 years after the repair and 2 had subsequent normal vaginal deliveries since the repair. We have not encountered any recurrence in this cohort.
Conclusion: Anorectal endosonography is useful in mapping out the extent of muscle damage and fibrous healing. The success of the repair relies on total excision of fibrous tissue and accurate anatomical layered reconstruction of the rectum, vagina, perineal body and anal sphincter mechanism. There is no need for defunctioning colostomy cover if meticulous post-op use of antiseptics, stool softners and lubricants is diligently followed.
COMPARISON OF LAPAROSCOPIC ACCESS TECHNIQUE THE OPEN HASSON VS VERESS NEEDLE IN GENERAL SURGERY PATIENTS: A RANDOMISED CONTROLLED TRIAL
T Sumbana, M Z koto
Sefako Makgato Health Science University, Dr George Mukhari Academic Hospital, Pretoria, South Africa
Aims: To determine the difference in complication rates between the open hasson and veress needle technique among general surgery patients including the so called high risk group ,(those with high or low BMI, previous abdominal surgery, previous TB, and distended loops of bowel ), at a teaching hospital in a semi-urban area. .
Methods: A randomized controlled trial conducted at Dr George Mukhari Academic Hospital, department of general surgery, Pretoria. The trial was conducted between, 1 November 2014 to 30 November 2015. All general surgery patients older than 18years, scheduled for emergency or elective laparoscopic surgery were recruited for the study. They were randomized to 'A' for veress needle or 'B' for open hasson technique using plug cards. The complications related to either procedure where recorded for statistical analysis. All statistical analysis were performed using the IBM SPSS statistic version 23, the chi square test was used for comparison of the two techniques, frequency tables used for demographics, the p value of <0,05 was considered statistical significance.
Results: A total of 104 patients were recruited for the study, 96 were included in the final analysis and 8 were excluded, because of incomplete data collection sheets, 33 /96 were in the high risk group. A total of 50 patient in the veress needle arm 'A' and 46 patient in the open hasson 'B' arm, age ranging from 18 to 67 years with a mean age of 42, BMI the lowest was 17 and the highest being 45 with the mean of 25 kg/ m2, 47% of which were female and 53% male. The number of emergency procedures was 54%, and 46% were elective procedures. Minor complications were reported in six patients all in the veress needle arm, but it was not statistical significant (p value .309).
Conclusion: Even though the two methods are comparable the veress needle is associated with minor complications, even in the so called high risk group patients, our study did not show statistical significance due to a small sample size.
PREVALENCE OF FACTORS INFLUENCING RECURRENCE AND/OR METSTASIS IN DERMA-TOFIBROSARCOMA PROTUBERANS
A Y Benneh1, P S Kay1, JBL Kiluba1, M J Hale2, T E Luvhengo1
1 Department of Surgery, University of the Witwatersrand
2 Department of Anatomical Pathology, National Health Laboratory Services, University of the Witwatersrand
Introduction: Dermatofibrosarcoma protuberans has limited metastatic potential. The fibrosarcomatous variant of DFSP has increased propensity for local and distant recurrence. The aim of the study was to determine the prevalence of markers of aggressive DFSP.
Methods: We undertook a retrospective review of records of patients with DFSPs. Data retrieved included patients' demography, tumour site, size, biopsy type, excision margin, CD34 expression, mitotic count, presence of necrosis and evidence fibrosarcomatous change. Permission to conduct the study was received from HREC of Wits (M130974)
Results: 75 histopathological records were found of which 25.3% were recurrent. All were from black patients and majority 43/75 (57.3%) were females. Their average age was 39.7 years. Majority (66.7%) were in the trunk and the average size was 8.1cm (range: 1.5cm-19.5cm). Excision was performed in 43/75 (57.3%) and was deemed wide local excision in 35/43. Resection margin was adequate in 5.7%. FS-DFSP was reported in 12/75 (16.0%) overall and 12/43 (27.9%) of excised DFSPs. Most 9/12 (75.0%) of FS-DFSPs were in females. Only 9.7% of classical DFSPs involved limbs whereas 3/12 (25.0 %) of FS-DFSPs were in extremities. Average age of patients and size of FS-DFSPs were 44.7 years and 10.4cm, respectively. And, mitotic count of 5 and above per 10 high-power fields was reported in 74.9% (9/12) of FS-DFSPs.
Conclusion: DFSP is a disease of young adults and majority are above 5cm at presentation. FS-DFSP variant of DFSP affects older patients, is larger and likely to have mitotic count above 10 per 10 per high power field. Adequate tumour resection margin is rarely achieved.
PREDICTORS OF OCCURRENCE OF OMENTAL DEPOSITS IN PATIENTS WITH GASTRIC ADENOCARCINOMA UNDERGOING GASTRECTOMY: A HISTOPATHOLOGICAL AUDIT
O Tobiko, J Kiluba, C Jann-Kruger, M J Hale, T E Luvhengo
Department of Surgery, School of Clinical Medicine, University of the Witwatersrand and NHLS Department of Anatomical Pathology, School of Pathologies; University of the Witwatersrand and NHLS
Introduction: Milky spots in greater omentum are primary sites for seeding of exfoliated cells from transmural gastric cancer. Surgery is the mainstay of treatment of gastric adenocarcinoma and the greater omentum is usually resected en-bloc.
Aim: To determine if pathologists routinely perform analysis of greater omentum, and factors associated with findings of cancer deposits.
Methods: An audit of histopathology records of patients who had gastric malignancies between 2008 and 2012 was undertaken. Data retrieved included patients' demography, tumour site, tumour histology and subtypes, Helicobacter pylori status, associated gastritis, types of gastrectomy and; analysis and finding of omental deposits. Permission to conduct the study was received from Wits HREC (M121104)
Results: 325 records were found. Majority (76.6%) were adenocarcinomas and there were only few cases of GISTs and lymphoma. The overall male to female ratio of patients was 192:133 and their average age overall was 59.0 years (range: 23-102 years). The average age of patients who had adenocarcinoma was 60.2 years. Around 8.8% of patients who had adenocarcinoma were younger than 40 years.
Gastric resection was performed in 23.1% adenocarcinomas of which 9.1% was stage I. The greater omentum was part of specimen in 46.6% cases but report regarding cancer deposits was specified in 25.9% of which 11.1% were positive.
Conclusion: Pathologists do not routinely analyse and report findings on the greater omentum of patients had gastrectomy for cancer. It potential leads to under-staging. Assessment of greater omentum should be incorporated into the standard pathology reporting format for advanced gastric cancer.
PREVALENCE, DEMOGRAPHIC AND HISTOLOGICAL SUBTYPES OF HURTHLE CELL TUMOURS OF THE THYROID: A HISTOPATHOLOGICAL AUDIT
V Malith, N Harran, I Bombil,T E Luvhengo
Department of Surgery, University of the Witwatersrand
Introduction: Hurthle cell neoplasms (HCNs) account for 3-10% of thyroid carcinomas and adenomas preoperatively is difficult.
Aim: To determine factors associated with malignancy in patients who had thyroidectomy for HCNs at University of Witwatersrand teaching hospitals.
Methods: Histopathology records of patients who had thyroidectomy from January 2001 to October 2015 were reviewed. Data retrieved included indications for thyroidectomy, demographics, HCN subtypes and pre-operative FNAC results. Permission to conduct the study was
obtained Wits HREC (M150944).
Results: At total of 2641 records were found and 676 were for thyroid tumours. Around 107 cases were HCNs and 25.2% of HCNs were HCCs. Average tumor size for FCAs and FCC were 4.9 cm and 3.5 cm, respectively and the difference was statistically significant (p-value of 0.016). The risk of malignancy increased from 11.1% in FCNs less or equal to 1cm, through 33.3% for size of 1-4cm to 53.8% for tumour larger than 4cm.
Pre-operative FNAC results were available in 54.2% (58/107) and were reported as follows: suspicious for HCNs = 31, suspicious of papillary carcinoma = 7, atypia of unknown significance = 5, benign = 6 and non-diagnostic = 6. Age and gender were not significant demographical factors predictable for malignancy.
Conclusion: HCC is relatively more common in parts of South Africa than it is reported. A HCN larger than 4cm in diameter is likely to be HCC. Therefore total thyroidectomy should be considered in patients presenting with thyroid nodule greater than 4cm diameter if FNAC result suggests HCN.
BREAST CANCER: A COMPARITIVE STUDY TO EVALUATE THE DISPARITY BETWEEN PUBLIC AND PRIVATE SECTORS IN A MEDIUM INCOME COUNTRY
W C Coetzee1, J P A Apffelstaedt1, M du Plessis1; T V Zeeman2
1 Department of Surgery; Tygerberg Academic Hospital and Stellenbosch University, SA
2 Private practice, Bellville, Western Cape; SA
Introduction: Different outcomes in breast cancer have been reported for low and high socio-economic groups. We here present data quantifying disparities between South African public and private patients.
Methods: Records of 240 consecutive patients treated in 2008 in a public vs 97 patients in a private health facility were reviewed for demographic and oncologic data.
Results: The average of patients was 56.2 vs 51.9 years. Stage at presentation was 0 in 0.83 vs 25.8%, I in 4.5 vs 15.5%, II in 41.3 vs 37.1%, III in 37.1 vs 18.6% and IV in 16.3 vs 3.1% public vs private patients. Eighty percent of patients were symptomatic vs 55.7%. Of patients with stage 0 - III disease, 18 vs 20% had simple tumour excision and 7.5 vs 14 % oncoplastic tumour excision. The mastectomy rate was similar (58% vs 60%), but immediate reconstruction was performed in 10% vs 63%. For all stages, public patients were less likely to have radiotherapy. While the pathology was not significantly different, 27.2 vs 20 %, 54 vs 52%, 87 vs 61% of patients with stage I, II and III disease respectively had chemotherapy. Hormonal therapy for premenopausal patients in private was a LHRH agonist in 9.3%, ovarian ablation/BSO in 11.7% of public patients ; biologicals were given in 7.2% of patients in private, but not to any public patients. Overall survival for public vs private was 66 vs 80% (p<0.0005) months respectively. Per stage better overall survival of private patients 100% vs 100%, 72.7 vs 93.3%, 84.8 vs 88.9%, 57.3 vs 77.8%, and 33% vs 33% for stages 0, I, II, III and IV, did not reach statistical significance.
Conclusion: The greatest impact on outcome had stage at presentation, but more aggressive therapy for each stage resulted in a trend to better outcome for private patients.
DEVELOPMENT OF AN EX VIVO BREAST CANCER PLATFORM TO TEST NEW IN SILICO-DESIGNED ANTICANCER DRUGS
X X Stander1, T R Mokoena1, B Potter2, B A Stander3
1 Department of Surgery, Faculty of Health Sciences, University of Pretoria
2 Department of Pharmacology, University of Oxford
3 Department of Physiology, Faculty of Health Sciences, University of Pretoria
Introduction: Preclinical approaches such as in vitro tumorigenic cell lines, spheroids, mouse models and molecular and genetic profiling techniques are unable to capture the full complexity of the biological microenvironment of the native tumour. A highly sensitive ex vivo model system that matches an explanted tumour's three-dimensional matrix protein support, as well as a mixture of autologous ligands to maintain autocrine-paracrine loops of growth factors is desirable for drug testing.
Aim: To design and develop anticancer therapeutics and test it on an ex vivo breast tumour model.
Methods: In silico-docking using Autodock Vina and molecular dynamics using GROMACS were used to identify potential selective inhibitors of BRD4 and Sirtuin 1. The in vitro effect of BRD4 inhibitor, Sirtuin 1 inhibitor and STX1972 were assessed with spectrophotometry and flow cytometry. Fresh human breast tissue specimens from surgical discard material after mastectomy will mechanically and enzymatically digested to study tumour microenvironment. The Bio-Plex Pro™ Human Cytokine 27-plex assay will be used to study the cytokine expression of these breast cancer populations.
Results: BRD4 and Sirtuin 1 inhibitors were synthesized by WuXi AppTec (Shanghai, China) with purity greater than 95%. STX1972 is active at 35 nM on breast adenocarcinoma MCF-7 cells and metastatic breast cell line MDA-MB-231. BRD4 inhibitors CC5 and CC6 are active at micro molar concentrations (20-40 uM cell line depended).
Conclusion and future work: The study on breast cancer cell lines demonstrated the power of in silico methods for drug design. Furthermore, the development of the ex vivo model to test these new compounds has started and an optimized extracellular matrix and serum is expected by the end of 2017.
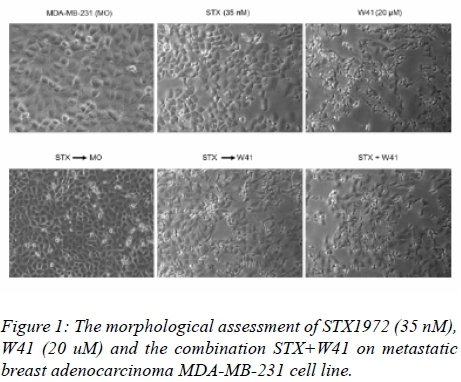
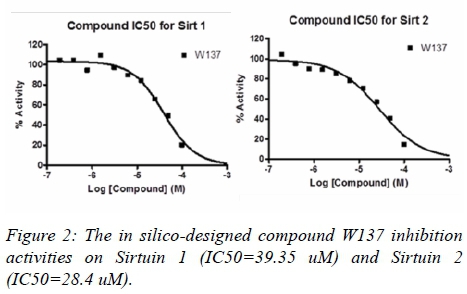
CYTOKINES AS BIOMARKERS OF PANCREATIC DUCTAL ADENOCARCINOMA: A SYSTEMATIC REVIEW
Y Y Yako1, D Kruger1, M Smith1,2, M Brand2
1 Department of Surgery, School of Clinical Medicine, Faculty of Health Sciences, University of Witwatersrand
2 General Surgery, Chris Hani Baragwanath Academic Hospital
Introduction: Pancreatic ductal adenocarcinoma (PDAC) is characterised by rapid progression to metastasis, and poor prognosis such that only 6-20% of patients undergoing radical surgical resection have a 5-year survival rate. The use of biomarkers to guide therapeutic decisions in non-pancreatic cancers is well established, but not in PDAC. Cytokines are emerging as potential biomarkers for PDAC due to their altered circulating levels in PDAC patients.
Aim(s): A systematic review of the role of cytokines in clinical medicine as diagnostic, predictive, or prognostic biomarkers in PDAC was undertaken.
Methods: A systematic review was conducted according to the 2009 PRISMA guidelines. PubMed database was searched for original articles on the topic of interest published until June 2015, and this was supplemented with references cited in relevant article. Studies were evaluated for risk of bias using the Quality in Prognosis Studies tools.
Results: Forty one cytokines were investigated in relation to PDAC in 65 studies, ten of which were analyzed by more than three studies. Six cytokines (interleukin[IL]-1β, -6, -8, -10, vascular endothelial growth factor, and transforming growth factor) were consistently reported to be increased in PDAC and associated with the disease severity by more than four studies; irrespective of sample type; method of measurement; or statistical analysis model used. When evaluated as part of distinct panels that included CA19-9; IL-1β, -6 and -8 improved the performance of CA19-9 alone in differentiating PDAC from healthy controls. IL-2, -6, -10, VEGF, and TGF levels were reported to be altered after patients received therapy or surgery.
Conclusion/Recommendations: Our review demonstrated that there is insufficient evidence to support the role of individual cytokines as diagnostic, predictive or prognostic biomarkers for PDAC. However, emerging evidence indicates that a panel of cytokines may be a better tool for discriminating PDAC from other non-cancer individuals.
HOW LONG ARE ELDERLY BREAST CANCER PATIENTS FOLLOWED UP WITH MAMMOGRAM AFTER THE DIAGNOSIS OF BREAST CANCER? A SINGLE CENTRE EXPERIENCE IN A DEVELOPING COUNTRY
Y Parag1, I Buccimazza2
1 Department of Radiology, Department of General Surgery, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban
2 Breast Unit, Department of General Surgery, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban
Introduction: The impact of breast cancer on elderly South African patients is not well characterised.
Aims: Our study aims to assess the impact of breast cancer and adherence to post-treatment surveillance programmes amongst the local elderly population attending the Breast Oncology Clinics at Addington and Inkosi Albert Luthuli Hospitals in KwaZulu-Natal.
Methods: A retrospective review was undertaken of all patients aged 65 years and older diagnosed with breast cancer during 2007. Hospital records were reviewed for a period of 5 years to ascertain stage of disease, treatment received, adherence to post-treatment surveillance mammogram, incidence of new mammographic findings and recurrence, site of recurrence and its mode of detection, disease free survival and overall survival rates at 5 years. Patients with a second malignancy and those with an incomplete dataset were excluded from the study. Data was analysed using the Statistical Package for Social Sciences (SPSS version 21). Survival analysis was recorded using the Kaplan Meier Curve. Institutional approval was obtained from the hospitals' management and from the University of KwaZulu-Natal Biomedical Research Ethics Committee (BE072/13).
Results: The incidence of breast cancer in the elderly population was 26.7%. A significant percentage of patients (56.3%) were diagnosed at an advanced stage of disease. Of the 46.9% who had surveillance mammograms, only 6.3% of patients received their post-treatment surveillance mammograms on time. New mammographic findings were detected in 26.7% of patients during the 5 year follow-up. 15.6% of the total study number of patients presented with disease recurrence during the follow-up period. 80% of cases of recurrence were detected clinically. The overall survival at 5 years was 65.6%.
Conclusion: Our study highlights the significant number of elderly patients with advanced disease at diagnosis, poor compliance with internationally recommended annual post-treatment surveillance mammograms, and the relatively low overall 5 year survival rate when compared to international studies.
"NIPPLE NIRVANA" - A NOVEL METHOD OF NIPPLE-AREOLA COMPLEX RECONSTRUCTION IN PATIENTS WITH MACROMASTIA
Y Brakovsky1, I Buccimazza2
1 Department of Plastic and Reconstructive Surgery and Breast Unit, I.A.L.C.H. Durban
2 Department of Surgery and Breast Unit, I.A.L.C.H. Durban
Introduction: Nipple-Areola Complex (NAC) reconstruction remains a challenge despite the multitude of methods described. We propose reconstruction of the NAC in patients with macromastia using the skin/ part of the areola from the reduced breast as an axial - Internal Mammary Perforator flap.
Aim(s): To assess the functional and aesthetic results of NAC reconstruction using the above method.
Methods: This was a retrospective study of all patients undergoing NAC reconstruction at I.A.L.C.H. between April 2015 and March 2016. All patients with NAC reconstruction by IMAP flap were included. Patients undergoing NAC reconstructions by other methods were excluded. Data captured included demographics, type of reconstruction, complications, measurements of areola size, nipple projection, comparison between sides, NAC sensation and patient satisfaction via a questionnaire .
Ethics approval was obtained: BE504/15
Results: Seven patients were included. The majority were urban patients who had an immediate breast reconstruction. There were three surgical complications of which two were minor. In four patients the shape /projection was maintained as compared to the opposite side. The sensation was preserved in four of the reconstructed nipple-areola complexes. The majority of patients were pleased with the results.
Conclusion/Recommendations: We describe a novel method to reconstruct a realistic-looking, sensate NAC in women with macromastia requiring a mastectomy for breast cancer. Overcorrection with regards to NAC size is necessary as partial loss of projection occurs. Preservation of sensation is unpredictable but occurs in the majority of patients.
RECEPTOR STATUS IN RECURRENT BREAST CANCER- A RETROSPECTIVE STUDY
Z Ally
Background: Breast cancer recurrence is a major clinical manifestation and represents a principal cause of breast cancer related death.There has been demonstrated a discordance rate between receptor status of primary and matched recurrence specimens, however the extent of this is not well-known. Repeating immunohistochemistry has financial and workforce implications in a resource-constrained environment, therefore it is important to determine the extent of change between specimens.
Aim: To compare the hormone receptor status between breast cancer primary and matched loco-regional recurrence to ascertainreceptor status discordance.
Methods: Beginning in 2006, all patients who presented to the respective breast care facilities with breast cancer recurrences were identified using the mammography department records. The specimens for each patient werescrutinized, oestrogen and progesterone receptor status and HER2 receptor status were noted for each patient and a comparison was made between primary, and recurrence, with loss and gain being noted.
Results: During this analysis, significant discordances were found for hormone receptor status between primary and matching recurrent samples. Switching of oestrogen receptor status occurred in 14% of patients (switching occurred both from ER-positive to -negative and vice versa) and for progesterone receptor status it occurred in 25%. A total of 40% discordance was found for HER2 receptor status. These results are not dissimilar to what has been previously reported in the literature. Of note, adverse receptor discordance (positive to negative) was noted in a total of 33 receptors ( ER 4 ; PR 11 ; HER2 18).
Conclusion: These results confirm the phenomenon of receptor discordance between breast cancer primary and recurrence. The results support the necessity of confirming receptor status on all possible and proven recurrent disease, thus reinforcing the importance of obtaining a confirmatory biopsy when patients present with suspicion of recurrent disease.


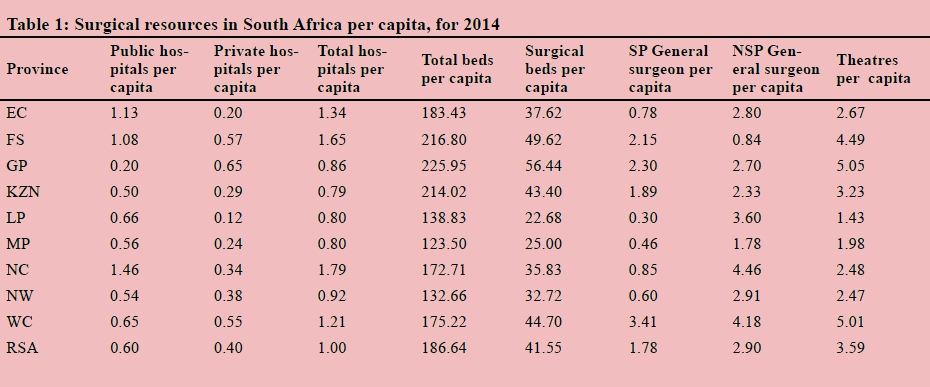{kind=link}
{kind=link}
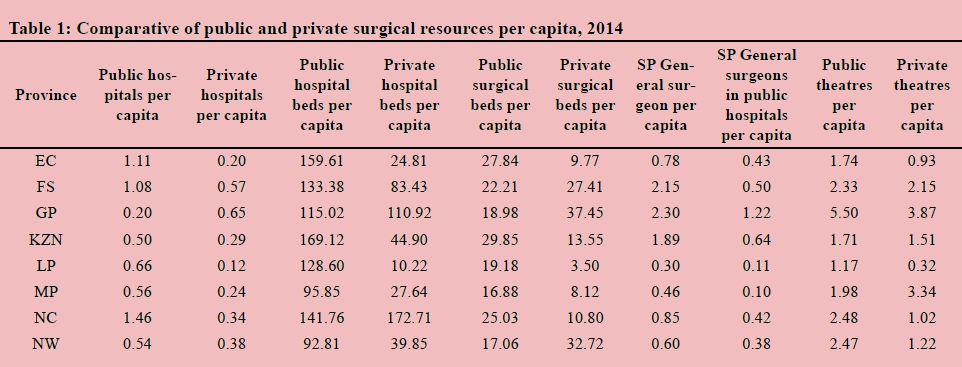{kind=link}
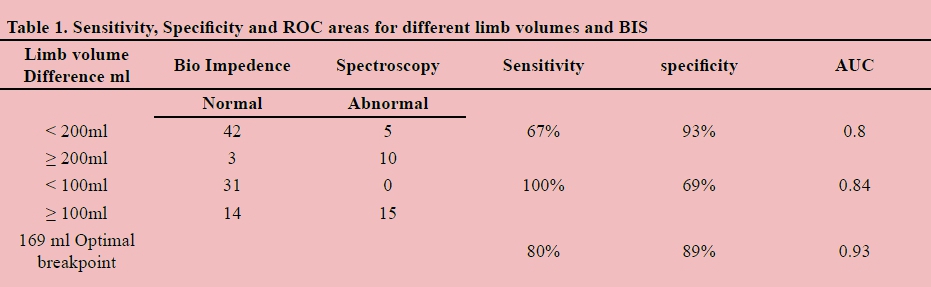{kind=link}
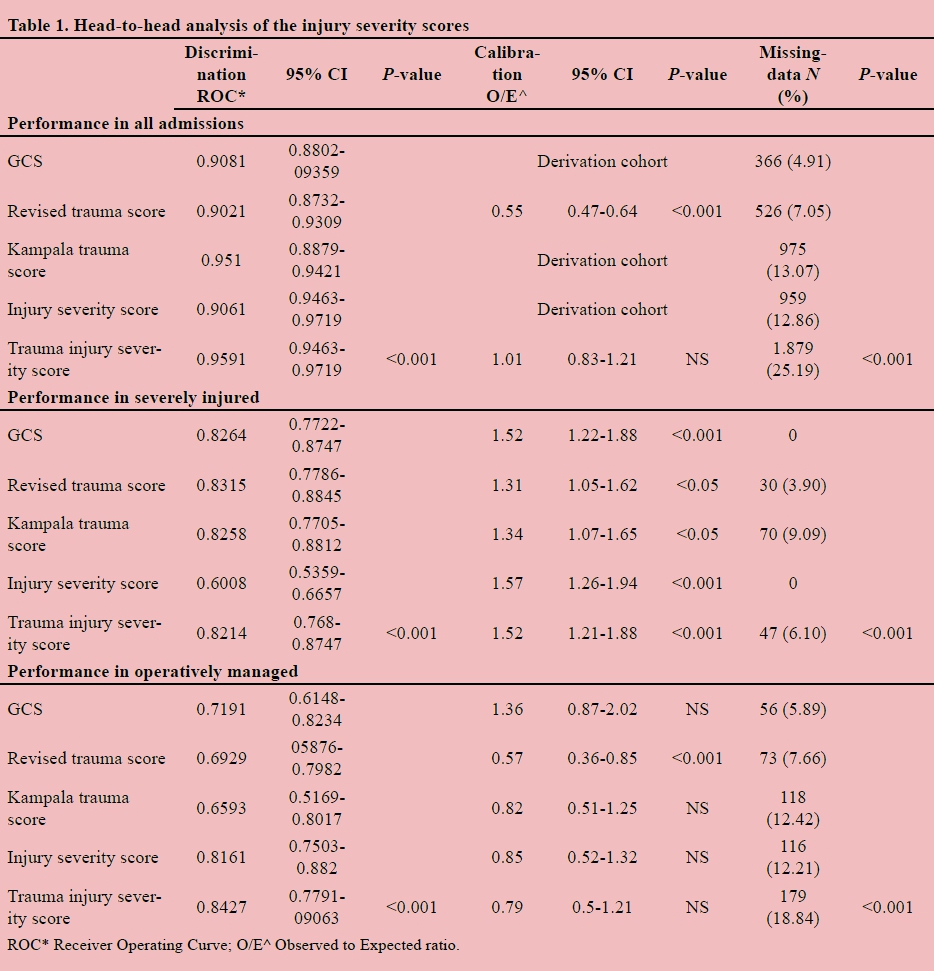{kind=link}
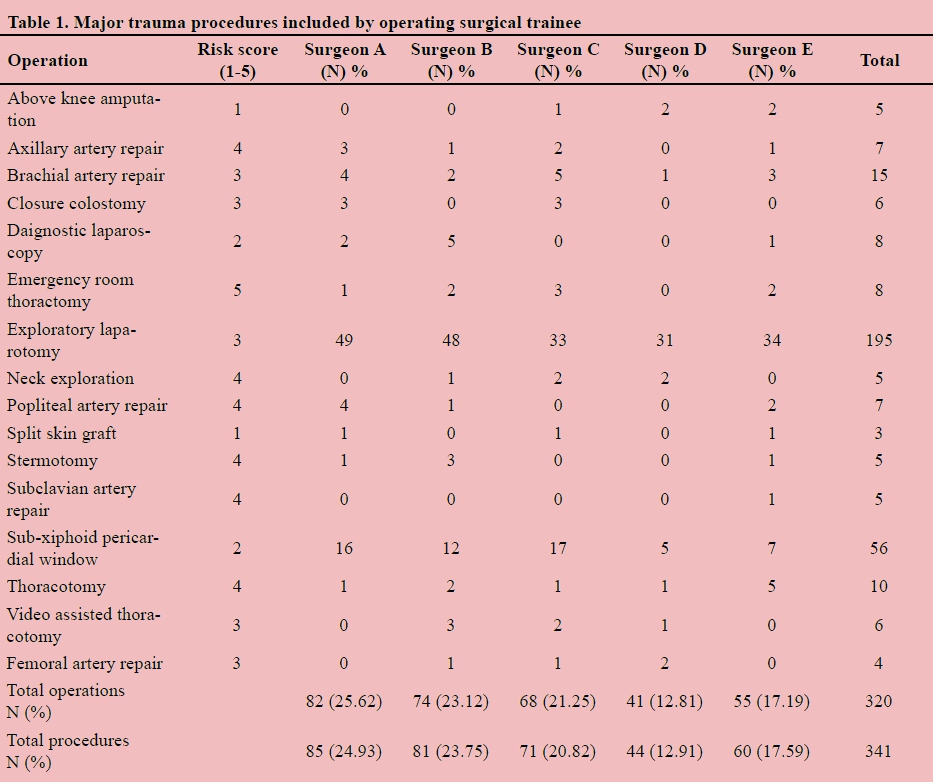{kind=link}
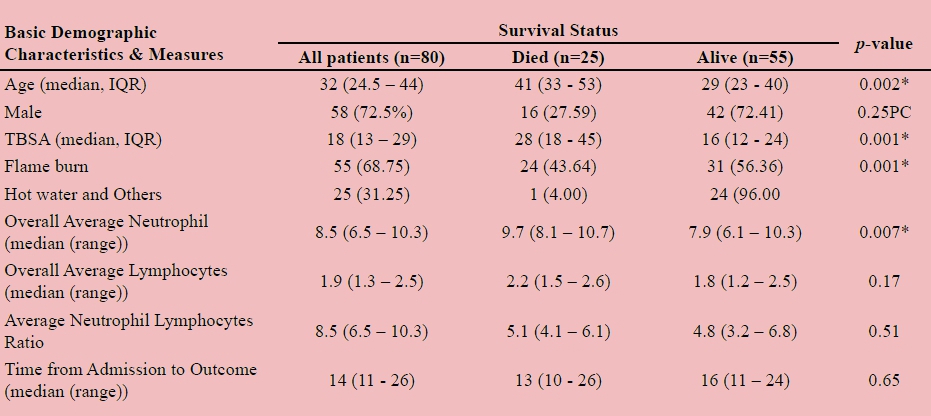{kind=link}