










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Surgery
versión On-line ISSN 2078-5151
versión impresa ISSN 0038-2361
S. Afr. j. surg. vol.54 no.2 Cape Town jun. 2016
CASE REPORT
It's not inside, it's on top! - An unusual cause of right iliac fossa pain
N SinghI; M GovenderII
IRegistrar, Department of General Surgery, Sefako Makgatho Health Sciences University
IIHead of Clinical Unit, Department of General Surgery, Sefako Makgatho Health Sciences University; Dr George Mukhari Academic Hospital
ABSTRACT
Rectus sheath haematoma (RSH) is an uncommon cause of acute abdominal pain, but can mimic a variety of acute surgical conditions. Computed tomography (CT) provides the diagnosis and avoids unnecessary procedures.
A 72-year-old female presented with acute-onset right iliac fossa pain, without any other symptoms. She had no co-morbidities and was not taking any chronic medication. Her previous surgical history included a previous Caesarean section at the age of 42 years. On examination, she was apyrexial, with tenderness in the right iliac fossa region. There were no palpable masses, but ecchymosis developed in the right suprapubic region on day 3 post the onset of pain (Figure 1).

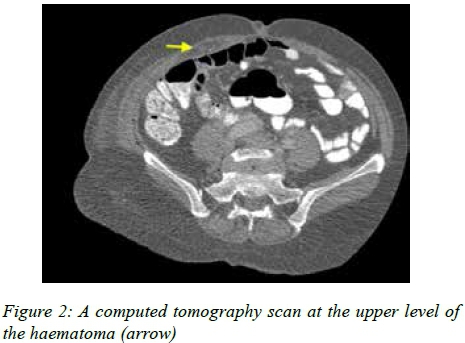
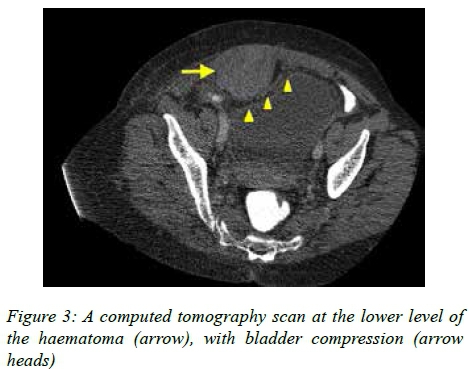
The patient's leucocyte count and C-reactive protein level were normal. Intra-abdominal pathology was not indicated on the abdominal sonar. A haematoma in the right lower rectus sheath was demonstrated on the CT scan of the abdomen (Figures 2 and 3).
On further inquiry, the patient admitted to performing abdominal crunches as part of a new exercise programme for the elderly. She improved on simple analgesia and was discharged on day 3.
Discussion
RSH is an unusual cause of acute abdominal pain, which can be mistaken for other surgical conditions.1 The source of haemorrhage in the rectus sheath is from branches of the inferior epigastric artery, or from a tear in the muscle.2 Most RSH are posterior to the muscle due to the anatomical location of the inferior epigastric artery and can occur spontaneously or post procedural. Some risk factors documented include anticoagulation therapy, bleeding disorders, hypertension, atherosclerosis, cough and physical exercise.
The typical presentation of a RSH is the triad of acute abdominal pain, abdominal wall mass and a decrease in the haemoglobin level,3 but patients may complain of non-specific symptoms, such as vomiting, nausea and fever. Cullen's and Grey-Turner's signs rarely occur, and suggest concomitant retroperitoneal haemorrhage, when present. Patients may present with an acute abdomen and hypovolaemic shock on severe cases. These symptoms and signs have a wide differential diagnosis, ranging from acute cholecystitis and appendicitis, to acute pancreatitis and a ruptured abdominal aortic aneurysm.
Two clinical examinations have been described to assist in differentiating abdominal wall pathology from intra-abdominal pathology. Both require examination of the patient's abdomen while supine. The patient is then asked to tense his or her anterior abdominal wall muscles by raising his or her shoulders from the bed.
Carnett's sign identifies the point of maximal abdominal tenderness, which worsens if the pathology is within the abdominal wall. If the tenderness is alleviated, then the pathology is likely to arise from the abdominal viscera as the contracted rectus muscle now protects the intra-abdominal contents.
Fothergill's sign is used for abdominal masses. If a mass lies intra-abdominally, the mass will be concealed when the patient tenses the anterior abdominal wall muscles, but if the mass arises from the abdominal wall, it will remain palpable.
These signs are sensitive for abdominal wall pathology, but not necessarily specific.1
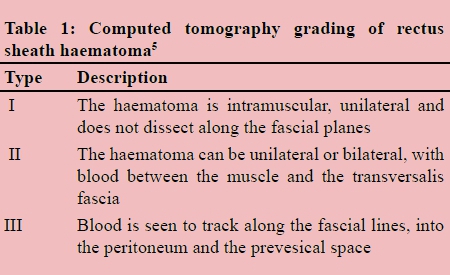
However, a CT scan is 100% sensitive and 100% specific in acute RSH,4 and it is used to classify RSH (Table 1). This classification, first proposed by Berna et al.,5 is used to guide management. Hospitalisation is not required for type I RHS, but types II and III require hospitalisation and a possible blood transfusion. Angiography and embolisation are used successfully in cases where patients continue to bleed. If these fail, or are unavailable, surgical exploration and ligation of the culprit vessel is mandatory.
REFERENCES
1. Fitzgerald JFE, Fitzgerald LA, Anderson FE, et al. The changing nature of rectus sheath haematoma: case series and literature review. Int J Surg. 2009;7(2):150-154. [ Links ]
2. Kapan S, Turhan AN, Alis H, et al. Rectus sheath hematoma: three case reports. J Med Case Rep. 2008;2:22. [ Links ]
3. Papadimitropoulos K, Condilis N, Philippou P, Birbilis A. Rectus sheath haematoma. Report of two cases. Ann Ital Chir. 2007;78(5):447-450. [ Links ]
4. Sullivan LEJ, Wortham DC, Litton KM. Rectus sheath hematoma with low molecular weight heparin administration: a case series. BMC Res Notes. 2014;7:586. [ Links ]
5. Berna JD, Garcia-Medina V, Guirao J, Garcia-Medina J. Rectus sheath hematoma: diagnostic classification by CT. Abdom Imaging. 1996;21(1):62-64. [ Links ]
 Correspondence:
Correspondence:
Natasha Singh
natasha_singh1230@yahoo.com

