










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.54 n.1 Cape Town Mar. 2016
TRAUMA SURGERY
An urban trauma centre experience with abdominal vena cava injuries
M HamptonI, II; D BewI, II; S EduI, II; A NicolI, II; N NaidooI, II; P NavsariaI, II
ITrauma Centre and Vascular Surgery Unit, Groote Schuur Hospital, Cape Town, South Africa
IIFaculty of Health Sciences, University of Cape Town, Cape Town, South Africa
ABSTRACT
BACKGROUND: The aim of the study was to present the surgical management of injuries to the abdominal vena cava (AVC) and to identify clinical and physiological factors and management strategies which affect the outcome.
METHODS: A retrospective review was conducted of AVC injuries in patients attending the trauma centre at Groote Schuur Hospital, Cape Town, from January 2003 to December 2011. Demographic data, mechanism and agent of injury, level of injury, physiological parameters, associated injuries, trauma scores, management strategy, morbidity and mortality, and length of hospital stay were taken from the trauma centre's operative databank at Groote Schuur Hospital.
RESULTS: Thirty-five patients with AVC injuries were identified. There were 33 penetrating injuries (94%). Gunshot wounds accounted for 28 of them (85%). There were 19 (54%) infrarenal, 9 (26%) juxtarenal, 3 (7%) suprarenal and 4 (11%) retrohepatic AVC injuries. Most patients were treated with ligation (66%). There were 17 (49%) deaths. There were significant differences in the preoperative systolic blood pressure (p = 0.044), number of red cell units transfused (p = 0.001), serum lactate (p = 0.007), arterial pH (p = 0.002) and preoperative temperature (p = 0.000) between the survivors and non-survivors. There was also a significant difference in ligation versus repair between the two groups (p = ≤ 0.000). There was no difference in the injury severity, level of injury and the number of associated injuries between survivors and non-survivors.
CONCLUSION: AVC injuries are associated with high mortality. Patients presenting with clinical and physiological evidence of shock and who require "damage control" surgery are more likely to suffer a worse outcome, particularly when multiple physiological derangements are present. Patients who died often have severe associated injuries.
Injuries to the abdominal vena cava (AVC) are rare, and occur more commonly following penetrating (0.5-5.0%) than blunt (0.6-1.0%) trauma. They are associated with a high mortality. The best reported survival rate in modern trauma centres is approximately 33%. The incidence of trauma to the AVC appears to be increasing. Some centres have reported that it constitutes up to 40% of all abdominal vascular injuries.1 The management of these injuries is usually challenging since they are rarely isolated, and are often associated with serious adjacent solid and/or hollow visceral injuries, as well as devastating concomitant major arterial injuries. Patients are frequently haemodynamically unstable, and require the utilisation of multiple resources, including blood products, anaesthetic care, theatre time and often prolonged intensive care unit stay, which often involves organ-supportive measures to ensure an optimal outcome. General surgeons manage the majority of South African trauma patients, and have to be comfortable managing all types of major abdominal vascular trauma. The management principles of vascular trauma in haemodynamically unstable patients have evolved over the last 30 years. The concept of "damage control" surgery has become the guiding principle. Complex time-consuming anatomical repairs of major vascular injuries are foregone, and temporary measures such as shunting, or non-corrective measures, such as ligation, are instead utilised. These techniques are relatively easy to execute and do not take much time. The majority of patients with AVC injuries meet the criteria for damage control surgery, and ligation of the AVC is a frequent strategy. Although there is little doubt that this is a lifesaving measure, the associated morbidity after caval ligation has not been clearly elucidated. Thus, the objective of this study was to review and report on the surgical management of AVC injuries in the trauma centre at Groote Schuur Hospital.
Aim
The aim of the study was to present the surgical management of injuries to the AVC, and to identify the clinical and physiological factors and management strategies that affect the outcome.
Method
The study was a retrospective chart review of AVC injuries managed in the trauma centre at Groote Schuur Hospital from January 2003 to December 2011. The study was approved by the University of Cape Town's Faculty of Health Sciences Human Research Ethics Committee. Patients were identified from the trauma centre's operative logbook, and their records obtained from the hospital records department. Patients with generalised peritonitis and/or an abdominal cause for haemodynamic instability underwent an emergency laparotomy. Demographic data, mechanism and agent of injury, level of injury, physiological parameters, associated injuries, trauma scores, management strategy, morbidity and mortality, and length of hospital stay were captured from the patient charts.
Statistical analysis was performed using Stata® version 11. For descriptive purposes, mean ± standard deviation was calculated for continuous variables, and proportions were used for the categorical variables. To determine the difference in the mean continuous variables, Student's t-test and oneway analysis of variance tests were applied, when appropriate. Chi-square and Fisher's exact tests were used to determine the association between the categorical variables. Statistical significance was defined at a level of p = ≤ 0.050.
Results
Thirty-five patients with AVC injuries were identified during the nine-year study period. There were 29 men and six women, with a mean age of 27 years, and an age range of 15-45 years. Thirty-three of the injuries were caused by penetrating trauma (94%), of which gunshot wounds accounted for 28, and stab wounds, four. There was one shotgun injury. The 2 blunt injuries (6%) were caused by road traffic accidents. There were 19 (54%) infrarenal, 9 juxtarenal (26%), 3 suprarenal (9%) and 4 retrohepatic (11%) caval injuries. There were 17 deaths (49%).
The means of the first recorded physiological parameters of the patients in the trauma centre are shown in Table 1.

The mean Revised Trauma Score and Penetrating Abdominal Trauma Index were 6.93 ± 1.48 (a range of 2.6-7.8) and 41.52 ± 13.06 respectively (a range of 12-61). The median Injury Severity Score (ISS) was 34, with an interquartile range of 16 (25-41).
Liver injuries (18) were the most common associated intra-abdominal injury, followed by large bowel injuries (13). There were a further 12 associated duodenal and 12 small bowel injuries (Table 2). All of the patients had at least one associated intra-abdominal injury. More than half of the patients sustained at least two intra-abdominal injuries. Extra-abdominal injuries were less common. A total of 63% of patients had at least one such injury. There were 14 associated extra-abdominal injuries in the 33 patients who sustained penetrating IVC injuries. There were two vertebral body fractures, one penetrating brain injury from a gunshot wound to the head, one brachial plexus injury, one spinal cord injury, two hand fractures, three haemothoraces, one pelvic fracture, one brachial artery injury and two femur fractures.

There were 11 associated extra-abdominal injuries in the two patients who sustained blunt IVC injuries. These were mainly pelvic and long bone fractures, as well as blunt chest trauma with haemothoraces.
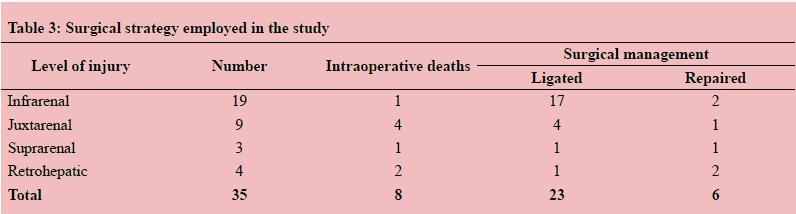
A trauma consultant surgeon was present at 30 of the 35 operations performed (86%). A senior trauma registrar was present in all the cases when a consultant was not present. The patients required a mean of 10 (a range of 2-43) units of packed red cells during the first 24 hours of management. AVC injuries were managed with ligation in 23 patients (66%). Intraoperative demise occurred in two patients due to the consequences of exsanguination after caval ligation had been performed. The first of these patients had sustained a retrohepatic caval injury with a major concommitant liver injury, for which haemostasis was not possible. The second patient had sustained multiple gunshot wounds and had a large haemothorax, penetrating injuries to the large and small bowel, as well as a penetrating injury to one of his brachial arteries. Repair of the AVC was performed in 6 patients (17%) (Table 3).
Of the 17 deaths, eight occurred intraoperatively due to exsanguination, with a further three occurring within 48 hours of presentation due to intractable coagulopathy. Five more patients demised after 48 hours due to multiple organ dysfunction syndrome with sepsis, while care was withdrawn from one patient with severe hypoxaemic brain injury.
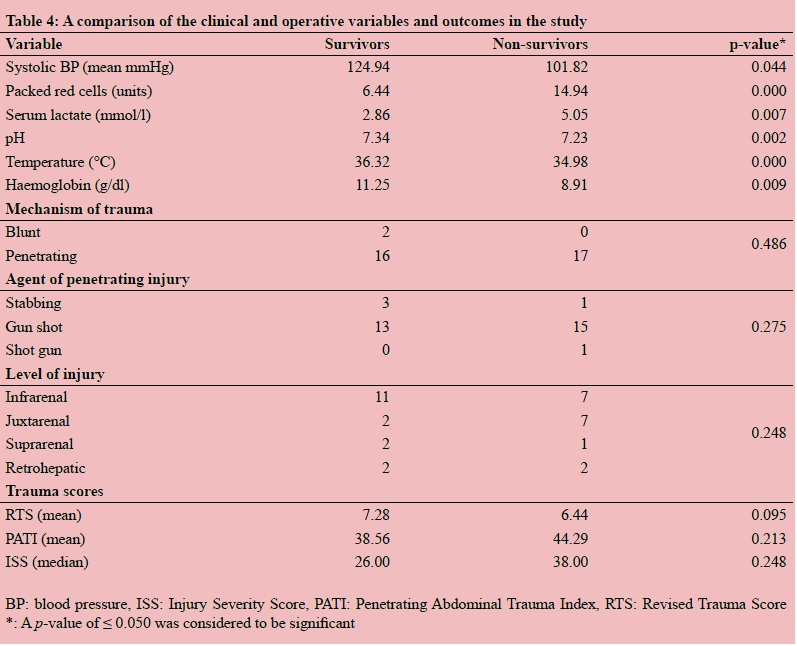
There was an overall mortality rate of 49%. Significant differences between the survivors and non-survivors in this series were found with respect to systolic blood pressure (SBP), the number of packed red cells required in the first 24 hours, serum lactate concentration, pH on the initial arterial blood gas analysis, the first recorded temperature and haemoglobin concentration. When the mechanism of injury, the agent of injury, the level of the injury, or the trauma score values were evaluated, there was no statistical association between the groups of survivors and non-survivors. The number of associated intra-abdominal injuries was not statistically different between the groups of survivors and non-survivors (p = 0.165) (Table 4). There was also no statistical difference between the groups who survived or demised with regard to the number of associated extra-abdominal injuries (p = 0.384). Differences in the physiological parameters were analysed between the survivors and non-survivors to detect whether values outside of the normal established range for a particular parameter would significantly predict an adverse outcome; in this case, death. The parameters analysed in this way included SBP, temperature and serum lactate concentration. The normal ranges and values were as follows: SBP ≥ 90 mmHg, temperature ≥ 36°C, serum lactate ≤ 2.5 mmol/l and base deficit ≤ - 4.0.
A serum lactate level of ≥ 2.5 mmol/l was found to be significantly associated with an adverse outcome (p = 0.042) in this series of patients, although some patients survived with levels in this range. There was a significant association between a temperature of ≤ 36.0°C and death (p = 0.042), although six survivors had a temperature of ≤ 36 °C on arrival. A significant association was not found between a SBP of ≤ 90 mmHg and mortality (p = 0.146). There was a trend towards a significant difference between the groups of survivors and non-survivors when the base deficit of greater or less than -4 was evaluated (p = 0.057). Death was the outcome for patients in the presence of a SBP ≤ 80 mmHg, serum lactate ≥ 2.5 mmol/l and a temperature ≤ 36.0 °C on admission. The situation was significantly different in those who did not have this combination of derangement (p = 0.019).
Three patients developed bowel obstruction in the post-surgical period. They were managed with laparotomies and adhesiolysis of the obstructing bands. One patient with a retrohepatic AVC injury also had an injury to the common bile duct. The common bile duct was repaired at the "relook" laparotomy, but the patient subsequently developed a common bile duct stricture and required a hepaticojejunostomy.
One patient with an intimal flap injury to his left common iliac artery, repaired with a polytetrafluoroethylene graft, developed graft sepsis for which an extra-anatomical femorofemoral bypass was required. Three patients developed deep vein thrombosis (DVT) during their index admission. There was no association between the risk of DVT and the strategy used to repair an AVC injury (ligation or repair) in this series (p = 0.481), although the small number of cases may have influenced this. There was one nonocclusive common femoral DVT, one iliofemoral DVT and one infrarenal vena caval free-floating thrombus that had been diagnosed in a patient who had been managed with a venous repair of a penetrating injury to the retrohepatic AVC. All three of these patients were followed-up after discharge at the trauma clinic in order to manage the ongoing oral anticoagulation, as well as to search for evidence of chronic venous insufficiency. The former two patients were managed with extended oral anticoagulation and compression stockings. Symptoms of chronic venous insufficiency were not reported at their subsequent clinic visits. The patient who developed free-floating caval thrombus was managed with the placement of a removable inferior vena cava filter. The filter was left in situ for a period of eight weeks while anticoagulation was established, and was subsequently recaptured and removed. This patient has been seen frequently in the follow-up clinic, and is now undergoing annual venous duplex surveillance of his AVC and deep leg veins. The first duplex surveillance performed at one year post injury was normal, with no evidence of chronic venous disease. His oral anticoagulation was stopped at this visit. Although evidence of postphlebitic changes in the deep veins of the thighs and AVC was demonstrated in the duplex examination performed one year later (Figure 1), the patient was well, and complained only of occasional swelling symptoms in his legs. He continues to be followed-up and uses compression stockings.

Follow-up of the patients who were discharged after successful management of their injuries was completed in seven of the 18 survivors (39%). The remaining patients were discharged to their local hospital. Some were seen once in the trauma outpatient clinic after one month and discharged, while one is undergoing long-term follow-up, and has been seen annually for the last three years. Of the seven patients who were followed-up, five have been managed with AVC ligation, and two with repair of the injury.
Discussion
AVC injuries continue to be associated with a high rate of mortality. A third of all patients die of their injuries before reaching hospital, and a further 30% die within 24 hours of hospital admission, due either to the consequences of exsanguination, or the resultant coagulopathy associated with major trauma.2 A further group of patients develop multi-organ dysfunction syndrome, and succumb to the consequences of the associated abdominal and extra-abdominal injuries.
Although the mortality rate of 49% in this series is comparable to that from other reported series, the increased rate of mortality seen, compared to that in the initial report by Navsaria et al., with respect to our institution, was concerning.3 There were no clearly identifiable reasons why this occurred, except for the fact that it is possible that the paramedic service has improved to such an extent that patients who would previously have demised before reaching the hospital are now reaching it earlier, suggesting that we are possibly treating patients who are initially more unstable than they were in the past. The numbers are not different when comparing the penetrating AVC injuries attributable to the different injuring agents in this series and those in the original study by Navsaria et al. The number of gunshot wounds is similar, and therefore the increase in the mortality rate in this series was not because of a higher number of gunshot wounds. A recent published report from Pretoria on a similar-sized patient cohort, with similarly distributed injuries to the abdominal cava, showed that 100% of the injuries in that series were caused by abdominal gunshot wounds with low-calibre weapons.4
It was shown in our study, and has been demonstrated in others, that basic physiological parameters, which should be measured on all trauma patients on admission, vary significantly between the group of patients who survive and those who do not. It was also demonstrated in our study that certain abnormalities with regard to these basic parameters were significantly predictive of an adverse outcome in our group of patients, especially when patients had a combination of physiological derangement. Thus, the use of emergency department thoracotomy, with aortic cross-clamp, is advocated in victims of penetrating trauma who are haemodynamically unstable and unresponsive to resuscitative efforts in the emergency department. Despite this, patient outcomes in this situation have remained dismal in all series.
Damage control principles should be readily utilised in patients with injuries to the AVC owing to the high likelihood of associated major injuries. Early recognition of these patients in the emergency department is possible with the use of simple measurements, i.e. the patient's vital signs, haemoglobin and serum lactate concentration. An abbreviated laparotomy in an unstable, bleeding patient is the optimal management, and rapid and definitive control of the major haemorrhage is required.
It was found in this series that the majority of injuries (approximately 80%) involved the infrarenal and juxtarenal cava. Although a statistically significant association between the likelihood of survival and the level of injury was not found, of the patients who survived, a high percentage (67%) of them had infrarenal injuries.
There were slightly fewer infrarenal injuries in this series than those found in the original series by Navsaria et al., where more than 85% of the injuries were infrarenal or juxtarenal, although this change is unlikely to represent true statistical difference.3
The first goal of damage control surgery, which is to stop major bleeding, is rapidly achieved with ligation of the AVC. It was found in our study that the group of patients who did not survive in this series was more likely to have been managed with caval ligation (p < 0.000), which may indicate that ligation was performed in only the most unstable patients with the worst injuries.
Infrarenal caval ligation is generally simple and its use as a lifesaving means of haemorrhage control in the appropriate circumstances is advocated. The rate of ligation in this series (63%) was similar to that in the previous series of AVC injuries at our institution that were reported by Navsaria et al.3 There is a definite role for caval repair when the patient is physiologically and haemodynamically stable, and able to tolerate a longer operation. The patients were more likely to have been part of the group of survivors (p = 0.005) in this series where the abdominal vena caval injury was managed with primary repair. The Pretoria group performed caval ligation much less frequently (in four of 27 patients) in their series. They also reported good success with caval repair in stable patients with easily accessible injuries. Fourteen of the 27 patients in their series underwent successful venorrhaphy, which illustrates the usefulness of this technique in the right set of circumstances.4 This is likely to be in a setting where a stable zone 1 retroperitoneal haematoma (between the diaphragm superiorly, the psoas muscles laterally and the pelvis inferiorly) has been recognised, and proximal and distal vascular control has been achieved, as recommended by the Durban group in its recent publication on the management of retroperitoneal haematomas following penetrating abdominal trauma.5
Some success has been achieved at our hospital in performing perihepatic packing for initial haemorrhage control via tamponade for injuries to the retrohepatic cava, and by subsequently performing a delayed retrohepatic caval repair. This was achieved without the use of deep hypothermic arrest and bypass, but it is acknowledged that some retrohepatic caval injuries may be better served using this technique. Atriocaval shunting has not been utilised, nor do we have any experience using laparoscopic methods of caval repair. Laparoscopic methods of repair are only really suitable in the setting of iatrogenic caval injury during an elective laparoscopic operation when the patient has not been subjected to a major physiological insult. The approach should be the same when using endovascular stent grafting of the cava. Although these are elegant techniques and have been shown in some case reports to be feasible in certain circumstances, their use should not be supported in patients who have sustained multiple injuries, and who require damage control surgery.6,7
Significant differences were found in our series with regard to the SBP, number of packed red cell units required by the patient in the first 24 hours, pH and serum lactate concentration in the initial arterial blood gas analysis, and core temperature and haemoglobin levels, between the survivors and non-survivors. This is in accordance with the findings in other published series.3,8 Statistically significant associations between these groups were not found when the mechanism of injury, the agent causing the penetrating injury, the level of injury and the trauma scores were analysed. This is in contrast to the previous series on our institution reported by Navsaria et al., where the ISS scores were significantly different between the survivors and non-survivors.3 Again, this may indicate an improvement in the paramedic services, in that very sick patients are now accessing our services more quickly, and because of changes in referral patterns, with the result that secondary drainage hospitals are being bypassed, and polytrauma patients are being brought directly to the centre. There was also no difference between the survivors and non-survivors in this series in terms of the number of associated injuries, nor was there a difference in the outcome whether or not a trauma consultant surgeon was present at the operation, also in accordance with the original study reported from our institution.
On further analysis of the data, a serum lactate level ≥ 2.5 mmol/l in the initial arterial blood gas analysis and a core temperature of ≤ 36 °C was found to be significantly associated with an adverse outcome. There was a trend towards significance for an adverse outcome when there was derangement in the base deficit. When more than one baseline physiological derangement was reported in patients, this was significantly associated with the outcome of death. It is suggested that rapid identification of derangement in polytrauma patients, together with targeted resuscitative therapy and early surgery, could help to lower the high mortality rate in patients with this devastating injury in the future. This leads to the question of whether or not futile damage control operations can be avoided by opting to not actively manage profoundly hyperlactataemic and hypothermic patients.
In order to address this question, Karinos et al. devised a formula that incorporated the age of the patient, the pH and temperature, to identify patients in whom active treatment would be futile.9
There has been some controversy in the literature regarding the use of prophylactic lower limb fasciotomies in situations when caval ligation has been performed. This intervention has never been performed in two series of AVC injuries at our institution. AVC ligation rates in excess of 60% were reported
in both series. In general, sufficient extra caval collateral venous pathways are available for blood to pass through on its return from the lower limbs to the right side of the heart. These pathways have been demonstrated in radiological studies.10 The occurrence of an acute obstruction to venous outflow from the leg, which is severe enough to result in a lower limb compartment syndrome, is extremely rare. Therefore, prophylactic fasciotomy of the lower limb is not justified. Although two of the surviving patients in this series, who had been managed with AVC ligation developed DVT, both were managed conservatively, and there was no evidence of postphlebitis syndrome at follow-up in either patient. A statistical association between AVC ligation and an increased risk of DVT was not found in this series.
Conclusion
Trauma teams and surgeons are often presented with difficult management problems when they encounter patients with injuries to the AVC. Usually, such patients are haemodynamically unstable, and are often at risk of the coagulpathy of trauma; now a well described and often fatal entity.
The highest risk of death is associated with patients who present with more than one isolated physiological derangement on arrival at the emergency unit.
Ligation of the vena cava has been described in this study and in others as a reasonable and time-efficient technique used to arrest haemorrhage from a blunt or penetrating injury to it; the cornerstone tenet of damage control surgery.
Pre-hospital triage of patients with potential major abdominal vascular injuries is strongly advocated with the use of simple measures such as taking the patient's vital signs and determining his or her baseline haemoglobin so that delays at centres without the necessary means to manage such patients can be avoided.
The majority of these patients require management at a dedicated trauma centre with the early institution of damage control principles if they are to have a chance of surviving this potentially devastating injury.
REFERENCES
1. Asensio JA, Chahwan S, Hanpeter D, et al. Operative management and outcome of 302 abdominal vascular injuries. Am J Surg. 2000;180(6):528-533. [ Links ]
2. Buckman RF, Pathak AS, Badellino MM, Bradley KM. Injuries of the inferior vena cava. Surg Clin N Am. 2001;81(6):1431-1447. [ Links ]
3. Navsaria PH, De Bruyn P, Nicol AJ. Penetrating abdominal vena cava injuries. Eur J Vasc Endovasc Surg. 2005;30(5):499-503. [ Links ]
4. Van Rooyen PL, Karruseit VOL, Mokoena T. Inferior vena cava injuries: a case series and review of the South African experience. Injury. 2015;46(1):71-77. [ Links ]
5. Manzini N, Madiba TE. The management of retroperitoneal haematoma discovered at laparotomy for trauma. Injury. 2014;45(9):1378-1383. [ Links ]
6. Hua Xie, Teach JS, Burke AP, et al. Laparoscopic repair of inferior vena caval injury using a chitosan-based hemostatic dressing. Am J Surg. 2009;197(4):510-514. [ Links ]
7. De Naeyer G, Degrieck I. Emergent infrahepatic vena cava stenting for life-threatening perforation. J Vasc Surg. 2005;41(3):552-554. [ Links ]
8. Sullivan PS, Dente CJ, Patel S, et al. Outcome of ligation of the inferior vena cava in the modern era. Am J Surg. 2010;199(4):500-506. [ Links ]
9. Karinos N, Hayes PM, Nicol AJ, Kahn D. Avoiding futile damage control laparotomy. Injury. 2010;41(1):64-68. [ Links ]
10. Ferris EJ, Vittimberga FI, Byrne JJ, et al. The inferior vena cava after ligation and placation: a study of collateral routes. Radiology. 1967;89(1):1-10. [ Links ]
 Correspondence:
Correspondence:
Pradeep Navsaria
pradeep.navsaria@uct.ac.za


{kind=link}
{kind=link}