










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.54 no.1 Cape Town Mar. 2016
ORIGINAL ARTICLE
A morphological and immunohistochemical evaluation of gastric carcinoma in the Western Cape province of South Africa
R RobertsI; P GovenderII; R NaidooI; M LocketzI
IDivision of Anatomical Pathology, National Health Laboratory Service and Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa
IIDivision of Anatomical Pathology, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa
ABSTRACT
BACKGROUND: Gastric resections for carcinoma are common, but gastric carcinoma in South Africa, and particularly within the Western Cape province, has not been well documented.
METHOD: The objective of the study was to immunohistochemically evaluate HER2/ neu overexpression, determine aberrations in β-catenin and epithelial-cadherin (E-cadherin) expression, and correlate these findings with gastric carcinoma subtypes.
RESULTS: Ninety-seven gastric adenocarcinoma resections were morphologically categorised as intestinal-, diffuse- or mixed-type adenocarcinomas, and immunohistochemically stained for β-catenin, E-cadherin (extracellular and cytoplasmic domains) and HER2/neu. The results of staining were compared between the subtypes for statistically significant differences. All 97 cases were confirmed as gastric adenocarcinomas, with 39 (40%) intestinal- type, 51 (53%) diffuse-type, and 7 (7%) mixed-type tumours identified. Patient ages ranged from 18-84 years. HER2/neu was overexpressed in 12 (12%) cases, with intestinal-type morphology (p = 0.017) reported in nine. Fourteen cases (14%) demonstrated abnormal β-catenin localisation. Aberrant E-cadherin (extracellular domain) localisation occurred in 36 (37%) cases. Diffuse-type morphology was associated with a significantly high proportion (p = ≤ 0.001). Aberrant E-cadherin (cytoplasmic domain) localisation occurred in 7 (7%) cases. A significantly high proportion (six of these cases) (p = 0.023) of these was diffuse-type morphology. Eleven (11%) adenocarcinomas occurred in patients aged ≤ 40 years, with intestinal morphology reported in nine of these 11. Aberrant E-cadherin (extracellular domain) localisation was noted in seven of the 11, a significantly high proportion when compared to that in the older patients (p = 0.025).
CONCLUSION: Distinct immunomorphological correlations are apparent in tumours demonstrating HER2/neu overexpression or abnormal E-cadherin localisation. Intestinal morphology, poor differentiation and E-cadherin abnormalities are frequently demonstrated in tumours occurring in younger individuals.
Gastric carcinoma resections are common, with gastric adenocarcinoma representing 80-90% of all gastric carcinoma subtypes.1 Distinct differences in the immunohistochemical profile and prognosis are demonstrated in these malignant tumours, dependent, in part, on their morphology, demographic distribution and underlying genetic aberrations. The occurrence of gastric carcinoma in South Africa, and in particular within the Western Cape province, has not been well documented.
The Lauren classification categorises gastric adenocarcinomas into intestinal and diffuse subtypes, based on their histopathological morphology, while tumours with equal proportions of intestinal and diffuse morphology are regarded as a mixed subtype.2
The incidence of gastric carcinoma varies widely. Defined high- and low-risk areas have been identified. High-risk areas include Japan, China, Chile and Portugal. Low-risk areas include the USA and the UK. South Africa is considered to be a low- to intermediate-risk region, with an incidence rate of 12 gastric carcinomas per 100 000 population per year.3
Gastric carcinoma is predominantly a disease of the middle-aged and elderly, with a mean age at presentation of 52 years. There is a strong male predominance, with a 2:1 male to female ratio.4 Gastric carcinomas do not commonly occur in patients aged ≤ 40 years, accounting for less than 5% of cases.5,6 These early-onset cases differ in their sex incidence (with either an equal male to female ratio, or female predominance), morphology (diffuse type, rather than intestinal type) and poor differentiation. Generally, they are associated with a poor prognosis. It was shown in a study by Matley et al.5 that this holds true for cases seen within the Western Cape, South Africa.
The Wnt signalling pathway is a cellular signal transduction system comprising a family of protein ligands which play a critical role in embryogenesis, cell migration, tissue homeostasis and neoplasia. Canonical (β-catenin-dependent) and noncanonical signalling pathways (β-catenin independent) are present, with the β-catenin-dependent pathway most frequently involved in neoplasia and malignancy through its role in the nuclear translocation of β-catenin. Two β-catenin pools are present within human cells. The membrane-bound pool, through its interaction with the epithelial-cadherin (E-cadherin) cell adhesion molecule, aids in cell-cell interaction by binding to the actin cytoskeleton. A second, Wnt-regulated β-catenin pool is present within the cytoplasm.
β-catenin is phosphorylated in the absence of Wnt signalling, resulting in its eventual proteosomal degradation via an E3 ubiquitin ligase process. Glycogen synthase kinase 3β (GSK-3β) and casein kinase 1 α (CK1α) mediate the process of phosphorylation by interaction with the axin and adenomatous polyposis coli (APC) proteins, ultimately forming an APC-axin-GSK-3β-CK1α complex. There is the formation of a WNT-FZD-LRP5/6 trimer with Wnt binding to Frizzled (FZD) via low-density lipoprotein-related receptors 5 and 6 (LRP5/6). Subsequently, FZD binds to Dishevelled, and there is phosphorylation of the cytosolic tail of LRP5/6. The phosphorylated LRP5/6 then binds to axin, and inactivates the APC-axin-GSK-3β-CK1α complex. β-catenin remains unphosphorylated, and accumulates within the cellular cytoplasm. Nuclear translocation of β-catenin then occurs, whereupon it acts as a potent transcription co-regulator through its interaction with the nuclear transcription factors.
E-cadherin is a member of the cadherin superfamily, serving as the main epithelial intercellular adhesion molecule. It consists of extracellular, transmembrane and intracellular domains. The intracellular domain links E-cadherin to the Wnt signalling pathway via its binding of β-catenin. In a normal state, E-cadherin acts as a tumour suppressor gene through the maintenance of cell-cell adhesion and sequestration of β-catenin on the cell membrane. When E-cadherin expression is downregulated, loss of E-cadherin results in the release of β-catenin into the cytoplasm, with the translocation of β-catenin into the nucleus, and the upregulation of epithelial-mesenchymal-related transcription factors. These transcription factors cause a change in phenotype from a cohesive epithelial cell to a motile and discohesive mesenchymal cell which has increased stromal invasive abilities. Loss of E-cadherin expression, which can be demonstrated by immunohistochemical staining, is associated with poor tumour differentiation, increased tumour grade, increased metastasis and poorer prognosis.
Aberrations in β-catenin and E-cadherin are integral to the molecular pathogenesis of gastric adenocarcinoma. A genotype-phenotype correlation is present, with a strong association noted between nuclear β-catenin accumulation and intestinal type adenocarcinomas.7 Additionally, the downregulation of E-cadherin and the loss of immunohistochemical membrane staining is seen in diffuse-type gastric adenocarcinomas.8
HER2/neu is an oncogene on chromosome 17q12-q21. Approximately 20% of gastric adenocarcinomas overexpress HER2/neu. Overexpression of HER2/neu can be assessed by both immunohistochemistry and fluorescence in situ hybridisation (FISH) techniques, with a strong concordance between the two.9 Molecular therapy that targets HER2/neu [anti-HER2/neu monoclonal antibody trastuzumab (Herceptin®)] is currently approved for the treatment of advanced gastric adenocarcinoma and metastatic gastric adenocarcinoma if the carcinoma demonstrates unequivocal evidence of HER2/neu overexpression by immunohistochemistry, or amplification by FISH. HER2/neu testing criteria for the determination of overexpression and amplification were validated in the multinational study of Herceptin® (trastuzumab) in combination with chemotherapy compared with chemotherapy alone in patients with HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA),10 with immunohistochemically determined overexpression equating to a score of 3+. It has been shown in large studies that HER2/neu overexpression was associated with intestinal-type morphology, decreased patient survival and an overall poorer prognosis.9,11
Method
Ethics approval was obtained from the Human Research Ethics Committee, Faculty of Health Sciences, University of Cape Town (Reference Number 504/2009), as part of the broader study proposal titled, Molecular analysis and identification of biomarkers from formalin-fixed, paraffin-embedded gastric cancers, whereafter a retrospective study was undertaken.
Scientific approval of the research proposal for this project was obtained from the research committees of both the Department of Clinical Laboratory Sciences, and the Faculty of Health Sciences, University of Cape Town.
A computerised search of the DISA database of the Division of Anatomical Pathology, University of Cape Town/National Health Laboratory service was performed, searching for gastric carcinoma resections between January 2003 and December 2011. Ninety-seven gastric carcinoma resections were reviewed. All of the cases were confirmed as gastric adenocarcinomas. The tumours were morphologically subclassified into the representative categories of intestinal-, diffuse- or mixed-type adenocarcinomas, and all tumours graded and staged based on the (2009) seventh edition of the Tumor-Node-Metastasis Classification of Malignant Tumours.12
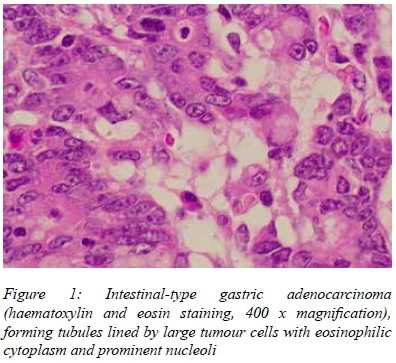
Gastric adenocarcinomas were defined as a primary malignant epithelial neoplasm demonstrating glandular differentiation, either through the formation of neoplastic glands, or by the presence of discrete intracellular mucin. Intestinal-type tumours were characterised by mitotically active epithelial cells with large nuclei, prominent nucleoli and intracytoplasmic mucin. The tumour cells formed glands, nests, sheets and tubules.
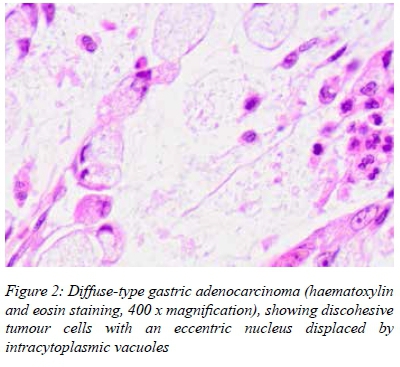
Diffuse-type tumours were characterised by linear cords of poorly cohesive or discohesive epithelial cells, with moderate to severe nuclear hyperchromasia and minimal clear to pale eosinophilic cytoplasm. Signet-ring morphology was often apparent. Gland formation was inconspicuous. Small glands within the superficial regions of the neoplasm were found in occasional tumours.
Equal proportions of intestinal- and diffuse-type morphology were reported in mixed-type tumours. Grade 1 tumours were well differentiated adenocarcinomas, with |≥ 95% of the tumour comprising glands. Grade 2 tumours were moderately differentiated adenocarcinomas, with 50-95% of the tumour comprising glands. Grade 3 tumours were poorly differentiated adenocarcinomas, with 49% or less of the tumour comprising glands. Thus, all diffuse-type tumours were poorly differentiated.
All cases were immunohistochemically stained with antibodies directed against β-catenin, E-cadherin extracellular domain (36B5), E-cadherin cytoplasmic domain (36/E-cadherin) and HER2/neu (Table 1), using standard and well established immunohistochemical staining protocols.
β-catenin staining was scored summatively using the Jass scoring system, with a maximum score of 5. One point was allocated for loss of cell membrane staining; 1 for a slight increase in cytoplasmic staining, 2 for a marked increase in cytoplasmic staining; 1 for slight nuclear staining, and 2 for pronounced nuclear staining. Cases scoring 4 or more were regarded as positive for abnormal β-catenin immunolocalisation.13
Membranous, or a combination of membranous and cytoplasmic staining, represented normal E-cadherin extracellular domain localisation. Cytoplasmic, or a combination of membranous and cytoplasmic staining, represented normal E-cadherin cytoplasmic domain immunohistochemical staining. Any deviation from these staining patterns, including absent staining, was considered to be aberrant cellular localisation.
HER2/neu immunohistochemical staining was scored according to the criteria used in ToGA.10 This scoring system is summarised in Table 2.
Fisher's exact test, the Shapiro-Wilk test, the Bonferroni correction and chi-square test were used in the analysis of variables. Computerised statistical analysis and interpretation was performed using Stata® 12.0 statistical software. The results were considered statistically to be significant when p = ≤ 0.050.
Results
All 97 cases were confirmed as gastric adenocarcinomas, comprising 39 intestinal (Figure 1), 51 diffuse (Figure 2) and seven mixed-type adenocarcinomas (Figure 3). The findings are summarised in Table 3.
The age range for all cases combined was 18-84 years, with a mean age of 57 years. The age range varied from 32 - 84 years for intestinal-type adenocarcinomas, with a mean age of 63 years. An age range of 33-82 years, with a mean age of 55 years, was reported for diffuse-type adenocarcinomas, and 18-57 years, with a mean age of 45 years, for mixed-type gastric adenocarcinomas. Statistically significant differences were noted when comparing age in the intestinal and diffuse gastric adenocarcinoma subtypes (p = 0.007), and between intestinal and mixed subtypes (p = 0.002).
When all cases of gastric carcinoma were compared, more men (53%) than women (47%) were afflicted. Intestinal-type gastric adenocarcinomas were noted in more men (62%) than women (38%), while there was a female predominance in diffuse- and mixed-type tumours, i.e. 57% each. However, statistically significant differences were not reported when the tumour subtypes were compared by gender.
Sixty seven per cent of the intestinal-type tumours were grade 1 or 2 cancer, while 100% of the diffuse-type carcinomas were grade 3. All of the mixed-type tumours were poorly differentiated. A significantly higher proportion of diffuse-type tumours was poorly differentiated, i.e. grade 3 (p = ≤ 0.000), when compared to intestinal-type tumours. Poor differentiation, i.e. grade 3, was demonstrated in a significantly greater proportion of mixed-, compared to intestinal-type tumours.
Lymph nodes were recovered in 94 of the 97 gastrectomy specimens. Regional lymph node metastases were found in all of the tumour subtypes, and detected in 62% of the intestinal-, 61% of the diffuse-, and 85% of the mixed-type tumours. Statistically significant differences were not reported for regional lymph node metastases in the tumour subtypes in the 94 cases where lymph nodes were recovered.
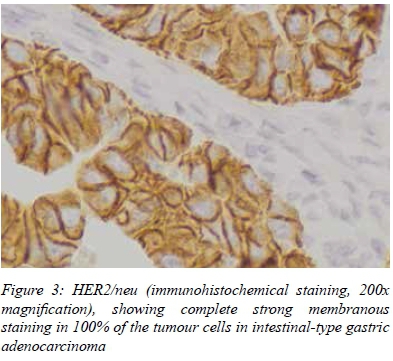
HER2/neu immunohistochemical staining was performed for all 97 cases. Twelve (12) of the 97 cases demonstrated 3+ immunopositivity (Figure 3), and thus were considered to overexpress HER2/neu. These cases comprised nine intestinal-and three diffuse-type tumours. HER2/neu overexpression was shown in a significantly greater proportion (p = 0.017) of the intestinal-type tumours (23%), compared to the diffuse-type tumours (6%).
Abnormal localisation of β-catenin, as detected by immunohistochemistry, was shown in 14 of the 97 gastric adenocarcinoma cases (14%). Abnormal β-catenin immunolocalisation was noted in all three gastric adenocarcinoma subgroups, occurring in 13%, 16% and 14% of the intestinal-, diffuse- and mixed-type tumours, respectively. A statistically significant difference was not evident with respect to β-catenin immunolocalisation in the tumour subgroups.
Aberrant E-cadherin (extracellular domain) localisation occurred in 36 of the 97 cases (37%). Diffuse-type morphology (p = ≤ 0.001) was noted in a significantly higher proportion of the cases. Aberrant E-cadherin (cytoplasmic domain) localisation occurred in seven of the 97 cases (7%) cases. Diffuse-type morphology was demonstrated in six of these cases, a significantly high proportion of these cases (p = 0.023). Therefore diffuse morphology was often associated with E-cadherin derangement.
Mixed-type tumours demonstrating aberrant β-catenin and E-cadherin (extracellular and cytoplasmic domain) immunolocalisation, were reported to have deranged immunostaining in both the intestinal and diffuse tumoural components, mirroring the staining patterns expected for diffuse-, rather than intestinal-type, adenocarcinomas.
There was a statistically significant correlation (p = 0.002) in all of the tumour subtypes with regard to the abnormal immunolocalisation of the E-cadherin cytoplasmic domain and the E-cadherin membranous domain. In addition, a statistically significant (p = 0.023) proportion of the diffuse-type tumours was reported to have abnormal immunolocalisation of both the E-cadherin clones. There was no significant correlation in the intestinal- and mixed-type tumours for immunolocalisation of the two E-cadherin domains.
Eleven cases (11%) of gastric adenocarcinoma were identified in patients aged ≤ 40 years, comprising 9 intestinal-type tumours (82%), 1 diffuse-type tumour (9%) and 1 mixed-type tumour (9%). Six adenocarcinomas (54%) were reported in women and 5 (46%) in men. One tumour (9%) was grade 2 cancer, and 10 tumours (91%) were grade 3. Seven of the eleven cases (64%) demonstrated aberrant E-cadherin (extracellular domain) immunolocalisation. This was significantly greater (p = 0.025) compared to aberrant immunolocalisation in tumours in patients aged ≥ 40 years. Significant differences (p = 0.933) in aberrant E-cadherin (cytoplasmic domain), β-catenin (p = 0.732) or HER2/neu (p = 0.789) immunolocalisation were not found between the two age groups.
Discussion
This study highlights epidemiological and morphological differences in cases of gastric adenocarcinoma occurring within the Western Cape province, compared to those reported in the global literature, with a higher proportion of carcinomas in young adults, with a higher female incidence, and with a higher incidence of tumours in which diffuse-type morphology was demonstrated.
The age range for all cases was 18-84 years, with a mean age of 57 years, similar to findings described in a cohort of 34 cases of gastric carcinoma in a South African study, thus confirming that gastric adenocarcinoma is a disease of the middle-aged and elderly.5 Gastric carcinomas in patients aged ≤ 40 years are uncommon. However, a higher proportion of young gastric adenocarcinoma (11%) was noted in our study cohort, when compared to the 5-6% described in the literature.4 Ninety per cent of the tumours occurring in patients aged ≤ 40 years were grade 3 cancer, confirming the findings described in a previous Western Cape cohort5 and within the broader literature.6
There were more men (53%) than women (47%) in the study cohort, with a male to female ratio of 1.1:1.0. This finding differs markedly from the 2:1 male to female ratio described in the Surveillance, Epidemiology, and End Results database.4
Diffuse-type adenocarcinomas predominantly occur in epidemiologically low-risk regions, and intestinal-type tumours in high-risk areas.14 South Africa is considered a low- to intermediate-risk region for the development of gastric carcinoma.3,15 Diffuse-type morphology was reported for 53% of cases within our study. Corroboratively, 72% of our cases were reported to be grade 3 cancer. Statistically significant differences in immunohistochemically detected HER2/neu overexpression were noted between the tumour subgroups. Overexpression was demonstrated in 12% of the total cases, which included a significant nine of 39 (23%) intestinal-type tumours, compared to only three of 51 cases of diffuse-type tumours in which overexpression was shown. These findings correlate well with previous reports in the literature, confirming the morphological-immunophenotypical association of HER2/neu overexpression and intestinal-type morphology. In addition, the findings are similar to the reported proportion (15-25%) of gastric carcinomas in which HER2/neu is overexpressed.9
Targeted therapy (trastuzumab) is currently approved for the treatment of advanced gastric adenocarcinoma and metastatic gastric adenocarcinoma if the carcinoma demonstrates unequivocal evidence of HER2/neu overexpression by immunohistochemistry, or amplification by FISH. Thus, knowledge of HER2/neu status plays an integral role in patient management through the identification of patients who may benefit from molecular targeted therapy.
The highlights of the study were as follows:
• Gastric adenocarcinoma in the Western Cape is predominantly a disease of the middle-aged and elderly. However, when compared to other populations, a higher proportion of the tumours occurred in younger patients.
• A higher proportion of grade 3 intestinal-type tumours was reported in younger patients with gastric adenocarcinoma, together with deranged E-cadherin immunolocalisation, compared to that in older patients.
• Intestinal-type morphology was often associated with tumours in which HER2/neu was overexpressed.
• Aberrations in E-cadherin immunolocalisation, either involving the E-cadherin extracellular domain alone, or resulting from combined defects in both the cytoplasmic and extracellular domains, were demonstrated in diffuse-type tumours.
• The Wnt signalling pathway is deranged in gastric adenocarcinoma.
Conflict of interest
The authors report that there was no conflict of interest when writing this manuscript.
Declaration
Funding for this study was obtained from the Cancer Association of South Africa, National Health Laboratory Service Research Trust and National Research Foundation.
REFERENCES
1. Kelly JR, Duggan JM. Gastric cancer epidemiology and risk factors. J Clin Epidemiol. 2003;56(1):1-9. [ Links ]
2. Lauren P. The two histologic main types of gastric carcinoma: diffuse and so-called intestinal-type. An attempt at a histo-clinical classification. Acta Pathol Microbiol Scand.1965;64:31-49. [ Links ]
3. Buffart T, Louw M, van Grieken N, et al. Gastric cancers of Western European and African patients show different patterns of genomic instability. BMC Medical Genomics. 2011;4:7. [ Links ]
4. Howlader N, Noone AM, Krapcho M, et al, editors. SEER Cancer Statistics Review, 1975-2010. National Cancer Institute [homepage on the Internet]. 2013. c2016. Available from: http://seer.cancer.gov/archive/csr/1975_2010/ [ Links ]
5. Matley P, Dent D, Madden M, Price S. Gastric carcinoma in young adults. Ann Surg.1988;208(5):593-596. [ Links ]
6. Rugge M, Busatto G, Cassaro M, et al. Patients younger than 40 years with gastric carcinoma. Cancer. 1999;85(12):2506-2511. [ Links ]
7. Ogasawara N, Tsukamoto T, Mizoshita T, et al. Mutations and nuclear accumulation of β-catenin correlate with intestinal phenotypic expression in human gastric cancer. Histopathology. 2006;49(6):612-621. [ Links ]
8. Brooks-Wilson A, Kaurah P, Suriano G, et al. Germline E-cadherin mutations in hereditary diffuse gastric cancer: assessment of 42 new families and review of genetic screening criteria. J Med Genet. 2004;41(7):508-517. [ Links ]
9. Kim M, Jung E, Lee H, et al. Evaluation of HER-2 gene status in gastric carcinoma using immunohistochemistry, fluorescence in situ hybridization and real-time quantitative polymerase chain reaction. Hum Pathol. 2007;38(9):1386-1393. [ Links ]
10. Bang Y, Van Cutsem E, Feyereislova A, et al. Trastuzumab in combination with chemotherapy verses chemotherapy alone for the treatment of Her2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376(9742):687-697. [ Links ]
11. Kim KC, Koh YK, Chang HM, et al. Evaluation of HER2 protein expression in gastric carcinomas: comparative analysis of 1414 cases of whole-tissue sections and 595 cases of tissue microarrays. Ann Surg Oncol. 2011;18(10):2833-2840. [ Links ]
12. Sobin LH, Gospodarowicz MK, Wittekind C, editors. TNM classification of malignant tumors. 7th ed. Weinheim: Wiley; 2009. [ Links ]
13. Jass J, Barker M, Fraser L, et al. APC mutation and tumour budding in colorectal cancer. J Clin Pathol. 2003;56(1):69-73. [ Links ]
14. Steward BW, Kleihues P. World cancer report. Lyon: IARC Press, 2003. [ Links ]
15. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55(2):74-108. [ Links ]
 Correspondence:
Correspondence:
Riyaadh Roberts
riyaadh.roberts@uct.ac.za


{kind=link}
{kind=link}
{kind=link}