










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.53 n.3-4 Cape Town Dec. 2015
GENERAL SURGERY
Acute appendicitis in South Africa: A systematic review
E YangI, II; D KahnII; C CookII
IOregon Health and Science University, Portland, Oregon, USA
IIUniversity of Cape Town, Cape Town, South Africa
ABSTRACT
BACKGROUND: Acute appendicitis is one of the most common surgical emergencies in the West. A large body of research is investigating the risk factors for disease and perforation. As South Africa has a social environment, health system structure, and population demography unique from developed nations, the findings may not be generalisable to this setting. A systematic review has not been performed for appendicitis research in South Africa. The objective of this review was to systematically examine the literature on appendicitis in South Africa.
METHOD: Published articles discussing appendicitis in South Africa up to March 2014 were identified using MEDLINE and EBMReviews. Research themes were analysed in the literature. Perforation rates, mortality, negative appendicectomy rates and gender differences were analysed from audits of patients undergoing appendicectomy for acute appendicitis.
RESULTS: Ten audits were included in the quantitative analysis. Some were excluded in the subgroup analyses. Negative appendicectomies occurred at a rate of 17% (580/3 354). Women were more likely to have a negative appendicectomy than men (28% vs. 9%, p < 0.01). The perforation rate for appendicectomy patients was 36% (970/2 688), and mortality rate was 1% (36/2 946). Research efforts focused on investigating differential incidence and outcomes between racial groups within the country.
CONCLUSION: Appendicitis trends in South Africa are consistent with those in developing regions. However, there is lack of research from the private sector. Further research is needed to investigate specific factors which delay care, outcomes and cost analyses for laparoscopic surgery, and the system strengthening of surgical services at district hospitals.
Appendicitis is one of the most common surgical emergencies in the developed world.1 The appendix becomes inflamed and swollen in its disease course as intestinal bacteria multiply in the lumen, recruiting white blood cells and forming pus. With this accumulation of purulent material, the intraluminal pressure rises, leading to wall ischaemia, necrosis and eventual rupture. Rupture can then either lead to a contained abscess or widespread soiling of the abdominal cavity, which, in turn, causes sepsis and potentially death.2
The aetiology of appendicitis is generally thought to be obstruction of the appendicular lumen, which facilitates intraluminal pressure build-up. However, this is contested, as the obstruction itself does not guarantee disease, and other theories of disease are supported.3 Although its aetiology is still a matter of debate, appendicitis affects both men and women, young and old, and people of all races.3 Despite this widespread potential, its incidence peaks in children and young adults, and is more common in developed regions than in developing regions.4
If left untreated, acute appendicitis naturally progresses to rupture, causing longer hospital stays, higher complication and mortality rates.5 A ruptured appendix carries a heavier disease burden for the patient and constitutes a resource burden on the health system.6
In particular, the rupture rate has been found to be higher in men, the elderly and the very young.7 It has also been found to correlate with health insurance status,8-10 poor utilisation of preventive health services,11 race,12,13 and mental disease.13 Increased perforation risk is essentially attributable to delayed medical care for each of these risk factors.
Antibiotics are advocated as first-line therapy to an extent,14 but the accepted, definitive cure for the disease is surgical removal of the appendix via appendicectomy.15 Considering the time-dependent nature of the disease, timely surgical care is critical in minimising an adverse outcome and disease burden. Thus, considering these dramatic differences in outcomes in ruptured and non-ruptured patients, as well as the time-dependent nature of the disease, ruptured appendicitis has been used as a measure of healthcare access and equity in numerous public health studies.16
However, much of the research in which risk factors for perforation have been investigated has been conducted in the USA and European countries. As South Africa has a political and a social history, a health system structure and population demography which are unique from these other settings, the generalisability of these studies may be somewhat limited to our country. Therefore, a systematic review was conducted on appendicitis research in South Africa, in order to better understand the nature of appendicitis and the risk factors for perforation in this setting.
Objective
The objective of this systematic literature review was to provide an historical and contemporary perspective of appendicitis in South Africa.
Method
Search strategy
MEDLINE and EBM Reviews were searched for published literature on appendicitis and appendicectomy in South Africa. The reference lists of identified studies were searched further to identify relevant studies. Articles published in Afrikaans were translated into English for review. The following specific search terms were used for all searches:
- "Appendicitis AND South Africa"
- "Appendectomy AND South Africa"
- "Appendicectomy AND South Africa".
Selection criteria
All peer-reviewed, published, original research studies in which appendicitis was addressed in South Africa were eligible for inclusion in this review. Inclusion criteria and the methodology to define appendicitis were used to determine inclusion in the analysis for the appendicitis and appendicectomy audits. Recurring themes and observations were compiled and assessed by the researchers. Racial categories were included to highlight research in differential determinants of disease and outcomes.
Results
Appendicitis in South Africa
The first audit for appendicitis in South Africa was published in 1939, drawing on hospital records throughout the country, in an effort to assess the nature of the disease and its impact on different racial groups.17 Erasmus formed two major conclusions when contrasting the disease between ethnic groups, namely, that there was a significantly higher incidence rates of appendicitis in white patients than that in black patients, but with significantly less morbidity and mortality.17 These two observations formed the groundwork and direction for the further study of appendicitis in South Africa over the next 70 years.
Differential incidence: dietary hypothesis and fibre intake
Hospital records from three Johannesburg hospitals were reviewed in Erasmus' study, from 1929-1937. Appendicitis and overall admissions were recorded according to racial groups. Using these figures, 4% of white inpatients were admitted for appendicitis, compared to 1% of coloureds and 0% of black inpatients.17 Although these figures do not represent the true incidence rates in the general population, as hospital access and utilisation patterns are likely to have differed between three racial groups, the important possibility of differential incidences between racial groups was raised. These trends were supported by findings from audits in Cape Town and Upington.18,19
A leading theory in which these differences are explained is that a Westernised diet, with declining dietary fibre content, increases the risk of appendicitis developing.20 Consistent with this reasoning, Erasmus noted that appendicitis was more common in black South Africans on a "European" diet than in those on a "native" diet,17 suggesting that environmental factors influenced the pathology of appendicitis, in addition to genetic proclivities for disease. This association has been supported through further ecological studies in which the epidemiology of these diseases was evaluated in comparison to dietary habits in both developed and developing countries around the world.21
Burkitt et al.21 studied the dietary fibre content and stool transit times in people in the UK, Uganda and South Africa, and found a negative correlation between fibre content and transit times, irrespective of ethnicity. Looking specifically at the South African subjects in this study, white students eating a refined diet, black students on a mixed diet, and black students on an unrefined diet - this correlation still holds true. Longer stool transit times were recorded as the fibre content decreased. High bowel disease rates were not recorded in any community with a high-fibre diet in their study, supporting the appendicitis incidence findings previously mentioned. Dietary fibre consumption negatively correlated with appendicectomy frequency for the South African students, in particular.22
If, then, dietary habits dictate the risk of appendicitis, it would follow that there would be a rise in incidence in urbanised communities with increasingly Westernised food consumption. Mixed results were seen in South Africa from 1950-1978 as appendicitis rates increased in urban black patients near Durban.23 However, changes were not noted in semi-rural black patients near Bloemfontein.24 Furthermore, appendicitis rates in urban black patients near Johannesburg from 1979-1983 were found to be roughly the same as those reported by Erasmus in 1937.25 However, incidence estimates in South Africa increased from 8.2 cases per 100 000 population in 1986 (25) to 15 per 100 000 over 20 years later.5,26
If the dietary hypothesis is further explored, several studies have investigated the potential causal role of faecaliths, with the thought that greater faecal residue associated with a low-fibre diet leads to obstructive faecaliths, which, in turn, causes appendicitis. Black South Africans with appendicitis were more likely to have appendicular faecaliths than those with a normal appendice, and as a whole had fewer faecaliths than a comparison group of Canadian patients.27 These findings were contested at the time,28 but gathered support years later.29
Differential outcomes
The second main observation from Erasmus' study is that of differential outcomes and mortality rates between black and white South Africans with appendicitis. Blacks not only had higher rates of rupture and complicated appendicitis, their mortality was three times that of whites, i.e. 30% vs. 10%.17 These figures echoed previous research performed in the USA, in which appendicitis outcomes between African-Americans and Caucasian-Americans in New Orleans were compared.30 While Erasmus suggested that a biological mechanism may have contributed to these worse outcomes in blacks, the difference in outcome seemed to relate more to health-seeking behaviour which affected how promptly medical care was received.
Delayed presentation is a recurring theme when discussing the high perforation rates in South Africa. It was found in several studies that perforated patients generally delayed seeking care longer than those with non-perforated appendicitis5,29,31 and that South Africans, as a whole, presented later than patients in developed countries, leading to higher perforation rates.26 In trying to understand the reasons underlying this phenomenon, the authors cited socioeconomic disadvantage,26 health system weaknesses,5 poor access to care,29 the use of traditional healers32 and poor education.33 Only one study contested the association between delayed presentation and perforation, as the delay was similar in both patient groups.34 Kong et al. identified rural origin as an independent risk factor for perforation in their audit in Pietermaritzburg.35
Even if patients present to health facilities in a timely fashion, misdiagnoses can delay surgical treatment. As acute appendicitis is mostly a clinical diagnosis, the question of whether or not disease presentation varies between races has been contested over the years. Some have argued that black patients generally have atypical disease presentations which diverge from "classical" appendicitis, thus leading to delayed diagnoses and care.5,34 Others have argued the opposite, that black African patients with appendicitis present similarly to white European patients, but that barriers in communication and language lead to perceived differences in symptomatology.29,36
Appendicitis audits
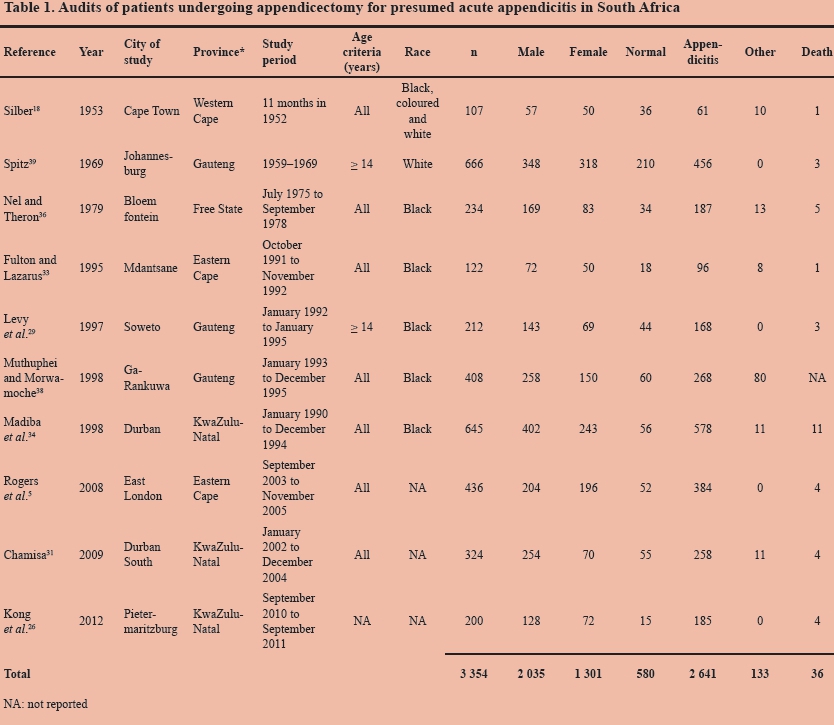
Ten studies were included for analysis, based on inclusion criteria. The studies included patients undergoing operation for presumed acute appendicitis, and excluded those undergoing incidental appendicectomy, patients with appendicitis who were treated conservatively without an operation, and patients with chronic appendicitis. Appendicitis was defined histologically in all the studies, except for those by Rogers et al.5 and Kong et al.,26 in which diagnoses were made by operative findings.
The diagnosis of chronic appendicitis, a diagnosis which often led to negative appendicectomies and persistent symptoms after operation, was discussed in the older studies in this review.18 As a separate and distinct preoperative entity than acute appendicitis, chronic appendicitis patients were also excluded from analysis.
Studies with different inclusion criteria were excluded from the analysis. Moore and Schneider37 and Segal et al.25 studied patients with histologically proven appendicitis, thus excluding those with presumed appendicitis who had histologically normal appendixes. Movsowitz19 audited appendicectomy cases in Upington, but was unclear in his inclusion criteria, and included an unusually high number of normal specimens, prompting exclusion from this analysis.
The findings from these studies are summarised in Table 1. Of the patients undergoing appendicectomy for presumed acute appendicitis in South Africa, 79% were found to have appendicitis. This figure includes those with perforated appendicitis. Negative appendicectomies constituted 17% of the total operations, and the appendixes were found to be diseased with some other pathology in 4% of the operations. After excluding Muthuphei and Morwamoche,38 who did not report deaths in their study, the overall mortality rate for appendicectomy patients was calculated to be 1% (36/2 946).
Appendicitis with perforation
Nine audits were included for analysis, based on the mentioned criteria mentioned. Spitz39 was excluded, as detailed a breakdown of acute versus perforated patients was not recorded in his article. From the included studies, shown in Table 2, the perforation rate for patients undergoing appendicectomy for acute appendicitis in South Africa was 36%. The negative appendicectomy rate was 14%.
Moore and Schneider37 conducted an audit on histologically proven appendicitis in paediatric patients near Cape Town. Of the 436 proven appendicitis cases which he reviewed, 203 (47%) were perforated, a figure consistent with the findings from the included studies when normal and non-appendicitis cases were removed from analysis.
Mortality
Of the audits included for analysis in analysing appendicitis rates, nine were analysed for mortality. Muthuphei and Morwamoche38 were excluded as deaths were not reported. A summary of appendicular pathology for those patients who died is provided in Table 3. Of the 36 recorded deaths, 90% were noted to have appendicitis, with perforation and/ or generalised peritonitis (32/36). Of the remaining four patients, one was acutely inflamed, but with distant abscesses, one had a normal appendix, and there was no mention of surgical findings for the other two. To compare the mortality rate according to appendixes that were perforated and those that were not, Spitz39 was also excluded as overall breakdown by pathology was not specified in his study. From the remaining eight studies, there were a total 33 deaths from 2 280 appendicectomies. Of those with perforations, 3% died, compared to 0% of those who were not perforated (p < 0.010, Fisher's exact test).
Time to presentation
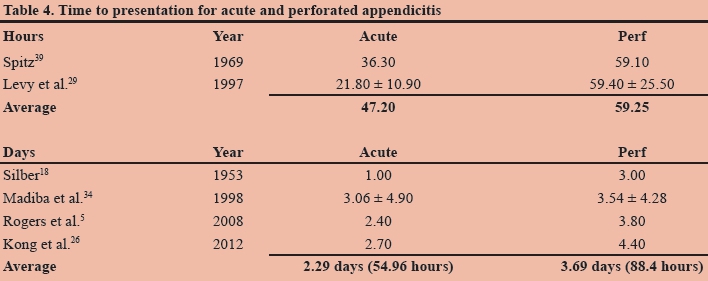
Of the appendicectomy audits, six published details on the time to presentation for patients with proven perforations, compared to those with inflamed appendixes. Two studies reported the time in hours, whereas the other four reported the time in days (Table 4). Regardless of the time unit used for measurement, those with perforated appendicitis consistently experienced symptoms for longer before receiving medical care, than those with non-ruptured, inflamed appendixes.
Gender variation
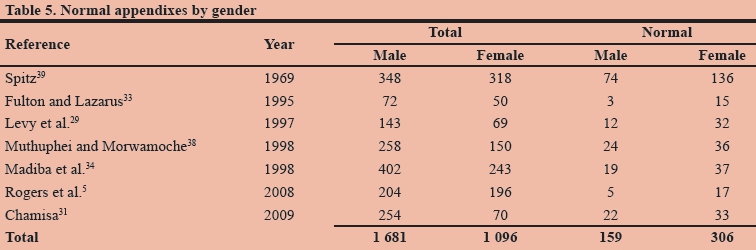
Patients undergoing appendicectomy for suspected acute appendicitis were more likely to be male than female (Table 5). However, from the seven studies which reported a gender breakdown on appendixes which were found to be normal, women were found to have a much higher negative appendicectomy rate. Twenty-eight per cent of women undergoing appendicectomy were found to have a normal appendix, compared to 9% of men (Χ2 = 162.2, p < 0.010).
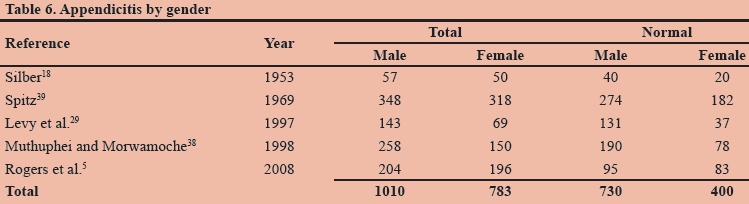
Five studies provided gender breakdowns for those who were confirmed to have appendicitis, whether it was inflamed or perforated (Table 6). Men undergoing appendicectomy for acute appendicitis were more likely than women to have appendicitis (72% vs. 51%, Χ2 = 85.0, p < 0.010). This higher rate of misdiagnosis in women was noted by several authors, who emphasised the need to consider and exclude other pathology in women because of to the potential of other mimicking conditions.18,29,39
Four studies provided a gender breakdown for those who were found to have perforated appendicitis.5,29,31,38 Men had a perforation rate of 26% (227/859), and women a perforation rate of 21% (103/485). Men who underwent appendicectomy for acute appendicitis were more likely to have perforated than women (26% vs. 21%, Χ2 = 4.5, p 0.034), which is reflected in the literature.7
Health systems and quality metrics
Recent studies have explored the role of the health system in providing adequate surgical care to South Africans, particularly in rural settings. As greater awareness has risen regarding inequality in surgical care, the Department of Health guidelines for which surgical services should be offered at district level can be found in the district hospital service package (DHSP).40
However, rural district hospitals have been found to perform very few appendicectomies, laparotomies and other general surgery procedures listed in the DHSP.41 This was partially owing to the fact that the underlying pathology of an acute abdomen is often diagnosed intraoperatively, with some conditions treatable at district hospitals, and others requiring transfer to a higher level of care. Because of this uncertainty, medical officers have often opted to transfer patients to regional hospitals, rather than potentially embark on cases which are considered too difficult to manage at district hospital level.
A surgical outreach programme was initiated by the Department of Health n Kwazulu-Natal in an effort to deliver surgical care and training to district hospitals. Clarke et al. found that "there remains a significant gap between the range of surgeries the World Health Organization believes should be performed in a district hospital and what is actually delivered", in their review of 12 years of activity in rural KwaZulu-Natal.42
Discussion
Following Erasmus' audit in 1939,17 appendicitis research in South Africa has addressed issues of differences in incidence, perforation and morbidity associated with the disease. The appendicitis incidence rate in white South Africans was comparable to that in developed countries, whereas the incidence in black South Africans was significantly lower. However, perforation rates were high in South Africa, and associated with a delay in seeking medical care. Nearly all deaths recorded in appendicectomy patients were attributable to perforation and generalised peritonitis.
Women undergoing appendicectomy were more likely to have a negative operation than men, but men were more likely to have more serious disease. This has been shown in previous studies,7 with an underlying explanation of differences in health-seeking behaviour, whereas no differences by gender have been reported in other large-scale studies.43,44
Generally speaking, the appendicitis trends observed in South Africa were consistent with those found in comparable settings. The perforation rate of 36% was consistent with, or higher than, the rate in studies performed in other African countries.45-48 Overall, the incidence rate was much lower than that in developed countries, with slight increases as urbanisation increased.
However, despite the number of studies which have been performed over the last century, several notable gaps in the literature remain.
The body of literature on appendicitis in South Africa is skewed towards black populations utilising public health services. Studies on white patients and those in the private sector are visibly lacking. White South Africans have largely been assumed to behave similarly to white populations in developed countries, an oversimplification which fails to address cultural, environmental and social factors which are unique to this country. Research efforts focused on the public sector do not capture the population which chooses to utilise private health services, a group which conceivably doesn't face the same socio-economic constraints as public sector patients, thereby leading to delayed presentation and subsequent perforation. This omission may contribute to the demonstrably poor outcomes which have characterised South African audits to date, but the degree of this potential effect is unknown.
Perhaps related to this skew is the unusually long time to presentation noted in South African patients. As shown in the reviewed studies, South Africans presented to the hospital notably later than patients in developed settings. Numerous reasons and influences have been suggested by the investigators of the audits, but more comprehensive research on influential factors behind the delay is lacking. Studies explore attitudes toward hospitals and deterrents to South Africans seeking medical care in general,49 but the reasons for delaying to seek medical care need to be more fully explored with respect to surgical patients specifically.
The surgical approach for appendicitis has been mentioned in several studies, in which a very small proportion utilised a laparoscopic approach.26 The understanding is that the vast majority of appendicectomies performed in South Africa are via open incision, rather than the laparoscopic approach. Surgeons have increasingly recognised the importance of laparoscopic surgery, but generally, public hospitals are not uniformly able to routinely offer them.50 The advanced spectrum of disease in rural South Africans may also influence surgeons to favour an open approach over laparoscopy.
The prohibitive cost of laparoscopic equipment is a significant reason for this. However, laparoscopic appendicectomy has been shown in some settings to provide equally safe and effective surgical treatment as open surgery, but at a comparable economic cost.51 When considering the costs of either approach, post-surgical hospital care and productivity losses need to be taken into consideration in order to gain a full understanding of economic costs. Thus, research comparing the laparoscopic and the open approach in South Africa is needed, including measurements of outcome, length of hospital stay and effects on productivity.
Given that many medical officers at district hospitals may not feel comfortable performing laparotomies and appendicectomies, the care of rural patients seeking medical care at these hospitals may be delayed, and they may unduly suffer as a consequence. Further research is needed to understand how surgical services at the district hospital can be strengthened, thus offloading patient volume from the regional centres and shortening delays to surgery for surgical patients. In addition to improving health outcomes for these patients, the cost burden on the health system would be expected to decrease as well if patients received earlier treatment.52
The findings in this review, together with some notable gaps in the literature, emphasise the need for further research in which appendicitis in the private sector is investigated, and understanding gained as to why delays in care occur, for the prevalence and outcomes of laparoscopic surgery to be estimated, and on how to strengthen surgical services at the district hospital.
REFERENCES
1. Saidi HS, Adwok JA. Acute appendicitis: an overview. East Afr Med J. 2000;77(3):152-156. [ Links ]
2. Berry J Jr, Malt RA. Appendicitis near its centenary. Ann Surg. 1984;200(5):567-575. [ Links ]
3. Carr NJ. The pathology of acute appendicitis. Ann Diagn Pathol. 2000;4(1):46-58. [ Links ]
4. Walker AR, Segal I. Appendicitis: an African perspective. JR Soc Med. 1995;88(11):616-619. [ Links ]
5. Rogers AD, Hampton MI, Bunting M, Atherstone AK. Audit of appendicectomies at Frere Hospital, Eastern Cape. S Afr J Surg. 2008;46(3):74-77. [ Links ]
6. Gadomski A, Jenkins P. Ruptured appendicitis among children as an indicator of access to care. Health Serv Res. 2001;36(1 Pt 1):129-142. [ Links ]
7. Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990;132(5):910-925. [ Links ]
8. Braveman P, Schaaf VM, Egerter S, et al. Insurance-related differences in the risk of ruptured appendix. N Eng J Med. 1994;331(7):444-449. [ Links ]
9. Herrod HG, Chang CF. Potentially avoidable pediatric hospitalizations as defined by the Agency for Healthcare Research and Quality: what do they tell us about disparities in child health? Clin Pediatr (Phila). 2008;47(2):128-136. [ Links ]
10. Pieracci FM, Eachempati SR, Barie PS, Callahan MA. Insurance status, but not race, predicts perforation in adult patients with acute appendicitis. J Am Coll Surg. 2007;205(3):445-452. [ Links ]
11. Smink DS, Fishman SJ, Kleinman K, Finkelstein JA. Effects of race, insurance status, and hospital volume on perforated appendicitis in children. Pediatrics. 2005;115(4):920-925. [ Links ]
12. Guagliardo MF, Teach SJ, Huang ZJ, et al. Racial and ethnic disparities in pediatric appendicitis rupture rate. Acad Emerg Med. 2003;10(11):1218-1227. [ Links ]
13. Tsay JH, Lee CH, Hsu YJ, et al. Disparities in appendicitis rupture rate among mentally ill patients. BMC Public Health. 2007;7:331. [ Links ]
14. Hansson J, Korner U, Ludwigs K, et al. Antibiotics as first-line therapy for acute appendicitis: evidence for a change in clinical practice. World J Surg. 2012;36(9):2028-2036. [ Links ]
15. Wilms IM, de Hoog DE, de Visser DC, Janzing HM. Appendectomy versus antibiotic treatment for acute appendicitis. [Cochrane review]. In: The Cochrane Library, Issue 11, 2011. Oxford: Update Software. [ Links ]
16. Lee SL, Yaghoubian A, Stark R, Shekherdimian S. Equal access to healthcare does not eliminate disparities in the management of adults with appendicitis. J Surg Res. 2011;170(2):209-213. [ Links ]
17. Erasmus JPF. The incidence of appendicitis in the Bantu. S Afr Med J. 1939;13:601-607. [ Links ]
18. Silber W. Appendicectomy: a survey of 200 cases. S Afr Med J. 1953;27(9):187-190. [ Links ]
19. Movsowitz L. Some observations on appendicitis in general practice in Upington. S Afr Med J. 1967;41(33):823-826. [ Links ]
20. Mayo CH. THe appendix in relation to, or as the cause of, other abdominal diseases. J Am Med Assoc. 1924;83(8):592-593. [ Links ]
21. Burkitt DP, Walker AR, Painter NS. Effect of dietary fibre on stools and the transit-times, and its role in the causation of disease. Lancet. 1972;2(7792):1408-1412. [ Links ]
22. Walker AR, Walker BF. Appendectomy in South African inter-ethnic school pupils. Am J Gastroenterol. 1987;82(3):219-222. [ Links ]
23. Moore SW, Robbs JV. Acute appendicitis in the Zulu: an emerging disease? S Afr Med J. 1979;55(18):700. [ Links ]
24. Griffiths ML. A comparison of admissions to a semirural hospital between the years 1959/1960 and 1977/1978. S Afr Med J. 1981;59(27):983-96. [ Links ]
25. Segal I, Paterson A, Walker AR. Characteristics and occurrence of appendicitis in the black population in Johannesburg, South Africa. J Clin Gastroenterol. 1986;8(5):530-533. [ Links ]
26. Kong VY, Bulajic B, Allorto NL, et al. Acute appendicitis in a developing country. World J Surg. 2012;36(9):2068-2073. [ Links ]
27. Jones BA, Demetriades D, Segal I, Burkitt DP. The prevalence of appendiceal fecaliths in patients with and without appendicitis. A comparative study from Canada and South Africa. Ann Surg. 1985;202(1):80-82. [ Links ]
28. Brink CF, Prinsloo H, van der Poel JS. The seasonal incidence of acute appendicitis. S Afr Med J. 1985;68(3):156-158. [ Links ]
29. Levy RD, Degiannis E, Kantarovsky A, et al. Audit of acute appendicitis in a black South African population. S Afr J Surg. 1997;35(4):198-202. [ Links ]
30. Boyce FF, McFetridge EM. The essential clinical considerations of acute appendicitis. Internat S Digest. 1936;22:195-213. [ Links ]
31. Chamisa I. A clinicopathological review of 324 appendices removed for acute appendicitis in Durban, South Africa: a retrospective analysis. Ann R Coll Surg Engl. 2009;91(8):688-692. [ Links ]
32. Walker AR, Walker BF, Manetsi B, et al. Appendicitis in Soweto, South Africa: traditional healers and hospitalization. JR Soc Health. 1989;109(6):190-2. [ Links ]
33. Fulton J, Lazarus C. Acute appendicitis among black South Africans. S Afr J Surg. 1995;33(4):165-166. [ Links ]
34. Madiba TE, Haffejee AA, Mbete DL, et al. Appendicitis among African patients at King Edward VIII Hospital, Durban, South Africa: a review. East Afr Med J. 1998;75(2):81-84. [ Links ]
35. Kong VY, van der Linde S, Aldous C, et al. Quantifying the disparity in outcome between urban and rural patients with acute appendicitis in South Africa. S Afr Med J. 2013;103(10):742-745. [ Links ]
36. Nel CJ, Theron EJ. Appendicitis in the Black population. S Afr Med J. 1979;55(23):939-941. [ Links ]
37. Moore SW, Schneider J. Acute appendicitis in childhood: experience in a developing country. Pediatr Surg Int. 1995;10(2-3):71-75. [ Links ]
38. Muthuphei MN, Morwamoche P. The surgical pathology of the appendix in South African blacks. Cent Afr J Med. 1998;44(1):9-11. [ Links ]
39. Spitz L. Acute appendicitis. An analysis of six hundred and sixty-six appendicectomies in adults 1959-1968. S Afr J Surg. 1969;7(3):129-137. [ Links ]
40. The primary healthcare package for South Africa: a set of norms and standards. Part 3: Norms and standards for district hospitals. Pretoria: Department of Health, 2002. [ Links ]
41. Voss M, Duvenage R. Operative surgery at the district hospital. S Afr Med J. 2011;101(8):521-522. [ Links ]
42. Clarke DL, Aldous C. Surgical outreach in rural South Africa: are we managing to impart surgical skills? S Afr Med J. 2013;104(1):57-60. [ Links ]
43. Charfi S, Sellami A, Affes A, et al. Histopathological findings in appendectomy specimens: a study of 24,697 cases. Int J Colorectal Dis. 2014;29(8):1009-1012. [ Links ]
44. Marudanayagam R, Williams GT, Rees BI. Review of the pathological results of 2660 appendicectomy specimens. J Gastroenterol. 2006;41(8):745-749. [ Links ]
45. Ayoade BA, Olawoye OA, Salami BA, Banjo AA. Acute appendicitis in Olabisi Onabanjo University Teaching Hospital, Sagamu: a three year review. Nigerian Journal of Clinical Practice. 2006;9(1):52-56. [ Links ]
46. Ali N, Aliyu S. Appendicitis and its surgical management experience at the University of Maiduguri Teaching Hospital Nigeria. Nigerian Journal of Medicine. 2012;21(2):223-226. [ Links ]
47. Ohene-Yeboah M, Togbe B. An audit of appendicitis and appendicectomy in Kumasi, Ghana. West Afr J Med. 2006;25(2):138-143. [ Links ]
48. Willmore WS, Hill AG. Acute appendicitis in a Kenyan rural hospital. East Afr Med J. 2001;78(7):355-357. [ Links ]
49. Harris B, Goudge J, Ataguba JE, et al. Inequities in access to health care in South Africa. J Public Health Policy. 2011;32 Suppl 1:S102-S123. [ Links ]
50. Apostolou C, Panieri E. National survey of surgeons' attitudes to laparoscopic surgical training in South Africa. S Afr J Surg. 2007;45(3):86. [ Links ]
51. Minutolo V, Licciardello A, Di Stefano B, et al. Outcomes and cost analysis of laparoscopic versus open appendectomy for treatment of acute appendicitis: 4-years experience in a district hospital. BMC Surg. 2014;14:14. [ Links ]
52. Kong V, Aldous C, Handley J, Clarke D. The cost effectiveness of early management of acute appendicitis underlies the importance of curative surgical services to a primary healthcare programme. Ann R Coll Surg Engl. 2013;95(4):280-284. [ Links ]
 Correspondence:
Correspondence:
Estin Yang
appystudy@gmail.com


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}