










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.53 no.2 Cape Town Jul. 2015
http://dx.doi.org/10.7196/SAJSNEW.7851
CASE REPORT
Hypoxic brain injury and cortical blindness in a victim of a Mozambican spitting cobra bite
A ChackoI; S AndronikouII; V RamanjamIII
IMB BCh, FC Rad (SA); Department of Radiology, Steve Biko Academic Hospital, University of Pretoria, South Africa
IIMB BCh, FC Rad (SA), FRCR, PhD; Department of Radiology, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIMB ChB, DCH (SA), FCPaed (SA), Cert Neurodev (SA); Department of Paediatrics and Neuro-Development, 2 Military Hospital and Red Cross War Memorial Children's Hospital, Cape Town, South Africa
ABSTRACT
Snakebite and the subsequent envenomation is a serious and potentially fatal illness, owing to the effects of the various toxins present in the venom. Cortical blindness following bites containing neurotoxin is a rare complication. We describe the clinical findings and imaging in a child who sustained significant brain injury following a bite from a Mozambican spitting cobra. We also discuss the venom composition, complications and appropriate management of such cases.
Case report
A 6-month-old male infant was bitten on the right ankle while asleep in late February 2012. The snake was caught, killed and later identified as a Mozambican spitting cobra (Naja mossambica mossambica). The child was immediately taken to the local primary healthcare clinic from where the patient and family were referred to the nearest secondary hospital, Richards Bay Hospital in KwaZulu-Natal, South Africa. The transfer to the hospital involved a journey of several hours.
En route the patient was noted as having severe breathing difficulty and had a reported respiratory arrest upon arrival in Richards Bay. Resuscitation was performed and the patient was admitted to the intensive care unit where he remained for the next 3 weeks. Generalised tonic-clonic convulsions were reported during this time. Polyvalent anti-snake venom (ASV) was administered to the patient more than 24 hours after the snakebite incident owing to delay in procuring the ASV from Johannesburg.
The site of the bite proceeded to become necrotic and required debridement and later skin grafting.
The patient was discharged from the Richards Bay Hospital 1 month after the incident in a stable condition but with significant neurological sequelae. The patient was then referred at the age of 10 months to 2 Military Hospital in Cape Town for ongoing management from a neurodevelopmental perspective, assessment of right lower limb contractures following the skin grafting and for assessment of post-intubation stridor.
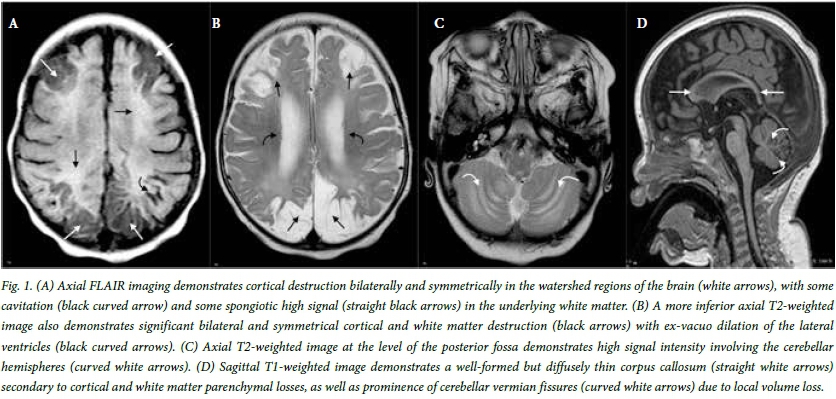
Clinically, the patient had microcephaly, cortical visual impairment and mild global developmental delay, but with no long tract signs. Magnetic resonance imaging (MRI) (Fig. 1) performed in Cape Town 4 months after the incident demonstrated global hypoxic ischaemic damage with grey and white matter cystic changes and a thinned corpus callosum.
The patient is currently stable under management of the paediatric neurologists.
Discussion
Naja mossambica, also known as the Mozambican spitting cobra, is found in sub-Saharan Africa, mainly in Angola, Botswana, Malawi, Mozambique, Namibia, South Africa, Swaziland, Tanzania, Zambia and Zimbabwe.
In early reports, a relatively large percentage (94%) of patients (from KwaZulu-Natal, South Africa) were bitten inside human dwellings and of these approximately 80% occurred while the victims were asleep, as in our case.[1]
Snake venoms contain proteins, lipids, steroids, amines, aminopolysaccharides, quinines, neurotransmitters and other compounds that are capable of causing many effects.
The Mozambican spitting cobra, an elapid, has both cytotoxic and neurotoxic components in its venom. Extensive experience in the treatment of bites, specifically by the Mozambique spitting cobra, has been described in KwaZulu-Natal, where it has been shown that the predominant effect of the venom is cytotoxic with only minimal neurotoxic effects.[1]
A more recent report in 2010 (although much smaller in the number of cases described) also recorded predominantly cytotoxic effects of envenomation and relatively little neurological effects from this venom.[2] This makes the findings in our patient somewhat unique in that it represents the first case reported where cortical blindness (representative of a hypoxic injury to the brain) resulted from a Mozambican spitting cobra bite. The history in our case is highly indicative of a neurotoxic effect with respiratory arrest.
Neurotoxic envenomation has the potential to cause a broad spectrum of early presentations varying from ptosis and ophthalmoplegia to respiratory arrest, which can present as acute medical emergencies. Generally patients show good response if treatment is given in good time.
The other end of the spectrum is formed by delayed neurotoxic manifestations, which include peripheral neuropathies, occasionally optic neuritis and cortical blindness.[3] Cerebellar involvement and ataxia as well as the 'locked-in syndrome' are very uncommon manifestations of neurotoxic snakebite. Common neurological symptoms in decreasing order of frequency include ptosis (85.7%), ophthalmoplegia (75%), limb weakness (26.8%), respiratory failure (17.9%), palatal weakness (10.7%) and neck muscle weakness (7.1%).[4] These are experienced usually within 6 hours of the bite.[4]
Following administration of antivenom, the signs of recovery become evident within a few hours to several days.[3] Our patient received antivenom only 24 hours after the snakebite, which may explain the enhanced neurotoxic effects. He developed most of the neurological symptoms described above at various stages of the admission in intensive care unit.
Cortical blindness is the total or partial loss of vision in a normal-appearing eye caused by damage to the visual area in the brain's occipital cortex.[3] Cerebral vascular hypoperfusion is the most common cause of cortical blindness and MRI with or without contrast is an important diagnostic test in cortical blindness.
The major causes of cortical blindness in general are: asphyxia, hypoxia or ischaemia, all of which may occur during the birth process, developmental brain defects, head injury, hydrocephalus and infections of the central nervous system, such as meningitis and encephalitis.
The least common cause of hypoxia is snakebite.[3] The latter condition can lead to respiratory failure by the neurotoxic venom or to cardiac arrest following an anaphylactic reaction after injecting ASV.
Imaging findings in cortical blindness following snakebite are similar to those of other causes of hypoxic brain injury.[5] These can be divided into early and late findings. The best diagnostic clue is that of periventricular leukomalacia. The initial early clue on MRI is restriction on diffusion weighted imaging, while the late findings are periventricular volume loss, associated ventriculomegaly and gliosis in the affected areas. Cavitation, thalamic scarring and demyelination are also sometimes seen in late imaging.[5] Our patient showed features of a global insult occurring some time previously as the scan was only performed after 4 months from the date of the incident.
In case series from KwaZulu-Natal, the South African Institute of Medical Research polyvalent antivenom was administered where possible and the evidence suggests that the effectiveness of the antivenom is indirectly proportional to the time that has elapsed between the bite and the administration of the antivenom.[4] This same finding has been borne out in other similar case series and studies.[2,3] Appropriate management of the acute snakebite includes appropriate first-aid and prompt seeking of medical attention.
In the hospital setting, the management includes supportive measures as well as anti-snake venom administration, whether monovalent (species specific) or polyvalent (broad spectrum). Administration of a high initial bolus followed by repeated doses every 6 hours until there are signs of neurological recovery have been recommended by some authors.[6] The ASV should be administered together with neostigmine and atropine and supported by appropriate ventilation as required. In the study, the findings supported the above management and resulted in early recovery, reduced total dose of ASV, reduced duration of mechanical ventilation and reduced the incidence of complications.[6] In the rural setting, such therapy appears not to be available at the clinic level or even at regional hospital level. This is a failure of the health system considering that snakebites are more commonly encountered in the rural environment.
Conclusion
Evaluation of victims of neurotoxic snake bite for early signs of respiratory depression and prompt respiratory assistance, even if antivenom is not available, is essential as a life-saving measure and to prevent serious neurological sequelae. The catastrophic consequences of persistent neurological deficits, including cortical blindness, may thereby be minimised in victims who survive. MRI is a mechanism of demonstrating the devastating effects of delayed treatment in snakebites with neurotoxic venom, including that of the Mozambican spitting cobra.
REFERENCES
1. Tilbury CR. Observations on the bite of the Mozambique spitting cobra (Naja mossambica mossambica). S Afr Med J 1982;61(9):308-313. [ Links ]
2. Vermaak SS, Visser A, Le Roux TLB. A deadly bed partner: M'Fesi (Mozambique spitting cobra). SA Orthop J 2010;9(4):58-62. [ Links ]
3. Seneviratne U, Dissanayake S. Neurological manifestations of snakebite in Sri Lanka. J Postgrad Med 2002;48(4):275-278. [ Links ]
4. JRScience. Mechanisms of venom toxicity. http://jrscience.wcp.muohio.edu/studentresearch/costarica03/venom/mechanisms.htm (accessed 7 August 2012). [ Links ]
5. Osborn AG, Salzman KL, Katzman G, et al. Diagnostic Imaging: Brain. Salt Lake City: Amirsys, 2004:68-87. [ Links ]
6. Agrawal A, Gupta A, Khanna A. What dose of anti-snake venom should be given in severe neuroparalytic snakebite? Ann Thorac Med 2011;6(1):47-48. [http://dx.doi.org/10.4103/1817-1737.74281] [ Links ]
 Correspondence:
Correspondence:
A Chacko
anithchacko@gmail.com


{kind=link}