










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Surgery
versión On-line ISSN 2078-5151
versión impresa ISSN 0038-2361
S. Afr. j. surg. vol.53 no.2 Cape Town jul. 2015
http://dx.doi.org/10.7196/SAJSNEW.7864
GENERAL SURGERY
Quilting after mastectomy significantly reduces seroma formation
G S MannuI, II; K QurihiIII; F CareyIV; M A AhmadV; M HussienVI
IMSc MRCSE; Breast Surgery Unit, Norfolk and Norwich University Hospital, Norfolk, UK
IIMSc MRCSE; General Surgery, Oxford University Hospital, Oxford, UK
IIIFRCS; Breast Surgery Unit, Norfolk and Norwich University Hospital, Norfolk, UK
IVMBBS BSc; Breast Surgery Unit, Norfolk and Norwich University Hospital, Norfolk, UK
VFRCS; Breast Surgery Unit, Norfolk and Norwich University Hospital, Norfolk, UK
VIMS MD FRCS; Breast Surgery Unit, Norfolk and Norwich University Hospital, Norfolk, UK
ABSTRACT
INTRODUCTION: Seroma formation is one of the most frequently encountered complications following mastectomy. It may cause significant morbidity, including delayed wound healing, infection and frequent clinic attendance for seroma aspiration.
OBJECTIVE: To evaluate the effect of surgical quilting after mastectomy in the prevention of postoperative seroma and to investigate which factors influence seroma formation.
METHODS: This was a single-centre prospective cohort study over a 1-year period. All patients who had a mastectomy operation during this period were included in this study. Group 1 patients (quilting) had mastectomy flaps sutured to pectoral muscle using interrupted absorbable sutures. Seroma requiring aspiration, number of aspirations and volume aspirated were recorded postoperatively.
RESULTS: During the study period, 168 patients were recruited, with 54 patients in group 1 (quilting) and 114 patients in group 2 (non-quilting). The proportion of patients who developed seroma requiring aspiration was 69% (n=79) in the non-quilting group and 29% (n=15) in the quilting group (p<0.001). Additionally, the total volume of seroma drained was 427 mL (standard error (SE)=69) in the non-quilting group and 63 mL (SE=21) in the quilting group (p=0.0008). The total number of seroma aspirations was 152 in the non-quilting group compared with 23 in the quilting group (p=0.0001). Seroma was more common in smokers (p=0.003) and was not decreased by the presence of drains.
CONCLUSION: Quilting of the mastectomy flaps significantly reduces seroma formation. Both total volume of seroma aspirated and number of aspirations are significantly reduced using this technique. We would therefore recommend quilting of mastectomy flaps to reduce the incidence of postoperative seromas and morbidity.
Breast cancer remains one of the leading causes of cancer deaths among women.[1] Simple mastectomy is a common surgical procedure that is used in the management of breast cancer. Seroma is one of the most frequently encountered complications following mastectomy and is a serous fluid that accumulates in the space between the skin flap and underlying tissues. It may cause significant morbidity, including delayed wound healing, and can result in frequent outpatient attendance for seroma aspiration. Repeat aspirations may in turn increase the risk of wound infection and impact on adjuvant treatment, thus compounding patient anxiety during an already difficult time. The incidence of seroma formation after mastectomy has been reported in the literature to vary from 15 to 81%.[2-5]
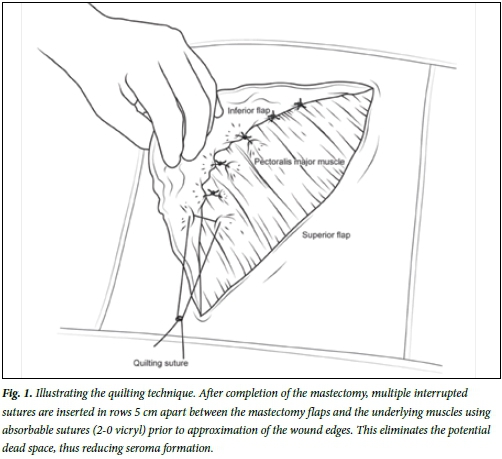
A number of techniques have been employed in an attempt to reduce or prevent seroma formation among mastectomy patients using both mechanical and chemical approaches. However, there is significant heterogeneity in their benefits and there is a paucity of uniform evidence for their use. Quilting is a simple surgical procedure that eliminates the anatomical dead space remaining after mastectomy (Fig. 1). It involves placing interrupted absorbable sutures between the mastectomy flap and pectoral muscle prior to wound closure. It has been described in several studies assessing the technique at donor sites of autologous breast reconstruction.[6-9] However, it has not yet been prospectively investigated in a large patient population in the context of addressing seroma formation following mastectomy. The objective of this prospective study is to evaluate the effect of surgical quilting after mastectomy in the prevention of postoperative seroma and to investigate which factors influence seroma formation.
Methods
This is a single-centre, prospective cohort study carried out from January 2012 to January 2013.
Participants and setting
Norfolk and Norwich University Hospital is a tertiary referral centre and our unit operates on 600 new breast cancer patients per year, including 200 from the UK national breast cancer screening programme. All patients who had a mastectomy with or without axillary surgery during this period were included in this study. Patients who had a skin-sparing mastectomy with immediate breast reconstruction were excluded. Data were collected on the day of surgery and at an outpatient follow-up clinic 2 weeks postoperatively.
Intervention
All patients received a single dose of cefuroxime 750 mg intravenously at the time of induction of anaesthesia. Surgery was carried out by four consultant breast surgeons. All patients in the cohort underwent simple mastectomy with preservation of pectoralis major muscle and the pectoralis fascia. Mastectomy flaps were dissected using electro-diathermy and the lymph node procedure (whether sentinel node biopsy or axillary clearance) was performed as planned. Only one surgeon performed the quilting procedure routinely, using a uniform technique in all simple mastectomies, while the remaining three did not. In the quilting group (group 1), after completion of the mastectomy and axillary procedure, multiple interrupted sutures were inserted in rows 5 cm apart between the mastectomy flaps and the underlying muscles using absorbable sutures (2-0 vicryl) prior to approximation of the wound edges using continuous 3-0 subcuticular monocryl sutures (Fig. 1). No patients in the quilting group had a drain inserted.
In the non-quilting control group (group 2), simple mastectomy was performed by three independent surgeons without quilting, and the skin edges were approximated with continuous 3-0 subcuticular monocryl. The use of drains was left to the discretion of the operating surgeon, but in order to investigate the effect of drains on seroma formation in this group, all surgeons were required to record their use of drains. Although the breast and axillary surgeries were conducted by different surgeons between the two arms of the study, it was by a standardised approach across the department determined by the unit's policy which has been previously published.[10, 11]
Information collected and outcomes
Data were collected on the day of surgery and on the subsequent follow-up appointments prospectively. The data collected included patient's age, body mass index (BMI), side of procedure, smoking status, nature of axillary surgery, use of drains, antiplatelet or anticoagulant medication and use of neo-adjuvant therapy. The primary dichotomous outcome measure was seroma formation requiring aspiration. Secondary outcomes were the number of aspirations performed and the volume of seroma drained (in millilitres) in each group.
All patients were informed that seroma is very common and may not need to be aspirated. Indications for seroma aspiration were discomfort, infection or wound leak. Patients were encouraged to contact a designated seroma clinic if they had any concerns prior to their planned appointments. All patients were reviewed in an outpatient clinic 2 weeks postoperatively and further outpatient appointments were arranged if needed. It was during these outpatient clinics that information on seroma formation and numbers of aspirations performed were recorded.
Adjuvant therapy
The final decision regarding the nature of adjuvant treatment was made after discussion in a multidisciplinary team meeting. The indications for post-mastectomy radiotherapy were positive excision margins or positive axillary lymph nodes. Chemotherapy was offered to high-risk patients with respect to the National Institute of Clinical Excellence (NICE) guidelines.[12] Endocrine therapy was accessible to patients with hormone receptor-positive carcinoma.
Statistical methods
Statistical analysis was performed by a medical statistician using NCSS version 07.1.7 software (NCSS, USA).[13] The two groups were compared. Associations between variables in both groups were assessed using X2-squared and i-test.
Results
Recruitment
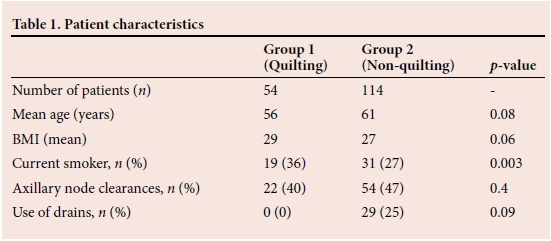
During the study period, 168 patients were recruited from January 2012 to January 2013. There were 54 patients in group 1 (quilting) and 114 patients in group 2 (non-quilting). There were no losses to follow-up and all patients had primary and secondary outcomes recorded.
Baseline characteristics
The baseline characteristics are shown in Table 1. Mean age (standard deviation (SD)) in the quilting and non-quilting groups were 56 (13.8) years and 61 (13.2) years respectively (p=0.08). Patient BMI (SD) in each group was 29 (5.0) and 27 (5.8) respectively (p=0.06). There were 19 smokers (36%) in group 1 compared with 31 (27%) in group 2 (p=0.003). Axillary clearance was performed in similar proportions in both groups (Table 1).
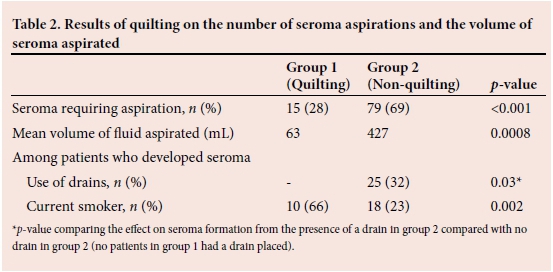
In group 2 (n = 114), 29 patients had drains, of whom 25 (86.2%) patients developed seroma. Of the 85 patients who did not have drains, 54 patients developed a seroma (63.5%). When assessing the cumulative effect of using drains in those who developed a seroma with those who did not in group 2, there was no statistically significant difference in seroma rates with the use of drains (p=0.09). No patients in group 1 had a drain inserted.
Assessment of primary and secondary outcomes across groups
The proportion of patients who developed seroma requiring aspiration was 29% (n = 15) in group 1 and 69% (n=79) in group 2 (p<0.001). Additionally, 23 patients (29%) had >3 aspirations of seroma in group 2 compared with 2 (13%) patients in group 1 (p=0.0001). The total volume of seroma drained in group 1 was 63 mL (standard error (SE) 21) compared with 427 mL (SE 69) in group2 (p=0.0008). There was no statistically significant difference on seroma formation by the addition of axillary clearance procedure to simple mastectomy between the two groups (p=0.4). Group 1 had statistically less seroma formation, reduced volumes of seroma and required fewer aspirations of the seroma.
Sub-analysis of seroma population
The impact of using quilting sutures on the occurrence of seroma was assessed in more detail in relation to three potential risk factors, namely age, BMI and smoking habit. A logistic regression analysis was conducted to determine the effects, if any, of these factors on the occurrence of seroma. Within the group 2, 46 (40.4%) patients had a BMI <25, 40 (35.1%) patients had a BMI between 25 and 29.9, and 28 (24.6%) patients had a BMI >30. There were proportionally more overweight patients in group 1, where 14 (25.9%) patients had a BMI <25, 18 (33.3%) patients had a BMI between 25 and 29.9, and 22 (40.7%) patients had a BMI >30. The mean (SD) BMI in group 1 was 29 (5.8) and in group 2 was 27 (4.9). There was no statistical significance between BMI and seroma formation across both groups (p=0.06). The mean (SD) age in group 2 was 61 (13.2) and in group 1 was 56 (14.7), and age was also not significantly associated with seroma formation across both groups (p=0.08).
Within group 1, smoking was significantly related to seroma formation (p=0.003). Of the patients in this group who developed a seroma, 33.3% (n=5) had never smoked and 66.7% (n=10) were current smokers (p=0.002). The statistical significance of smoking on seroma formation was not apparent in group 2, where 77.3% (n=61) had never smoked and 22.7% (n=18) were current smokers (p=0.1). The quilting method was successful among patients who had never smoked. However, this benefit in reducing seroma formation appeared to be negated by smoking.
Discussion
This study is one of the largest studies to prospectively assess quilting in reducing seroma formation following simple mastectomy in patients in the UK. Seroma formation is a very common occurrence after breast surgery and some authors have even called it a side-effect of surgery rather than a complication.[14] Traditionally, drains have been used to reduce seroma formation after breast surgery. Many different types of drain, such as low-pressure suction, high-pressure suction, closed tube, corrugated drains and multiple numbers of drains have been used in an attempt to find the best technique to prevent seroma formation. However, studies have shown that the presence or absence of suction drains does not make any significant difference to seroma formation,[4,15] nor is any one type of drain superior to another in preventing seromas.[16,17] Furthermore, our results actually show an increase in seroma formation after the use of drains. In group 2, 86% of patients who had wound drains developed a seroma compared with 63.5% who did not have drains (p=0.04). It is possible that the physical irritation of the plastic suction drain among the cauterised tissue contributes to the pro-inflammatory response, resulting in increased seroma formation.
Furthermore, prior to this study, no association between smoking and seroma formation has been described.[14] In our study, we have shown that smoking was significantly related to seroma formation in group 1 where twice as many patients were smokers than non-smokers (p=0.003). The effect of smoking appeared to negate the benefits of quilting on seroma formation.
The reason for this is unclear. However, it may be owing to the detrimental impact of smoking on the healing process.[18] Smoking may be a risk factor for seroma formation in group 2. However, our cohort did not show statistical significance to test that hypothesis (p=0.1).
Pathophysiology of seroma formation
The exact underlying mechanism of seroma formation remains unclear. Certain risk factors such as high BMI, large breast size, smoking, malignant axillary nodes and use of tamoxifen and heparin have been reported to increase seroma formation.[19] Furthermore, a number of theories have been put forward to explain its aetiology. Watt-Boolsen et al.[20]suggested that surgical trauma gives rise to an acute inflammatory reaction that results in the formation of an exudate that constitutes seroma fluid. However, others have suggested that seroma probably originates from lymphatic fluid.[21]
There is a body of evidence to suggest that electrocautery dissection may increase the incidence of seroma due to thermal trauma.[22] Unfortunately, electrocautery is essential for adequate haemostasis intraoperatively. Electrocautery has been increasingly used in all surgical disciplines to reduce operating time and minimise blood loss. It has been shown that using diathermy significantly increases the rate of seroma formation.[23] The reason for this may be the activation of proinflammatory cytokines as a result of tissue injury resulting in an increased incidence of seroma formation. Evidence for this theory comes from comparison of electrocautery and an ultrasonic dissector that appears to produce smaller volumes of pro-inflammatory cytokines and also has a reduced incidence of seroma formation.[24]
Chemical approaches for reducing seroma formation
There have been a variety of approaches aimed at reducing seroma formation described in the literature to date. However, these have had varying degrees of success. Although the exact aetiology of seroma formation remains uncertain,[22] it is generally thought to be the result of the postoperative inflammatory response. Glucocorticoids inhibit the inflammatory process and there has been interest in whether this could be used to reduce seroma formation. Unfortunately, randomised studies assessing the drainage volume of seroma formation following an injection of a bolus of 125 mg of methylprednisolone sodium succinate before mastectomy have not shown any significant difference.[25]
Fibrin glue and sclerosing agents have been used in an attempt to reduce postoperative seromas with varying degrees of success. Some small-scale studies have demonstrated reduction in post-mastectomy seroma formation with the use of tetracycline sclerotherapy[26] or 95% ethyl alcohol or povidone iodine.[27] However, when tetracycline-based sclerotherapy was assessed in a larger, randomised, controlled trial format, there was a lack of demonstrable benefit in those treated and the study was terminated prematurely due to severe pain when the tetracycline was introduced into the drains.[28]
Another study suggested that the timing of postoperative shoulder physiotherapy may play a factor in reducing seroma formation. It has shown that seroma formation is decreased when shoulder physiotherapy is delayed for 1 week without resulting in any detrimental outcome on long-term shoulder function (p<0.05)[29] However, this was demonstrated in an unblinded setting, following more extensive surgery (modified radical mastectomy) and with a limited numbers of patients.[29]
Surgical approaches to reducing seroma formation
It is clear that chemical approaches to reducing seroma formation have had only mixed success. Thus, various surgical techniques have been used to try to help prevent seroma formation. Halstead[30] first described a technique in 1913, which involved suturing the short superior flap following mastectomy with silk to the fascia below the first rib and with the remaining part of the defect being skin grafted. Other methods such as using tension sutures or through-and-through sutures between skin flaps and chest wall, have been used historically to obliterate the dead space in an attempt to decrease seroma formation.[31] A prospective, randomised, controlled trial in 1993 successfully showed that fixation of the skin flaps using multiple tacking sutures to close the dead space reduced seroma formation in patients who underwent mastectomy. However, that study only had 39 patients and all of them had axillary clearance and drain insertion.[32] In contrast, our study analysed a larger number and none of the patients in the quilting group (group1) had a drain inserted.
There has been growing evidence for the use of quilting for seroma prevention in recent years.[33-35] A recent study has shown quilting to reduce postoperative hospital stay and provide a possible financial saving of £240 per patient.[34] A recent Chinese randomised controlled trial of 201 patients noted volume, duration and drainage rates of post operative seroma in the quilting group was reduced in the first 72 hours (p<0.01) following surgery with reduced seroma formation (p<0.01)[36]. Our current study is the largest in the UK to demonstrate the benefit of quilting.
The limitations of our study included the non-randomised, unblinded nature of patient recruitment. This is an inherent difficulty with surgical studies of this nature. However, patients were equally matched by baseline characteristics and demographics between the study arms. The operating surgeon(s) only performed the procedure stipulated in their allocated arm in order to limit observer or intervention bias between the two arms. Although we accept that there is the possibility that other confounding factors may affect the outcomes of a single surgeon performing the quilting procedure, it is clear that the next step is a UK-based randomised controlled trial to further investigate this approach.
Conclusion
Quilting of the mastectomy flaps significantly reduces seroma formation, total volume of seroma aspirated and number of aspirations. Seroma formation is more common in patients who smoke. The use of surgical drains during mastectomy does not reduce seroma formation. We would therefore recommend quilting of mastectomy flaps to reduce the incidence of postoperative seromas and hence reduce morbidity.
REFERENCES
1. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer statistics, 2008. CA Cancer J Clin 2008;58(2):71-96. [http://dx.doi.org/10.3322/CA.2007.0010] [ Links ]
2. Woodworth PA, McBoyle MF, Helmer SD, Beamer RL. Seroma formation after breast cancer surgery: Incidence and predicting factors. Am Surg 2000;66(5):444-450. [ Links ]
3. Roses DF, Brooks AD, Harris MN, Shapiro RL, Mitnick J. Complications of level I and II axillary dissection in the treatment of carcinoma of the breast. Ann Surg 1999;230(2):194-201. [ Links ]
4. Abe M, Iwase T, Takeuchi T, Murai H, Miura S. A randomized controlled trial on the prevention of seroma after partial or total mastectomy and axillary lymph node dissection. Breast Cancer 1998;30;5(1):67-69. [ Links ],
5. Say CC, Donegan W. A biostatistical evaluation of complications from mastectomy. Surg Gynecol Obstet 1974;138(3):370-376. [ Links ]
6. Thekkinkattil DK, Hussain T, Mahapatra TK, McManus PL, Kneeshaw PJ. Feasibility of use of a barbed suture (v-loc 180) for quilting the donor site in latissimus dorsi myocutaneous flap breast reconstruction. Arch Plast Surg 2013;40(2):117-122. [http://dx.doi.org/10.5999/aps.2013.40.2.117] [ Links ]
7. Rossetto LA, Garcia EB, Abla LE, Ferreira LM. Seroma and quilting suture at the donor site of the TRAM flap in breast reconstruction: A prospective randomized double-blind clinical trial. Ann Plast Surg 2013;72(4):391-397. [http://dx.doi.org/10.1097/SAP.0b013e3182610b11] [ Links ]
8. Sajid MS, Betal D, Akhter N, Rapisarda IF, Bonomi R. Prevention of postoperative seroma-related morbidity by quilting of latissimus dorsi flap donor site: A systematic review. Clin Breast Cancer 2011;11(6):357-363. [http://dx.doi.org/10.1016/j.clbc.2011.04.006] [ Links ]
9. Mannu GS, Farooq N, Down S, Burger A, Hussien MI. Avoiding back wound dehiscence in extended latissimus dorsi flap reconstruction. ANZ J Surg 2013;83(5):359-364. [http://dx.doi.org/10.1111/j.1445-2197.2012.06292.x] [ Links ]
10. Mannu GS, Navi A, Hussien M. Sentinel lymph node biopsy before mastectomy and immediate breast reconstruction does not significantly delay surgery in early breast cancer. ANZ J Surg 2015;85(6):438-443. [http://dx.doi.org/10.1111/ans.12603] [ Links ]
11. Mannu GS, Navi A, Morgan A, et al. Sentinel lymph node biopsy before mastectomy and immediate breast reconstruction may predict post-mastectomy radiotherapy, reduce delayed complications and improve the choice of reconstruction. Int J Surg 2012;10(5):259-264. [http://dx.doi.org/10.1016/j.ijsu.2012.04.010] [ Links ]
12. National Institute of Clinical Excellence. CG80: Early and locally advanced breast cancer: Diagnosis and treatment. National Institute of Clinical Excellence. http://guidance.nice.org.uk/cg80 (accessed 29 August 2013). [ Links ]
13. Hintze J. NCSS. In: NCSS, editor. 07.1.7 ed. Utah: USA; NCSS, 2008. [ Links ]
14. Srivastava V, Basu S, Shukla VK. Seroma formation after breast cancer surgery: What we have learned in the last two decades. J Breast Cancer 2012;15(4):373-380. [http://dx.doi.org/10.4048/jbc.2012.15.4.373] [ Links ]
15. Kuroi K, Shimozuma K, Taguchi T, et al. Evidence-based risk factors for seroma formation in breast surgery. Jpn J Clin Oncol 2006;36(4):197-206. [http://dx.doi.org/10.1093/jjco/hyl019] [ Links ]
16. Bonnema J, van Geel AN, Ligtenstein DA, Schmitz PI, Wiggers T. A prospective randomized trial of high versus low vacuum drainage after axillary dissection for breast cancer. Am J Surg 1997;173(2):76-79. [http://dx.doi.org/10.1016/S0002-9610(96)00416-3] [ Links ]
17. Taylor JC, Rai S, Hoar F, Brown H, Vishwanath L. Breast cancer surgery without suction drainage: The impact of adopting a 'no drains' policy on symptomatic seroma formation rates. Eur J Surg Oncol 2013;39(4):334-338. [http://dx.doi.org/10.1016/j.ejso.2012.12.022] [ Links ]
18. Sorensen LT. Wound healing and infection in surgery. The clinical impact of smoking and smoking cessation: A systematic review and meta-analysis. Arch Surg 2012;147(4):373-383. [http://dx.doi.org/10.1001/archsurg.2012.5] [ Links ]
19. Miller ME, Czechura T, Martz B, et al. Operative risks associated with contralateral prophylactic mastectomy: A single institution experience. Ann Surg Oncol 2013;20(13):4113-4120. [http://dx.doi.org/10.1245/s10434-013-3108-1] [ Links ]
20. Watt-Boolsen S, Nielsen VB, Jensen J, Bak S. Postmastectomy seroma. A study of the nature and origin of seroma after mastectomy. Dan Med Bull 1989;36(5):487-489. [ Links ]
21. Bonnema J, Ligtenstein DA, Wiggers T, van Geel AN. The composition of serous fluid after axillary dissection. Eur J Surg 1999;165(1):9-13. [http://dx.doi.org/10.1080/110241599750007441] [ Links ]
22. Agrawal A, Ayantunde AA, Cheung KL. Concepts of seroma formation and prevention in breast cancer surgery. ANZ J Surg 2006;76(12):1088-1095. [http://dx.doi.org/10.1111/j.1445-2197.2006.03949.x] [ Links ]
23. Porter KA, O'Connor S, Rimm E, Lopez M. Electrocautery as a factor in seroma formation following mastectomy. Am J Surg 1998;176(1):8-11. [ Links ]
24. Yilmaz KB, Dogan L, Nalbant H, et al. Comparing scalpel, electrocautery and ultrasonic dissector effects: The impact on wound complications and pro inflammatory cytokine levels in wound fluid from mastectomy patients. J Breast Cancer 2011;14(1):58-63. [http://dx.doi.org/10.4048/jbc.2011.14.1.58] [ Links ]
25. Okholm M, Axelsson CK. No effect of steroids on seroma formation after mastectomy. Dan Med Bull 2011;58(2):A4241. [ Links ]
26. Emad H, Sherif F, Soliman EK. Tetracycline sclerotherapy in treating postmastectomy seroma: A simple solution for a frequently occurring problem. Egypt J Surg 1999;28(3):99-104. [ Links ]
27. Throckmorton AD, Askegard-Giesmann J, Hoskin TL, et al. Sclerotherapy for the treatment of postmastectomy seroma. Am J Surg 2008;196(4):541-544. [http://dx.doi.org/10.1016/j.amjsurg.2008.06.020] [ Links ]
28. McCarthy PM, Martin JK Jr., Wells DC, Welch JS, Ilstrup DM. An aborted, prospective, randomized trial of sclerotherapy for prolonged drainage after mastectomy. Surg Gynecol Obstet 1986;162(5):418-420. [ Links ]
29. Schultz I, Barholm M, Grondal S. Delayed shoulder exercises in reducing seroma frequency after modified radical mastectomy: A prospective randomized study. Ann Surg Oncol 1997;4(4):293-297. [ Links ]
30. Halsted WS. Developments in skin grafting operation for cancer of the breast. JAMA 1913;60(6):416-418. [http://dx.doi.org/10.1001/jama.1913.04340060008004] [ Links ]
31. Orr TG Jr. An incision and method of wound closure for radical mastectomy. Ann Surg 1951;133(4):565-566. [ Links ]
32. Coveney EC, O'Dwyer PJ, Geraghty JG, O'Higgins NJ. Effect of closing dead space on seroma formation after mastectomy--a prospective randomized clinical trial. Eur J Surg Oncol 1993;19(2):143-146. [ Links ]
33. Sakkary MA. The value of mastectomy flap fixation in reducing fluid drainage and seroma formation in breast cancer patients. World J Surg Oncol 2012;10:8. [http://dx.doi.org/10.1186/1477-7819-10-8] [ Links ]
34. Almond LM, Khodaverdi L, Kumar B, Coveney EC. Flap anchoring following primary breast cancer surgery facilitates early hospital discharge and reduces costs. Breast Care (Basel) 2010;5(2):97-101. [http://dx.doi.org/10.1159/000301586] [ Links ]
35. Yu J, Forouhi P. Quilting of flaps substantially reduces seroma formation following mastectomy (MX) or axillary clearance (ANCL). Eur J Surg Oncol 2012;38(5):454. [ Links ]
36. Gong Y, Xu J, Shao J, et al. Prevention of seroma formation after mastectomy and axillary dissection by lymph vessel ligation and dead space closure: A randomized trial. Am J Surg 2010;200(3):352-356. [http://dx.doi.org/10.1016/j.amjsurg.2009.10.013] [ Links ]
 Correspondence:
Correspondence:
G S Mannu
gurdeepmannu@gmail.com

