










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.53 n.1 Cape Town Mar. 2015
http://dx.doi.org/10.7196/SAJS.1888
CASE REPORT
Selective angioembolisation for splenic salvage following blunt abdominal trauma
G L LaingI; J L BruceII; J IslamIII; D L ClarkeIV
IMB ChB, FCS (SA), Cert Trauma Surgery (SA); Pietermaritzburg Metropolitan Trauma Service, Pietermaritzburg, South Africa
IIMB ChB, FCS (SA); Pietermaritzburg Metropolitan Trauma Service, Pietermaritzburg, South Africa
IIIMB ChB, MMedSci, FCS (SA), Cert Vascular Surgery (SA); Pietermaritzburg Metropolitan Trauma Service, Pietermaritzburg, South Africa
IVMB ChB, FCS (SA), MBA, MMedSci, MPhil; Pietermaritzburg Metropolitan Trauma Service, Pietermaritzburg, South Africa
ABSTRACT
Isolated high-grade splenic injury following blunt abdominal trauma is an uncommon finding. The selected use of catheter-directed angiography and angioembolisation for splenic salvage has been successful in haemodynamically stable patients.
Case report
A 20-year-old man was referred with a delayed presentation of blunt abdominal trauma (BAT). He had sustained a focal blow to the left upper quadrant (LUQ) with a wooden rod (knobkierrie) 5 days earlier. On examination, the pulse rate was 100 beats per minute (bpm) and the blood pressure was 130/86 mmHg. Abdominal palpation elicited focal LUQ tenderness and fullness. A full blood count confirmed a reduced serum haemoglobin concentration of 9.5 g/dL.
In view of the clinical findings and suspicion of a splenic injury, a double-contrast computed tomography (CT) scan of the abdomen was performed. This investigation confirmed an American Association for the Surgery of Trauma (AAST) grade IV splenic injury, with contrast extravasation consistent with a splenic pseudoaneurysm (Fig. 1).

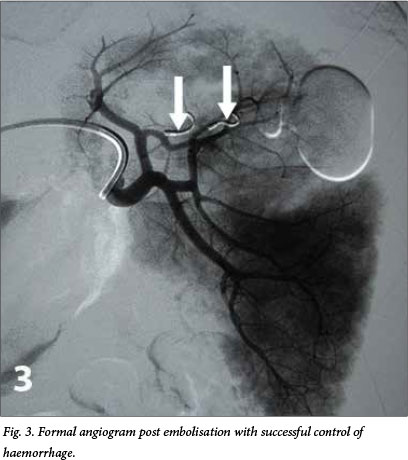
We proceeded to perform catheter-directed angiography of the splenic artery, which confirmed the diagnosis of splenic artery pseudoaneurysm of a segmental branch of the upper splenic pole (Fig. 2). The relevant segmental artery was selected and embolised with two coils. A postembolisation angiogram confirmed successful control of the haemorrhage (Fig. 3).

The patient suffered no complications following the procedure and was discharged after 48 hours of clinical observation.
Discussion
Splenic injury most commonly occurs as a result of BAT due to motor vehicle collisions. Less commonly it may present following BAT sustained in an assault.
Following the pioneering work of paediatric surgeons, the traditional management of splenic injuries has shifted from operative exploration and splenectomy to selective non-operative management (SNOM).[1] Progressive development in the quality and accessibility of accurate imaging modalities and interventional technology has extended the window of opportunity for splenic salvage.
The management options for splenic injury include SNOM, angiographic embolisation and surgical exploration. Management selection is dependent on haemodynamic status, the grade of injury and the presence or absence of associated injuries. Availability of the requisite skills and resources also influences the management approach ultimately selected.
A haemodynamically unstable patient with a positive focused assessment by sonography for trauma (FAST) scan or diagnostic peritoneal lavage requires emergency abdominal exploration to determine the source of intraperitoneal haemorrhage.[2,3]
Haemodynamically stable patients are considered for evaluation by means of a contrasted abdominal CT scan. Patients with lesser-grade splenic injuries (AAST I, II and III) without evidence of associated intra-abdominal injuries or active contrast extravasation are candidates for a trial of SNOM.
CT scan findings of contrast extravasation indicate that intervention is necessary, as these patients have a high rate of failed SNOM and are at risk of fatal haemorrhage.[4] This subset of BAT patients has derived maximum benefit from interventional angioembolisation, which has a reported success rate of 96%.[5] In view of the fact that the perfusion of the splenic sinusoids is determined by the arterial pressure, it is not yet known whether a therapeutically induced thrombosis will alter normal long-term splenic and immunological function.[6]
Surgery is indicated in patients who cannot be adequately observed owing to limited resources or other injuries, and those in whom non-surgical management fails. Technical options at surgical exploration are dictated by patient physiological factors and grade of splenic injury. These include splenectomy or splenic salvage by means of partial splenic resection and haemostatic manoeuvres (suture, mesh encapsulation).
The case reported here is a testament to the selective use of angioembolisation for splenic salvage in a haemodynamically stable patient with an isolated high-grade splenic injury.
REFERENCES
1. Upadhyaya P. Conservative management of splenic trauma: History and current trends. Pediatr Surg Int 2003;19(9-10):617-627. [http://dx.doi.org/10.1007/s00383-003-0972-y] [ Links ]
2. Lo A, Matheson AM, Adams D. Impact of concomitant trauma in the management of blunt splenic injuries. N Z Med J 2004;117(1201):U1052. [ Links ]
3. Wahl WL, Ahrns KS, Chen S, Hemmila MR, Rowe SA, Arbabi S. Blunt splenic injury: Operation versus angiographic embolization. Surgery 2004;136(4):891-899. [http://dx.doi.org/10.1016/j.surg.2004.06.026] [ Links ]
4. Schurr MJ, Fabian TC, Gavant M, et al. Management of blunt splenic trauma: Computed tomographic contrast blush predicts failure of nonoperative management. J Trauma 1995;39(3):507-513. [http://dx.doi.org/10.1097/00005373-199509000-00018] [ Links ]
5. Bhullar IS, Frykberg ER, Sigarusa D, et al. Selective angiographic embolization of blunt splenic traumatic injuries in adults decreases failure rate of nonoperative management. J Trauma Acute Care Surg 2012;72(5):1127-1143. [http://dx.doi.org/10.1097/TA.0b013e3182569849] [ Links ]
6. Richardson JD. Changes in the management of injuries to the liver and spleen. J Am Coll Surg 2005;200(5):648-669. [http://dx.doi.org/10.1016/j.jamcollsurg.2004.11.005] [ Links ]
 Correspondence:
Correspondence:
G L Laing
grantlaing@me.com

