










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.53 n.1 Cape Town Mar. 2015
http://dx.doi.org/10.7196/SAJS.2458
CASE REPORT
Aorto-internal iliac artery endovascular reconstruction for critical limb ischaemia: A case report
J PillaiI; T MonarengII; T B RangakaIII; C YaziciogluIV; R JayakrishnanV; M G VellerVI
IBSc, MB BCh, FCS, CVS; Division of Vascular Surgery, Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIBDS, MB BCh, FCS; Division of Vascular Surgery, Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIMB BCh, MMed; Division of Vascular Surgery, Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IVBSc, BHSc (Hons); Division of Vascular Surgery, Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VMB BCh, FCS; Division of Vascular Surgery, Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VIMB BCh, FCS, MMed; Division of Vascular Surgery, Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
The internal iliac artery and cruciate anastomosis are important collateral vessels in severe aortoiliac occlusive disease. This report describes a patient with left leg rest pain due to occlusion of the left common and external iliac arteries. In addition, there was a high-grade stenosis of the right common iliac artery. Direct catheter canulation of the left internal iliac artery revealed that it was patent. Endovascular stent placement was successful in re-establishing blood flow into the left internal iliac artery. Ischaemic rest pain was relieved and the ankle brachial index was maintained at 0.85 at 6 months follow-up.
Trans-Atlantic Inter-Society Consensus (TASC) D lesions of the aortoiliac arteries are known to cause lower limb ischaemia.[1] The viability of the affected lower limb is maintained by an important collateral network between the internal iliac and profunda arteries. This is commonly referred to as the cruciate anastomosis, which is a collateralisation between the inferior gluteal (internal iliac), medial circumflex femoral, lateral circumflex femoral and the first perforating branch (profunda femorus).
In this case report, we present a case of critical lower limb ischaemia treated by endovascular revascularisation of the internal iliac artery.
Case report
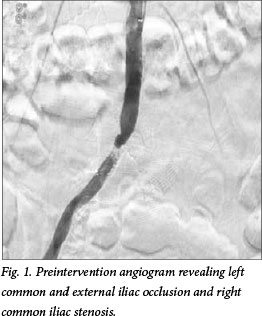
In May 2011, a 44-year-old man presented with a 3-week history of rest pain of the left leg due to aortoiliac occlusive disease. He had a 20 pack-year smoking history as his only risk factor for atherosclerosis. Both femoral pulses were absent. His ankle brachial index (ABI) was 0.65 on the right leg and 0.35 on the left. Initial arteriography was performed via the left brachial artery using a 6F 90 cm sheath (OptiMed, Germany), revealing a critical stenosis of the origin of the right common iliac artery and occlusion of the left common and external iliac arteries, with reconstitution of the left common femoral artery (Figs 1 and 2).
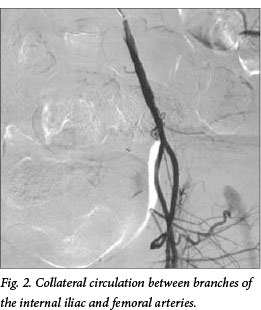
A guidewire test confirmed absence of fresh thrombus. Subintimal passage of a hydrophilic wire was followed by direct catheter canulation of the left internal iliac artery. Arteriography revealed a patent internal iliac artery and collateralisation to the femoral arteries (Fig. 2). A 5F Headhunter catheter (Cook Medical, USA) was advanced into the subintimal plane and entered the internal iliac artery.
Owing to his youth and the risk of extending long stents directly into the common femoral artery, we inserted shorter stents into the internal iliac artery, thus perfusing the lower limb via the cruciate anastomosis.
A 0.035-inch hydrophilic-coated guidewire (Terumo Medical Corporation, Japan) was exchanged for a stiff Lunderquist wire (Cook Medical, USA). The right common femoral artery was canulated with a 6F sheath (Cook Medical, USA) and a 0.035-inch hydrophilic-coated guidewire was navigated through the right common iliac stenosis. Predilatation was performed using 'kissing balloons', 6 - 40 mm on the right and 5 - 80 mm on the left (Medtronic, USA). Two nitinol endoprostheses were inserted: 8 - 60 mm from the right groin and 7 - 80 mm from the left arm (CR Bard Inc., USA). The left nitinol endoprosthesis was deployed first into the left internal iliac artery and extended about 2 cm into the aorta. Thereafter the right nitinol endoprosthesis was deployed using the left endoprosthesis as a marker for precise aortic position. Kissing balloons postdilatation was performed using 7 - 40 mm on the right and 6 - 80 mm on the left (Medtronic, USA).
A postprocedural arteriogram revealed adequate flow into the left internal iliac artery. Femoral pulses were palpable after the procedure. Clopidogrel was prescribed for an indefinite period. His postoperative course was unremarkable with complete resolution of his rest pain and an improvement of his ABI to 0.85 on the left. This was unchanged at the 6-month follow-up. He is assessed periodically and remains symptom free 2 years after the index procedure.
Discussion
Critical limb ischaemia due to TASC D aortoiliac lesions is classically treated by open surgery: fem-fem bypass and aortobifemoral bypass.[1] Alternatively, endovascular procedures are suggested by some authors. In the case described, this would have necessitated either extending the stents into the left common femoral artery or common femoral-external iliac endarterectomy and patching with subsequent inline stenting.
There is an extensive collateralisation between the internal iliac artery and branches of the common and profunda femoral arteries. These networks of collaterals are referred to as the cruciate and trochanteric anastomoses. The cruciate anastomosis involves the inferior gluteal, medial femoral circumflex, lateral femoral circumflex and the first perforating branch of the profunda femoral arteries. The trochanteric anastomosis is between the inferior gluteal, superior gluteal, medial circumflex femoral and lateral circumflex femoral arteries.
Reports highlight the relationship between internal iliac artery malperfusion and buttock and thigh claudication.[2-5]
A few case reports suggest that open surgical revascularisation of the internal iliac artery may be performed to salvage critical ischaemic limbs.[6-8] Hashemi et al.[6] described a patient with limb-threatening ischaemia after thrombosis of an aortobifemoral graft. A bypass procedure, using poly-tetrafluoroethylene (PTFE), was performed between the right limb of the aortobifemoral graft after thrombectomy and the right internal iliac artery. This resulted in relief of the rest pain and healing of the ischaemic leg ulcer. The graft thrombosed 1 year later and the patient underwent an above-knee amputation. Filho et al.[7]also described open surgical revascularisation of the left internal iliac artery in a patient with critical ischaemia. This case was anatomically similar to ours in that the left common and external iliac arteries were occluded together, with a 20 - 30% stenosis of the right proximal common iliac. Revascularisation was achieved using a 6 mm Dacron graft from the right distal external iliac artery to the left proximal internal iliac artery. The 20 - 30% stenosis of the right common iliac artery was not treated prior to the bypass. The patient was well and pain free at 5 months. Onohara et al.[8] reported a case of an acutely threatened limb caused by acute arterial thrombosis of the right internal iliac artery. After intra-arterial thrombolytic therapy revealed a stenotic lesion at the origin of the internal iliac artery, an open thrombo-endarterectomy resulted in limb salvage.
To our knowledge, only one other case report describes endovascular management of the internal iliac artery to salvage critical limb ischaemia. Garrido et al.[9] described a case of critical limb ischaemia with an ischaemic foot lesion. The patient had occlusion of the external iliac artery and a critical stenosis of the internal iliac artery. The common iliac artery was patent. Limb salvage was achieved by inserting a stent graft to treat the stenosis. The patient had resolution of rest pain and regression of the ischaemic foot lesion, with an ABI of 0.8 3 weeks after the procedure.
In our case, the patient had occlusion of the left common and external iliac arteries. We opted not to place long stents from the aorta into the left common femoral artery. The main body of the internal iliac artery was adequately patent with good collateral-isation to the femoral arteries (Fig. 3). Kissing stents were mandatory owing to the flush-left common iliac occlusion and the right common iliac stenosis. By performing kissing aortoiliac stenting and extending the left stent into the internal iliac artery, we were able to reperfuse the left leg and eliminate the patient's rest pain.

Conclusion
To our knowledge, this is the first published case of critical limb ischaemia, iliac occlusion and successful endovascular revascularisation of the internal iliac artery. Limb salvage was possible owing to extensive collateralisation between the internal iliac and femoral vessels.
REFERENCES
1. Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). Eur J Vasc Endovasc Surg 2007;33(1):suppl:S1-S75. [http://dx.doi.org/10.1016/j.ejvs.2006.09.024] [ Links ]
2. Engelke C, Elford J, Morgan RA, Belli AM. Internal iliac artery embolization with bilateral occlusion before endovascular aortoiliac aneurysm repair: Clinical outcome of simultaneous and sequential intervention. J Vasc Interv Radiol 2002;13(7):667-676. [ Links ]
3. Mehta M, Veith FJ, Darling RC, et al. Effects of bilateral hypogastric artery interruption during endovascular and open aorto iliac aneurysm repair. J Vasc Surg 2004;40(4):698-702. [http://dx.doi.org/10.1016/j.jvs.2004.07.036] [ Links ]
4. Chaer RA, Faries PL, Lin L, Dayal R, McKinsey JF, Kent KC. Successful percutaneous treatment of gluteal claudication secondary to isolated bilateral hypogastric stenosis. J Vasc Surg 2006;43(1):165-168. lhttp://dx.doi.org/10.1016/j.jvs.2005.09.026] [ Links ]
5. Donas KP, Schwindt A, Pitoulias GA, Schonefeld T, Basnera C, Torsello G. Endovascular treatment of internal iliac artery obstructive disease. J Vasc Surg 2009;49(6):1447-1451. [http://dx.doi.org/10.1016/j.jvs.2009.02.207] [ Links ]
6. Hashemi H, Massimiano P, Mukherjee D, Aryavand B. Internal iliac artery revascularization for limb salvage purposes. J Vasc Surg 2007;45(3):607-609. [http://dx.doi.org/10.1016/j.jvs.2006.10.036] [ Links ]
7. Filho HP, Batista MAR, Luccas GC. Revascularization of the internal iliac artery for critical lower limb ischemia treatment. J Vasc Br 2004;3(2):161-164. [ Links ]
8. Onohara T, Takahashi I, Nishizaki T, Wakasugi K, Matsusaka T, Kume K. Direct hypogastric artery reconstruction for threatened lower limb ischemia: Report of a case. Surg Today 2001;31(3):274-276. [ Links ]
9. Garrido SA, Mackenzie RL, Parodi MF, Caviglia J. Sténose de l'artere hypogastrique chez un patient en ischémie chronique severe. Ann Vasc Surg 2010;24(6):900e1-900e4. [http://dx.doi.org/10.1016/j.acvfr.2011.01.030] [ Links ]
 Correspondence:
Correspondence:
C Yazicioglu
c_yazicioglu@yahoo.com

