










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.52 n.4 Cape Town Nov. 2014
http://dx.doi.org/10.7196/sajs.1904
CASE REPORT
Largest recorded non-invasive true intrathoracic desmoid tumour
G R Alexander
MB ChB, FC Cardio SA, MMed (Cardiothorac Surg); Inkosi Albert Luthuli Central Hospital, Durban, South Africa
ABSTRACT
Intrathoracic desmoid tumours are rare soft-tissue neoplasms arising from fascial or musculo-aponeurotic structures, accounting for less than 0.03% of all neoplasms. Most cases in fact represent intrathoracic extension of chest wall tumours. This case report describes the largest recorded true intrathoracic desmoid tumour without mediastinal or chest wall invasion. The tumour was completely excised through a left thoracotomy with negative tumour margins. Management of the patient will involve radiological surveillance. Desmoids are benign tumours that do not metastasise but have a high rate of recurrence, especially if tumour margins are positive after surgical resection. Complete surgical resection is the treatment of choice. Other treatment options include radiotherapy; non-steroidal inflammatory drugs or antioestrogen therapy (tamoxifen) or a combination thereof; and chemotherapy or targeted drug therapy.
Desmoid tumours are rare monoclonal fibroblastic proliferations arising in the soft tissue and accounting for less than 0.03% of all neoplasms. These benign neoplasms are locally invasive and tend to recur, but do not metastasise.
Desmoid tumours generally occur between the ages of 15 and 60 years.[1,2] Two different types have been described: a sporadic type, and a familial type in which the tumours are usually intra-abdominal.[2,3] The chest wall is the most common site for extra-abdominal desmoid tumours, with true intrathoracic tumours being extremely rare. Patients with intrathoracic desmoid tumours are usually asymptomatic and generally present when the lesion is large enough to cause compression of vital structures or erosion into adjacent bone or joints.
These tumours resemble sarcomas both clinically and histologically. Although not specific, beta-catenin and mutations thereof are highly sensitive for sporadic desmoid tumours.[3] First-line therapy is complete surgical resection if this will not result in unacceptable morbidity.
Case report
A 17-year-old boy was referred to the Department of Cardio-thoracic Surgery at Inkosi Albert Luthuli Central Hospital (IALCH), Durban, South Africa, with a history of worsening dyspnoea and constitutional symptoms. Two years previously, he had been found to have an incidental pleural opacity on a chest radiograph taken following blunt thoracic trauma. He had been discharged but was lost to further review.
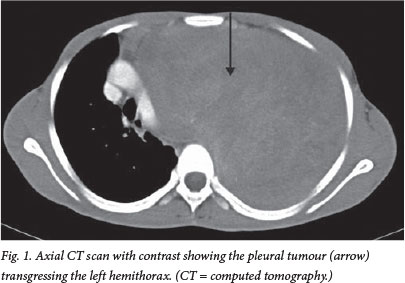
The chest radiograph on admission suggested pleural space occupation with contralateral mediastinal shift. A computed tomography (CT) scan of the chest and mediastinum confirmed a pleural mass of about 25 cm χ 17 cm with mediastinal shift and compression of the underlying left lung (Fig. 1). A core biopsy of the pleural mass was suggestive of a spindle cell tumour, but the differential diagnosis varied widely and included fibromatosis.
A left exploratory thoracotomy was considered suitable. Owing to the large size of the tumour, a second thoracotomy and anterior osteotomies of ribs 8 - 10 were done to facilitate extraction of the tumour from the thorax. There was no invasion of any mediastinal structures or the diaphragm. Complete adhesiolysis of the tumour was performed using a combination of sharp and blunt dissection. The tumour was attached near the apex of the hemithorax, closely abutting the brachial plexus and the first two ribs posteriorly. It was then successfully completely removed, albeit in several large pieces owing to its enormous size. There was no residual disease.
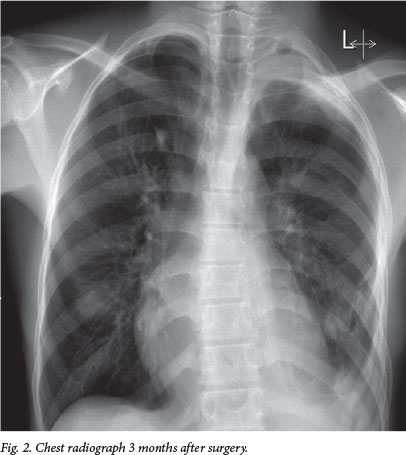
The underlying lung appeared normal and eventually re-expanded completely. The patient's postoperative course was uneventful, and he was discharged a week after surgery. He is due to be followed up in the Department of Oncology at IALCH and will require radiological surveillance. Fig. 2 shows a chest radiograph 3 months after surgery. Histological examination of the resected 3.3 kg specimen confirmed a desmoid tumour.
Discussion
Desmoid tumour is a rare heterogenous disease requiring individualised therapy to reduce the possibility of local recurrence. True intrathoracic desmoid tumours are defined as desmoid tumours originating within the pleura or mediastinum, with the majority of the tumour located within the thoracic skeleton and associated with minor chest wall involvement. There have only been two reported cases of desmoid tumours originating from the visceral pleura or pulmonary parenchyma.[1] The present case is the largest reported true intrathoracic desmoid tumour appearing to originate from the parietal pleura without chest wall involvement.
Intrathoracic tumours usually present with compression or invasion of the surrounding intrathoracic structures. When true intrathoracic desmoid tumours are discovered they are therefore larger than other desmoid tumours, which have an average size of 10 cm.
Increased incidences of desmoid tumours have been associated with pregnancy and exposure to oral contraceptives. Spontaneous tumour regression has been reported during menopause, and has formed the basis of treatment with hormonal therapy.
Numerous hypotheses regarding the cause of these tumours have been suggested, including abnormal scarring from previous trauma in up to 25% of cases, hormonal factors (oestrogen) and familial predisposition.[2]
Most desmoid tumours with bony involvement are detectable on a chest radiograph. A CT scan usually further elucidates the size and location of the tumour. Magnetic resonance imaging is more sensitive in determining soft-tissue infiltration and local recurrence[4]
Adequate surgical resection with negative tumour margins is the mainstay of treatment. While no data from randomised controlled trials have demonstrated any effect of microscopic tumour status on local recurrence,[1] surgery should nevertheless aim to achieve complete tumour excision.
If complete surgical resection is not possible, treatment options include neoadjuvant radiotherapy to reduce tumour size to permit resection or achieve a possible cure;[2] postoperative brachytherapy or intraoperative radiation therapy to kill remaining tumour cells; non-steroidal inflammatory drugs, antioestrogen therapy (tamoxifen) or a combination thereof; and chemotherapy or targeted drug therapy.[3,5]
Radiotherapy alone and surgery combined with radiotherapy result in better local control than surgery alone. Even in patients with positive margins following surgery, adjuvant radiotherapy resulted in a significant decrease in recurrence.[2] However, radiotherapy should be used judiciously to avoid the complications of tissue fibrosis and radiation-induced neoplasms, which are of particular concern in the young patient.[2,3]
The recurrence rate varies from 29% to 54%, with a longer disease-free interval associated with negative resection margins.[1,2] Most of these tumours recur within 2 years after resection.[2] Repeat resection or radiation after surgery achieves a control rate of up to 80%.[1]
Regular follow-up imaging is necessary even if the tumour margins are free of tumour.[1] Positron emission tomography may be used for monitoring therapeutic management because it is able to detect slight differences of density between desmoid tumours and surrounding structures. These tumours are slow-growing, so surveillance positron emission tomography scans may be undertaken at 3-monthly intervals for the first 2 years.[2,3]
REFERENCES
1. Yadav Y, Patel MD, Kumar T, Ravi K, Patel MH, Kothari K. Case report of largest primary intrathoracic desmoid tumour with review of literature. Austral-Asian Journal of Cancer 2013;12(1):57-62. [ Links ]
2. De Jong WK, van der Graaf WTA, van der Jagt EJ, et al. Case for Diagnosis: A 20 year old male with thoracic pain and a lower thoracic mass. Eur Respir J 2005;26(4):740-743. [http://dx.doi.org/10.1183/09031936.05.00051605] [ Links ]
3. Kasper B, Strobel P, Hohenberger P. Desmoid tumours: Clinical features and treatment options for advanced disease. Oncologist 2011;16(5):682-693. [http://dx.doi.org/10.1634/theoncologist.2010-0281] [ Links ]
4. Iqbal M, Rossoff LJ, Kahn L, Lackner RP. Intrathoracic desmoid tumour mimicking primary lung neoplasm. Ann Thorac Surg 2001;71(5):1698-1700. [http://dx.doi.org/10.1016/S0003-4975(00)02296-7] [ Links ]
5. Meyerson ML, D'Amico TA. Intrathoracic desmoid tumour: Brief report and review of literature. J Thorac Oncol 2008;3(6):656-659. [http://dx.doi.org/10.1097/JTO.0b013e3181757aa6] [ Links ]
 Correspondence:
Correspondence:
G Alexander
(gerardale@ialch.co.za)

