










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Surgery
versión On-line ISSN 2078-5151
versión impresa ISSN 0038-2361
S. Afr. j. surg. vol.52 no.4 Cape Town nov. 2014
http://dx.doi.org/10.7196/sajs.1995
TRAUMA
An audit of trauma-related mortality in a provincial capital in South Africa
N B MoodleyI; C AldousII; D L ClarkeIII
IMB ChB; Department of Surgery, Nelson R Mandela School of Medicine, College of Health Sciences, Durban, South Africa
IIPhD; Department of Surgery, Nelson R Mandela School of Medicine, College of Health Sciences, Durban, South Africa
IIIMB BCh, FCS (SA), MMedSci, MPhil, MBA; Department of Surgery, Nelson R Mandela School of Medicine, College of Health Sciences, Durban, South Africa
ABSTRACT
INTRODUCTION: It has been shown repeatedly that hospital-based mortality data do not capture the actual mortality rate in South Africa, as many corpses are taken directly to the state mortuary
OBJECTIVE: To present a comprehensive overview of the forensic mortality data for trauma in an urban metropolitan complex
METHODS: A retrospective audit was conducted by reviewing all mortuary reports for the period 1 January 2010 - 31 December 2011. The data recorded included demographics, mechanism of trauma, and cause and site of death
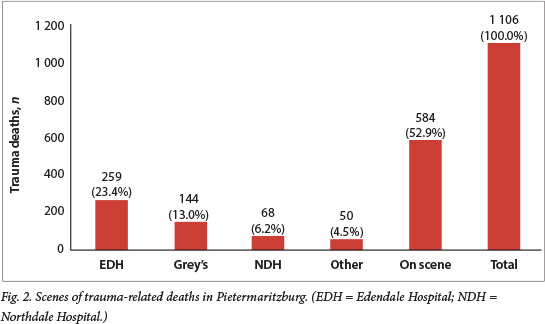
RESULTS: A total of 1 105 trauma victims died. There were 930 males (84.2%) and 175 females (15.8%), of whom 615 were victims of blunt trauma (55.7%) and 490 victims of penetrating trauma (44.3%). The scenes of death were: on scene 584 (52.9%), Edendale Hospital 259 (23.4%), Grey's Hospital 144 (13.0%), Northdale Hospital 68 (6.2%), and 'other' 50 (4.5%). The 'other' group comprised nine deaths at primary healthcare clinics and 41 at private hospitals in Pietermaritzburg. Of deaths related to blunt trauma, 153 (24.9%) were secondary to assault and 462 (75.1%) to a road traffic collision. Of the victims of penetrating trauma, 81 (36.9%) had sustained gunshot wounds and 309 (63.1%) stab wounds. The three leading causes of trauma-related deaths were head injuries (32.6%), polytrauma (29.7%) and chest injuries (27.4%
CONCLUSIONS: Pietermaritzburg has both a high rate of trauma-related mortality and an immature trauma system, resulting in a significant number of preventable deaths
Trauma in South Africa (SA) was described as a malignant epidemic over two decades ago, and this remains an apt term.[1] An epidemic demands a co-ordinated and systematic public health response, and there has been much interest in developing an appropriate and sustainable trauma system for SA.[1-4] Part of the public health response to an epidemic is the development of a comprehensive registry that allows tracking of the disease. Although there has been some progress in this regard over the past 5 years, mortality data remain a concern.[5] Research from SA has shown repeatedly that hospital-based mortality data do not capture the actual mortality rate, as many corpses are taken directly to the state mortuary,[6-9-resulting in significant under-reporting of trauma-related mortality rates. This study was designed to provide a comprehensive overview of forensic trauma-related mortality data for a 2-year period in Pietermaritzburg, the capital city of KwaZulu-Natal Province (KZN), and its metropolitan drainage and to identify relationships between the mechanisms of trauma, injury patterns and death.
Setting
The Pietermaritzburg Trauma Service functions as a trauma service rather than a trauma centre, and attempts to deliver trauma care across the metropolitan complex of Pietermaritzburg and provide strategic and political leadership in trauma care to the western rural health districts of KZN. Pietermaritzburg is the capital of KZN and is the largest city in the western part of the province. The 2011 census estimated the population of Pietermaritzburg to be 1 017 763 people, with a density of 1 771 inhabitants per square kilometre.[10] It is served by a tertiary hospital (Grey's), a regional hospital (Edendale) and a district hospital (Northdale). There are four private hospitals in the city. All forensic work is undertaken at the government mortuary based at Fort Napier in the city centre. Under SA law, all trauma-related fatalities must undergo a mandatory police postmortem.
Trauma patients are coded red, yellow or green by the emergency services. A red code patient is stretcher bound and has deranged physiology, a yellow code patient is not stretcher bound but has deranged physiology, and a green code patient is mobile and has normal physiology. For purposes of the emergency services, the city is divided into two functional zones. Patients from zone 1 are taken to Northdale Hospital and those from zone 2 to Edendale Hospital. However, victims of major trauma (red code) in zone 1 are supposed to bypass Northdale and be taken directly to Grey's. In a mass casualty situation, the metropolitan protocol states that two-thirds of red code trauma patients are distributed to Edendale and one-third to Grey's, while two-thirds of yellow code patients are distributed to Grey's and one-third to Edendale and all green code patients are distributed equally between Northdale and Edendale.
Methods
Ethics approval was obtained before commencing the study (BE 177/11). A retrospective audit was undertaken of all trauma patients presenting to the outpatient departments of the three government hospitals in Pietermaritzburg, as well as all the Pietermaritzburg state medicolegal mortuary reports of trauma-related deaths. Data were manually entered into a spreadsheet for the 2-year period 1 January 2010 - 31 December 2011. The data entered included demographic data and the mechanism of trauma, classified as blunt (assault or road traffic collision (RTC)) or penetrating (gunshot or stab). Cause of death as recorded in the mortuary register was noted. The site of death was also recorded and grouped as having occurred on scene or at Grey's Hospital, Edendale Hospital, Northdale Hospital or 'other', which included clinics and private hospitals in and around Pietermaritzburg. Statistical analysis was performed using Microsoft Excel 2010 (version 14.0).
Results
During the 2-year period under review, a total of 10 644 trauma victims were seen at the three hospitals comprising the Pietermaritzburg state hospital complex. There were 8 194 males (77.0%) and 2 450 females (23.0%). The trauma burden consisted predominantly of blunt trauma (69.6%), followed by penetrating trauma (30.4%). The blunt trauma group comprised 3 688 victims of assault (34.6%) and 3 715 victims of RTCs (34.9%). The penetrating trauma group comprised 516 victims of gunshot wounds (GSWs) (4.8%) and 2 725 (25.6%) victims of stab wounds. A total of 510 patients (4.8%) needed admission to an intensive care unit.
During this period, a total of 1 105 victims of trauma died as a result of their injuries (930 males (84.2%) and 175 females (15.8%), mean age 33.9 years). The group comprised 615 victims of blunt trauma (55.7%) and 490 of penetrating trauma (44.3%) (Fig. 1). The scenes of the deaths were as follows: 584 (52.9%) on scene, 259 (23.4%) at Edendale Hospital, 144 (13.0%) at Grey's Hospital, 68 (6.2%) at Northdale Hospital, and 50 (4.5%) 'other'. Nine fatalities were recorded from the primary healthcare clinics in Pietermaritzburg, and there were 41 deaths at the private hospitals in the city (Fig. 2). Comparing the 521 (47.1%) in-hospital with the 584 (52.9%) on-scene deaths, the majority of in-hospital deaths were due to an RTC mechanism (n=251, 48.2%) and the majority of the on-scene deaths to stabbings (n=212, 36.3%) (Fig. 3). A total of 159 on-scene deaths from stab wounds (75.0%) were due to penetrating chest injuries, of which 38 (23.9%) were penetrating cardiac injuries.
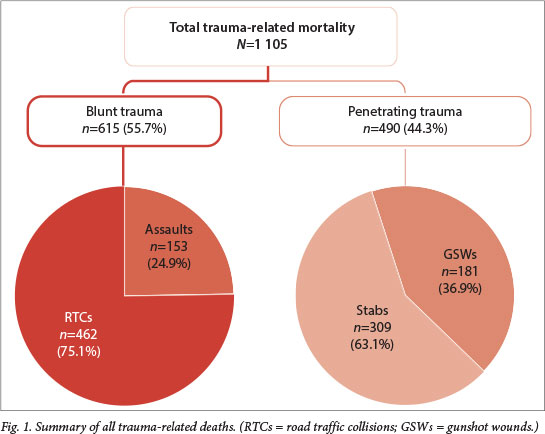

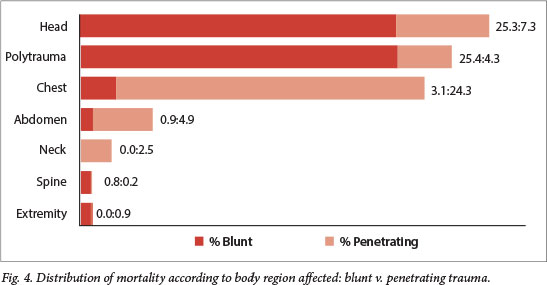
Of the 615 deaths related to blunt trauma, 153 (24.9%) were secondary to assault and 462 (75.1%) to an RTC. RTCs ultimately contributed to 41.8% of the overall trauma mortality. Of the victims of penetrating trauma, 181 (36.9%) had sustained gunshot wounds and 309 (63.1%) had been stabbed. The three leading causes of trauma-related deaths were head injuries (32.6%), polytrauma (29.7%) and chest injuries (27.4%). The majority of the polytrauma deaths (86.6%) and head injury-related deaths (77.6%) were due to blunt trauma. Deaths related to chest injuries were overwhelmingly due to penetrating trauma (88.8%) (Fig. 4).
Discussion
The trauma burden in SA remains significant, and the country experiences over 30 000 trauma-related deaths annually.[11] This figure represents almost two-thirds of the 46 000 annual trauma fatalities for the whole of Europe.[12] The accuracy of epidemiological data in SA and the developing world in general remains of concern. It has been shown repeatedly in research from SA that hospital-based mortality data do not capture all mortality, as many corpses are taken directly to the state mortuary without ever reaching a hospital,[5-9] resulting in significant underreporting of the actual trauma-related mortality rate. Our data confirm this, as almost half of the deaths occurred on scene, before the patient could be transported to hospital.
Interpersonal violence continues to be a major contributor to trauma-related deaths in SA, as evidenced by our figure of 58.2% (n=643) for assaults, gunshots and stabbings. This excessive burden of interpersonal violence is demonstrated by the high proportion of penetrating to blunt trauma, and the 1:1 ratio of intentional to non-intentional blunt trauma.[1-4]
Trauma trends do seem to be changing, however. In the present study, blunt trauma contributed to 55.7% (n=615) of all deaths - this stands in stark contrast to the almost 90% of trauma mortality being secondary to penetrating trauma reported from nearby Durban in the mid-1990s.[1,6,7] This shift to a predominance of blunt trauma is partly due to an increase in road traffic-related injuries, which constituted 41.8% (n=462) of all trauma deaths in the current study. Rapid urbanisation and the increasing numbers of vehicles on the roads contribute to this burden. RTCs are a major cause of morbidity and mortality, and are extremely expensive to treat.[9,13] This pattern brings SA figures more in line with those reported from the developed world, where, for example, RTCs are responsible for up to 50% of trauma mortality burden in cities such as Milan, Italy.[12] The wider economic impact of RTCs remains to be estimated in the SA context.
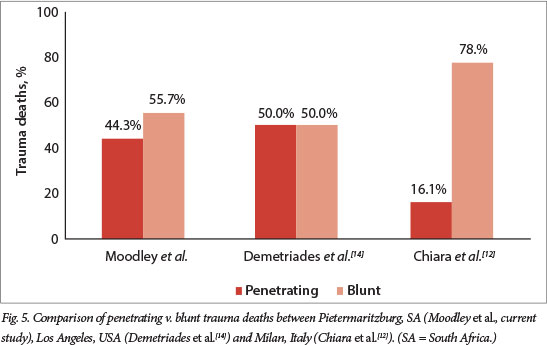
Other series reported from SA have suggested that the rate of GSWs is decreasing and has stabilised at 10 - 20% of all trauma-related incidents.[4,5,8] This implies that the new firearm control policies are effective and is cause for cautious optimism; however, mortuary statistics suggest that the actual rate of firearm-related trauma is higher than that obtained from hospital statistics. Firearm injuries comprise 15.9% of all penetrating injuries seen in Pietermaritz-burg, but 36.9% of all penetrating injury-related deaths. Firearm injuries remain more lethal than stab injuries, and penetrating trauma remains more lethal than blunt trauma.[1,6,7] Head trauma and polytrauma deaths are predominantly due to blunt trauma. Chest injury- and abdominal injury-related deaths, however, are predominantly due to penetrating trauma. When compared with studies in Los Angeles, USA,[14] and Milan,[12] our findings with regard to the preponderance of blunt trauma due to RTCs are similar (Fig. 5). We found that the overall contribution of gunshot wounds to trauma mortality is 16.4%, which is significantly lower than the 45.9% documented by Demetriades et al.[14](Fig. 6). Our incidence of fatal low-velocity interpersonal trauma is much higher than that documented by Demetriades et al.,[14] however, confirming that SA is still afflicted with a major problem of interpersonal violence.

There are two potential explanations for why more victims died on scene than in hospital. The majority of on-scene deaths were due to penetrating chest injuries, with penetrating cardiac injuries making up a large number of these. A second reason is that the prehospital service in Pietermaritzburg is immature. In a mature trauma system, one would expect most trauma-related deaths to take place in hospital. This issue of the prehospital component of a trauma system remains a neglected topic in South Africa. The concept of a trauma system is that injured patients are taken to the most appropriate facility to manage their degree of injury definitively. First-phase mortality is due to massive non-survivable injury, and its incidence can only be reduced by preventive strategies. So-called 'second-phase mortality' occurs in the few hours after the incident.[1] This period is referred to as the 'golden hour', and it is here that efficient resuscitation should reduce mortality. As has been pointed out by a number of commentators, the factors that determine favourable outcome in this cohort are appropriate prehospital care, triage, transportation to a trauma facility, prompt assessment and appropriate emergency management. Of the 521 deaths at the various medical facilities in Pietermaritzburg, 77 (14.8%) occurred at facilities that are not adequately equipped to treat severely injured patients. This implies failure to follow referral protocols and poor triage capacity on the part of the emergency rescue services. The development of an appropriate trauma registry that can be used in rural hospitals is an urgent requirement, and this registry must incorporate forensic data if it is to provide meaningful information.
Reducing trauma mortality in SA remains a challenge. The relative decline in GSWs in total and as a contribution to mortality is cause for optimism. The increased contribution in RTCs as a cause of mortality is in keeping with predicted trends and should spur broader civil society into developing active injury prevention programmes. The issue of the inadequacy of the prehospital service needs to be addressed urgently. An effective trauma system must ensure that patients are taken to the appropriate facility to treat their level of trauma. This does not appear to be happening, and needs to be addressed.
Conclusion
Pietermaritzburg has a large volume of trauma-related mortality. The proportion of blunt to penetrating trauma as a contribution to this mortality is similar to that documented by trauma units in North America but quite different to that in Europe. Although it would appear that GSWs have declined as a mechanism, high levels of interpersonal violence result in stabbings and assault-related trauma being major contributors to trauma mortality. The trauma system in the city is immature. Poorly defined and executed referral protocols result in a significant number of potentially preventable second-phase deaths as severely injured trauma patients are taken to inappropriate facilities.
REFERENCES
1. Muckart DJ. Trauma - the malignant epidemic. S Afr Med J 1991;79(2):93-95. [ Links ]
2. Norman R, Matzopoulos R, Groenewald P, et al. The high burden of injuries in South Africa. Bull World Health Organ 2007;85(9):695-702. [http://dx.doi.org/10.2471%2FBLT.06.037184] [ Links ]
3. Seedat M, van Niekerk A, Jewkes R, et al. Violence and injuries in South Africa: Prioritizing an agenda for prevention. Lancet 2009;374(9694):1011-1022 [http://dx.doi.org/10.1016/S0140-6736(09)60948-X. [ Links ]]
4. Hardcastle TC, Samuels C, Muckart DJ. An assessment of the hospital disease burden and the facilities for the in-hospital care of trauma in KwaZulu-Natal, South Africa. World J Surg 2013;37(7):1550-1561. [http://dx.doi.org/10.1007/s00268-012-1889-1] [ Links ]
5. Laing GL, Bruce JL, Aldous C, et al. The design, construction and implementation of a computerized trauma registry in a developing South African metropolitan trauma service. Injury 2014;45(1):3-8. [http://dx.doi.org/10.1016/j.injury.2013.05.013] [ Links ]
6. Campbell NC, Thomson SR, Muckart DJ, et al. Review of 1198 cases of penetrating cardiac trauma Br J Surg 1997;84(12):1737-1740. [ Links ]
7. Muckart DJ, Meumann C, Botha JB. The changing pattern of penetrating torso trauma in KwaZulu-Natal - a clinical and pathological review. S Afr Med J 1995;85(11):1172-1174. [ Links ]
8. Clarke DL, Quazi MA, Reddy K, et al. Emergency operation for penetrating thoracic trauma in a metropolitan surgical service in South Africa. J Thorac Cardiovasc Surg 2011;142(3):563-568. [http://dx.doi.org/10.1016/j.jtcvs.2011.03.034. [ Links ]]
9. Parkinson F, Kent SJ, Aldous C, et al. The hospital cost of road traffic accidents at a South African regional trauma centre: A micro-costing study. Injury 2014;45(1):342-345. [http://dx.doi.org/10.1016/j.injury.2013.04.007] [ Links ]
10. Statistics South Africa. Census 2011 Municipal report - KwaZulu-Natal/Statistics South Africa. Pretoria: Statistics South Africa, 2012. www.statssa.gov.za/Census2011/Products/KZN_Municipal_Report.pdf. (accessed 16 June 2014). [ Links ]
11. MRC/UNISA Crime, Violence and Injury Lead Programme. A profile of fatal injuries in South Africa 2008 - Annual Report for South Africa based on National Injury Mortality Surveillance System. www.mrc.ac.za/crime/nimss07.PDF (accessed 12 April 2014) [ Links ]
12. Chiara O, Scott J, Cimbanassi S. Trauma deaths in an Italian urban area: an audit of pre-hospital and in-hospital trauma care. Injury 2002;33(7):553-562. [http://dx.doi.org/10.1016/S0020-1383(02)00123-7] [ Links ]
13. Parkinson F, Kent S, Aldous C, et al. Road traffic crashes in South Africa: The burden of injury to a regional trauma centre. S Afr Med J 2013;103(11):850-852. [http://dx.doi.org/10.7196/SAM.6914] [ Links ]
14. Demetriades D, Velhamos G, Rhee P, et al.Trauma deaths in a mature urban trauma system: Is 'trimodal' distribution a valid concept? J Am Coll Surg 2005;201(3):343-348. [http://dx.doi.org/10.1016/j.jamcollsurg.2005.05.003] [ Links ]
 Correspondence:
Correspondence:
D L Clarke
(damianclar@gmail.com)

