










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Surgery
versión On-line ISSN 2078-5151
versión impresa ISSN 0038-2361
S. Afr. j. surg. vol.52 no.2 Cape Town feb. 2014
TRANSPLANTATION
Retroperitoneoscopic live donor nephrectomy: Review of the first 50 cases at Tygerberg Hospital, Cape Town, South Africa
A van der MerweI; C F HeynsII
IMB ChB, MRCS (Engl), MRCS (Edin), MMed (Urol), FC (Urol) (SA); Department of Urology, Faculty of Medicine and Health Sciences, Stellenbosch University and Tygerberg Hospital, Tygerberg, Cape Town, South Africa
IIPhD; Department of Urology, Faculty of Medicine and Health Sciences, Stellenbosch University and Tygerberg Hospital, Tygerberg, Cape Town, South Africa
ABSTRACT
BACKGROUND: Changing from an open to a laparoscopic live renal donor programme poses challenges and may affect donor and graft outcomes.
OBJECTIVES: To evaluate donor safety and graft outcomes for the first 50 retroperitoneoscopic live donor nephrectomies performed at Tygerberg Hospital, Cape Town, South Africa.
METHODS: The procedures were performed by a single surgeon from 8 April 2008 to 3 April 2012. Operative and anatomical data were prospectively collected. A flank approach with lateral and posterior placements was used. Vascular control was achieved with Hem-o-lok clips in the majority of cases.
RESULTS: The mean age of the donors was 31.5 years (range 18 - 50), 28 (56.0%) were male, and the left kidney was harvested in 28 (56.0%) of cases. The mean operating time was 149.8 minutes (range 75 - 250), mean warm ischaemic time (WIT) 181.3 seconds (107 - 630), mean blood loss 139.7 ml (5 - 700) and mean hospital stay 3.2 days (2 - 5). Mean WIT was significantly longer for right-sided than left-sided nephrectomy (213 v. 162 seconds). In two right-sided cases the renal vein was too short and vena profunda femoris was used to create length. No donor received a blood transfusion. Comparing the last 25 with the first 25 cases showed a significant decrease in mean WIT (158 v. 204 seconds, respectively) and operating time (128 v. 172 minutes, respectively). No major complications occurred.
CONCLUSION: Our initial 50 retroperitoneoscopic live donor nephrectomies were performed without major complications. Donor safety was maintained during the early learning curve of the transition to minimal-access donor nephrectomy.
Laparoscopic live donor nephrectomy was performed for the first time in 1995.[1] Donors experience less pain, return to work earlier and are more satisfied with the scar after minimalaccess nephrectomy.[2-4] Schweitzer et al.[5] reported that laparoscopic donor nephrectomy increased the number of live donors by 20%. According to Greco et al.,[6] laparoscopic, retroperitoneoscopic and open donor nephrectomy are all accepted as standard of care. The retroperitoneal laparoscopic approach is particularly suitable for obese patients or a 'vessels-first' approach, but the working space in the initial stages of the operation is limited and may increase the degree of difficulty.
Setting
Tygerberg Hospital is an academic teaching hospital for the Faculty of Medicine and Health Sciences of Stellenbosch University, Western Cape, South Africa. The first renal transplant in this faculty was performed in 1976 at Karl Bremer Hospital, the teaching hospital at that time, and a well-established transplantation programme exists. Our patients generally present late in renal failure and often require immediate haemodialysis. Surgical construction of an arteriovenous fistula is often delayed, resulting in prolonged dialysis through catheters inserted in the iliac veins. This leads to phlebitis and thrombosis which makes graft implantation more difficult and increases the risk of graft morbidity.
The transition from open to minimal-access donor nephrectomy may be difficult and risky, so we analysed our prospectively collected data after the first 50 cases.
Methods
Donors and recipients at our institution are evaluated by a team consisting of transplant nephrologists, surgeons (urological and vascular), transplant co-ordinators, a social worker trained in transplant psychology, and clinical psychologists when required. Once patients have been completely screened and have agreed to a family renal donor/recipient pair, consent is obtained for retroperitoneoscopic renal harvesting with the option to convert to open surgery if required. The side is selected on the basis of radioisotope renography and vascular anatomy seen on computed tomography (CT) with three-dimensional reconstruction.
The anaesthetised patient is placed in the flank position as for an open extraperitoneal nephrectomy. Instruments for open nephrectomy are available from the start of the procedure in all cases. A routine three-port extraperitoneal access is created using either a commercially available or a hand-made inflation balloon. Dissection of the renal hilum is followed by freeing the kidney from the perinephric tissues and lastly transecting the ureter at the pelvic brim, saving as much peri-ureteric tissue as possible to retain the blood supply to the ureter. Vessel-sealing devices are not used for haemostasis and small vessels are managed with clips. The renal artery and vein are dissected completely free from all perivascular tissues to make accurate and effective clip placement possible.
A small muscle-splitting incision is made in the ipsilateral groin area, just large enough to allow the surgeon's hand access to the operating field. The kidney is elevated and each of the the vessels clipped with two XL Hem-o-lok clips (Teleflex Medical, Research Triangle Park, NC, USA). Vascular stapling devices (cutting and non-cutting) were employed for a few cases, but are not freely available at our hospital and are not favoured in the presence of small clips around the vessels that may cause staple failure.
The term hand extraction is preferred to hand-assisted nephrectomy, as the full dissection should be completed before the surgeon's hand is inserted. Hand placement too early may be counter-productive. Warm ischaemic time (WIT) was measured from the occlusion of the renal artery until the artery was connected to the cold irrigation fluid. Operating time was measured from the insertion of the first port until the kidney was removed. The time required for closure of ports and extraction incisions was not included, because both surgeon and assistant attended to the graft once donor safety was established. Blood loss was estimated and recorded by the anaesthetist.
Statistical analysis
Statistical analysis was performed with the t-test for unpaired data using GraphPad Prism Software. Values are expressed as mean (standard deviation).
Results
The donor characteristics and operative parameters are summarised in Table 1. There were 28 male and 22 female live kidney donors. The left kidney was harvested in 28 cases and the right kidney in 22. Three-port access was used in 46 cases and four ports in four. There were no conversions to open surgery and no intra-or postoperative deaths.

CT reported a single artery in all cases, but two arteries were found at surgery in three cases. CT reported a single renal vein in 49 cases, but two veins were found in six cases, three veins in one and four veins in one. CT reported two veins in one case, but four veins were found at surgery. Two grafts were lost in the 4th and 28th cases at 4 days and 6 weeks postoperatively, respectively. Problems at the vascular anastomosis were the most likely reason.
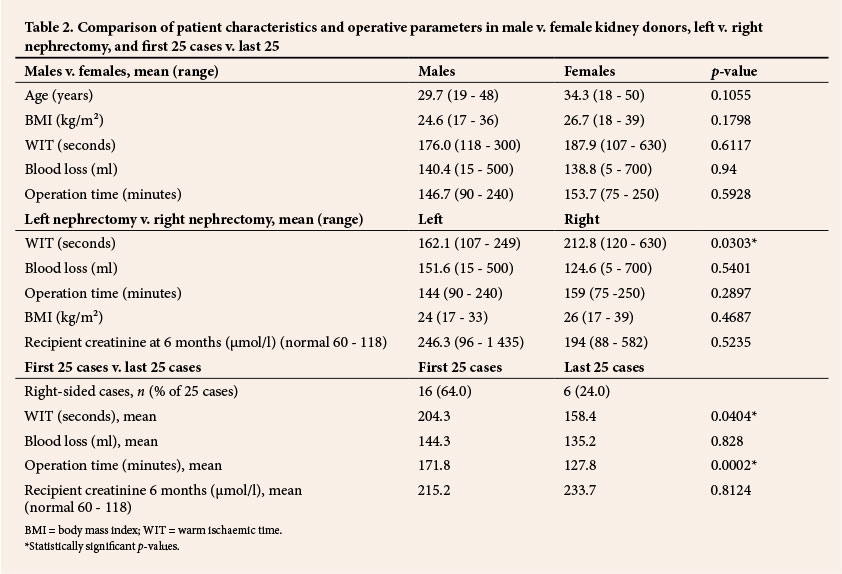
Comparing male and female donors showed no statistically significant differences (Table 2). Comparing left and right donor nephrectomy showed a significantly shorter mean WIT for left donor nephrectomy (Table 2). Comparing the first 25 with the last 25 cases showed a significantly shorter mean WIT and a shorter mean operating time (Table 2).
Intraoperative complications were two renal vein reconstructions for short right-sided renal veins. Postoperative complications were severe bladder infection with Klebsiella spp. in one case, urethral injury in one donor whose catheter was removed without deflation of the balloon, and acute gastritis in one donor.
Discussion
Retroperitoneal laparoscopic donor nephrectomy has been performed in France since 1998. The initial cases took an average of 280 minutes and were done in the lumbotomy (prone) position with good results.[7] This relatively long operating time for a centre of laparoscopic excellence may perhaps be ascribed to the reduced operating space provided by this approach.
The mean age of the donors in our series was 15 - 22 years, less than in the three comparative series[8-10] (Table 3). The mean WIT in our series compares well with the other series. Mean blood loss was higher than in two of the other series, probably attributable to one case in our series with blood loss of 700 ml when four renal veins were encountered instead of the single one reported on CT (Table 3). Mean hospital stay was shorter than in two of the comparative series.
Use of Hemo-o-lok clips for the renal artery and vein is controversial. A strong plea for the use of transfixing techniques has been made by Friedman et al.[11-13] and the Federal Drug Administration (FDA) in the USA. According to Friedman et al., the cause of donor death in many cases was lack of proper pain relief postoperatively. The resulting increased blood pressure in a healthy donor is enough to overcome the resistance of a non-transfixed clip on the renal artery. Equally strong arguments have been published for the use of Hem-o-lok clips.[14,15]
Endovascular transfixing stapler devices are not without problems. Chan et al.[16] and Deng et al.[17] reviewed their own cases and the literature and found two donor deaths as a consequence of stapler failure. The FDA recommends that vessel sealing devices and a variety of stapling devices should be routinely available. However, owing to cost constraints this is not attainable in our setting. When vessel sealing haemostatic devices are used for hilum dissection there are no clips in the path of stapler devices, which may cause them to fail. We sometimes use multiple titanium or Hem-o-lok clips for smaller vessels, prior to managing the renal vessels. In the presence of these clips, stapler failure becomes an unacceptably high risk. We therefore remove as much perivascular tissue from the renal vessels as possible, leave a long vascular stump, and routinely place two clips on the proximal vessel to decrease the risk of clip disengagement. The fact that the same surgeon performs the donor and recipient operation may remove some stress, as the length of the renal graft vessels becomes less of a potential issue.
In our series, as in the report by Tanabe et al.,[10] the surgical time was defined as the time from the first port insertion until removal of the kidney. The mean surgical time in our series was shorter than in the study of Tanabe et al.,[10] similar to that reported by Bachmann et al.[8] and slightly longer than that reported by Ma et al.[9] (Table 3).
In our series the proportion of right-sided nephrectomies was considerably higher than in the compared series (Table 3). Right-sided nephrectomy is perceived as being easier because the adrenal and gonadal veins are not involved, but is reported to have the same complication risk as the left side.[3,18-20] The choice of side should be determined by the findings on renography and CT angiography. We currently prefer the left side if favourable, because the renal vein is longer.
In this series, graft function appeared to be worse than reported in the literature. This can possibly be explained by the difficulties experienced during graft vascular anastomosis mentioned above, and is unlikely to be related to the donor surgery. In this series, the CT report on the number of renal veins was wrong in a higher proportion of cases than reported in the literature. Gluecker et al.[21] reported that their CT scans were accurate in 35/36 renal arteries and in all renal veins in the same live donors when confirmed at surgery. We may have a higher proportion of incorrect findings because we terminate the CT before the late venous phase to limit radiation exposure to the donor.
In this series, right-sided donor nephrectomy had a significantly longer WIT than left donor nephrectomy, possibly because the right-handed surgeon found it awkward to lift up the right-sided kidney at extraction, or as part of the early learning curve, as 16 out of the first 25 cases were right sided. However, slightly increased WIT had no significant effect on graft function at 6 months (Table 2). During the first 25 cases the mean WIT and surgical times were significantly longer than in the subsequent 25 cases. This may indicate that our learning curve was levelling off after 25 cases.
Conclusions
Our initial 50 cases of retroperitoneoscopic live donor nephrectomy were performed without major complications. Compared with other published series, our donors were younger and a greater proportion were male, but warm ischaemic time, blood loss, operating time and hospitalisation were similar.
REFERENCES
1. Ratner LE, Ciseck LJ, Moore RG, et al. Laparoscopic live donor nephrectomy. Transplantation 1995;60(9):1047-1049. [ Links ]
2. Bachmann A, Wolff T, Ruszat R, et al. Retroperitoneoscopic donor nephrectomy: A retrospective, non-randomized comparison of early complications, donor and recipient outcome with the standard open approach. Eur Urol 2005;48(1):90-96. [http://dx.doi.org/10.1016/j.eururo.2005.03.007] [ Links ]
3. Ruszat R, Sulser T, Dickenmann M, et al. Retroperitoneoscopic donor nephrectomy: Donor outcome and complication rate in comparison with three different techniques. World J Urol 2006;24(1):113-117. [http://dx.doi.org/10.1007/s00345-006-0051-9] [ Links ]
4. Simforoosh N, Bassiri A, Ziaee SA, et al. Laparoscopic versus open live donor nephrectomy: The first randomized clinical trial. Transplant Proc 2003;35(7):2553-2554. [http://dx.doi.org/10.1016/j.transproceed.2003.08.062] [ Links ]
5. Schweitzer EJ, Wilson J, Jacobs S, et al. Increased rates of donation with laparoscopic donor nephrectomy. Ann Surg 2000;232(3):392-400. [http://dx.doi.org/10.1097/00000658-200009000-00011] [ Links ]
6. Greco F, Hoda MR, Alcaraz A, et al. Laparoscopic living-donor nephrectomy: Analysis of the existing literature. Eur Urol 2010;58(4):498-509. [http://dx.doi.org/10.1016/j.eururo.2010.04.003] [ Links ]
7. Abbou CC, Rabii R, Hoznek A, et al. [Nephrectomy in a living donor by retroperitoneal laparoscopy or lomboscopy]. Ann Urol (Paris) 2000;34(5):312-318. [ Links ]
8. Bachmann A, Wyler S, Wolff T, et al. Complications of retroperitoneoscopic living donor nephrectomy: Single center experience after 164 cases. World J Urol 2008;26(6):549-554. [http://dx.doi.org/10.1007/s00345-008-0296-6] [ Links ]
9. Ma L, Ye J, Tian X, et al. Technical modifications of retroperitoneoscopic live donor nephrectomy: Chinese experience. Transplant Proc 2010;42(9):3440-3443. [http://dx.doi.org/10.1016/j.transproceed.2010.08.068] [ Links ]
10. Tanabe K, Miyamoto N, Ishida H, et al. Retroperitoneoscopic live donor nephrectomy (RPLDN): Establishment and initial experience of RPLDN at a single center. Am J Transplant 2005;5(4):739-745. [http://dx.doi.org/10.1111/j.1600-6143.2004.00702.x] [ Links ]
11. Friedman AL, Peters TG, Jones KW, et al. Fatal and nonfatal hemorrhagic complications of living kidney donation. Ann Surg 2006;243(1):126-130. [http://dx.doi.org/10.1097/01.sla.0000193841.43474.ec] [ Links ]
12. Friedman AL, Peters TG, Ratner LE. Perioperative mortality and long-term survival in live kidney donors. JAMA 2010;303(22):2248-2249. [http://dx.doi.org/10.1111/j.1600-6143.2011.03918.x] [ Links ]
13. Friedman AL, Peters TG, Ratner LE. Regulatory failure contributing to deaths of live kidney donors. Am J Transplant 2012;12(4):829-834. [http://dx.doi.org/10.1111/j.1600-6143.2011.03918.x] [ Links ]
14. Simforoosh N, Aminsharifi A, Zand S, et al. How to improve the safety of polymer clips for vascular control during laparoscopic donor nephrectomy. J Endourol 2007;21(11):1319-1322. [http://dx.doi.org/10.1089/end.2007.0070] [ Links ]
15. Simforoosh N, Sarhangnejad R, Basiri A, et al. Vascular clips are safe and a great cost-effective technique for arterial and venous control in laparoscopic nephrectomy: Single-center experience with 1834 laparoscopic nephrectomies. J Endourol 2012;26(8):1009-1012. [http://dx.doi.org/10.1089/end.2007.0070] [ Links ]
16. Chan D, Bishoff JT, Ratner L, et al. Endovascular gastrointestinal stapler device malfunction during laparoscopic nephrectomy: Early recognition and management. J Urol 2000;164(2):319-321. [http://dx.doi.org/10.1016/S0022-5347(05)67349-1] [ Links ]
17. Deng DY, Meng MV, Nguyen HT, et al. Laparoscopic linear cutting stapler failure. Urology 2002;60(3):415-419. [http://dx.doi.org/10.1016/S0090-4295(02)01778-8] [ Links ]
18. Hoda MR, Greco F, Reichelt O, et al. Right-sided transperitoneal hand-assisted laparoscopic donor nephrectomy: Is there an issue with the renal vessels? J Endourol 2010;24(12):1947-1952. [http://dx.doi.org/10.1089/end.2010.0116] [ Links ]
19. Hoda MR, Greco F, Wagner S, et al. Prospective, nonrandomized comparison between right- and left-sided hand-assisted laparoscopic donor nephrectomy. Transplant Proc 2011;43(1):353-356. [http://dx.doi.org/10.1016/j.transproceed.2010.12.021] [ Links ]
20. Ng CS, Abreu SC, Abou El-Fettouh HI, et al. Right retroperitoneal versus left transperitoneal laparoscopic live donor nephrectomy. Urology 2004;63(5):857-861. [http://dx.doi.org/10.1016/j.urology.2003.12.027] [ Links ]
21. Gluecker TM, Mayr M, Schwarz J, et al. Comparison of CT angiography with MR angiography in the preoperative assessment of living kidney donors. Transplantation 2008;86(9):1249-1256. [http://dx.doi.org/10.1097/TP.0b013e3181890810] [ Links ]
 Correspondence:
Correspondence:
A van der Merwe
(arvdm@sun.ac.za)


{kind=link}
{kind=link}