










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.52 n.1 Cape Town Jan. 2014
TRAUMA
Severity of upper-limb panga injuries and infection rates associated with early v. late tendon repair
N HowardI; W J M HolmesII; C E PriceIII; P RollinsonIV
IMSc, MRCS (Edin); Orthopaedic Department, Ngwelezana Hospital, Empangeni, KwaZulu-Natal, South Africa
IIMRCS; Martin Singer Hand Unit, Groote Schuur Hospital, Cape Town, South Africa
IIIMB ChB; Martin Singer Hand Unit, Groote Schuur Hospital, Cape Town, South Africa
IVFRCS (Eng and Edin); Orthopaedic Department, Ngwelezana Hospital, Empangeni, KwaZulu-Natal, South Africa
ABSTRACT
BACKGROUND: Panga or machete attacks are a common cause of significant upper-limb trauma in South Africa. Pangas are a multipurpose household tool used predominantly for foraging and agricultural purposes and are highly contaminated. While some centres advocate immediate primary repair if no concern exists regarding the risk of infection, others delay definitive repair until satisfied there is no evidence of infection.
OBJECTIVES: To compare infection rates and tendon re-rupture following early primary repair (within 24 h), primary repair after 24 h, and delayed repair following initial debridement.
METHODS: We conducted a multicentre, retrospective, observational study of 49 patients (mean age 28.9 years; range 17 - 69), who were followed up for a mean of 3.4 months (range 0 - 8). The injuries sustained included 32 flexor tendon injuries, 14 extensor tendon injuries, 9 fractures and 21 peripheral nerve injuries.
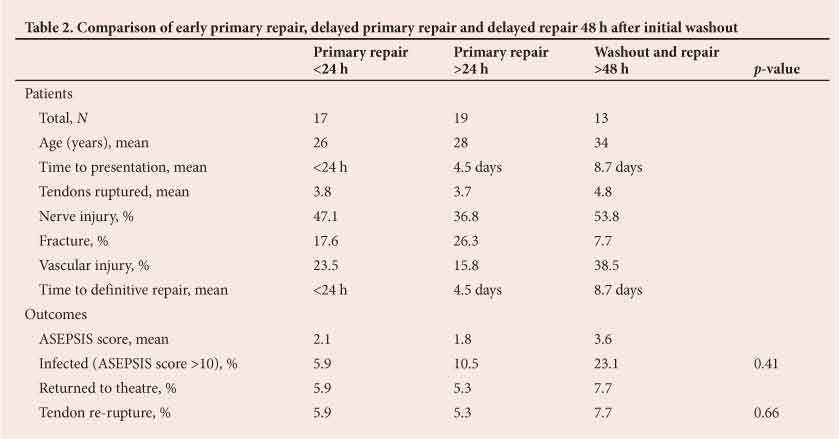
RESULTS: Of the patients, 17 underwent early primary repair (within 24 h), 19 delayed primary repair, and 13 delayed repair following primary washout. Wounds were assessed postoperatively using the ASEPSIS wound scoring system and patients were clinically assessed for tendon re-rupture. No significant differences were found in the comparative infection rates for early primary repair (5.9%; 1/17), delayed primary repair (10.5%; 2/19) and delayed repair following primary washout (23.1%; 3/13; p=0.662).
CONCLUSION: Our results indicate indicate that panga injuries can be repaired safely at first presentation with no increased risk of infection or re-rupture.
The panga is a variant of the machete used in east and southern Africa. Like the machete it has a long, broad, curved blade and is a multipurpose tool used for bush clearing and various other crude cutting tasks such as cutting wood. It is readily available with no legislation governing its acquisition.
Availability makes the panga a weapon commonly used in episodes of interpersonal violence. The type of injury sustained depends on the mechanism of injury. Stab-like injuries are inflicted using the end of the blade, while the back of the blade and the handle can be used as a blunt weapon. Injuries from blows with the long cutting edge of the blade are most frequently seen, and lacerations are often deep enough to transect tendons, nerves, blood vessels and bone, with amputations of digits and even limbs. A study from Nigeria found that upper-limb injuries accounted for 38% of all panga injuries.[1]
Only one paper has looked at the timing of repair of flexor tendon injuries in general and the use of antibiotics.[2] The authors concluded that repair of these injuries could be delayed beyond 12 h without increasing the likelihood of wound infection, and that antibiotics should be reserved for established infections and more serious hand injuries.
We aimed to delineate the pattern of panga injuries and compare infection rates in patients with early and delayed primary tendon repair v. debridement and delayed tendon repair (>24 h).
Methods
We conducted a prospective observational study in two South African hospitals, Ngwelezana Hospital in rural KwaZulu-Natal Province and Groote Schuur Hospital in central Cape Town. All patients who presented to hospital with panga injuries necessitating surgical intervention over a 10-month period were included.
We compared infection rates of injuries treated with primary washout and tendon repair v. primary washout and subsequent delayed repair after 48 h. Because delayed presentation of patients is so common in rural South Africa, even after serious injuries, the primary repair group was divided into two groups, those repaired within 24 h of injury and those repaired after 24 h, to investigate the effect this has on infection rates. Primary repair was carried out if the wounds assessed in theatre were not heavily contaminated. Wounds were washed and debrided, and a four-strand tendon repair was carried out on all ruptured tendons.
Inclusion criteria were: (i) isolated panga injury to the upper-limb, i.e. the anatomical territory from the glenohumeral joint to - the fingertip; and (ii) damage to a tendon, nerve or bone. Exclusion criteria were: (i) death; (ii) patients unable to attend for follow-up; and (iii) patients who discharged themselves without undergoing any medical treatment.
Data collection
For patients who fulfilled the inclusion criteria, age, gender, location of injury, associated injuries and time to presentation were recorded. The presence of fractures, nerve damage and tendon rupture and zone of tendon injury were also documented.
Treatment protocols
Patients who presented within 24 h with clean or clean-contaminated wounds were repaired primarily[3] at both centres. Patients who presented after 24 h with clean or clean-contaminated wounds at Ngwelezana Hospital were treated with washout, debridement and primary repair. Patients in the Martin Singer Hand Unit at Groote Schuur Hospital were treated with initial debridement, washout and closure. Wounds were reviewed at 48 h and delayed repair was undertaken unless there were signs of infection.
No patients included in the study had their management altered because of wound contamination at presentation. One patient who presented with an overtly infected wound was excluded from the study to make the groups comparable, as this patient would automatically have gone into the delayed repair group and been at increased risk of infection and tendon re-rupturing.
All patients were admitted and commenced on 1 g intravenous flucloxacillin four times a day until definitive repair had taken place. Postoperatively they were splinted, wounds were assessed at 48 h, and early limited mobilisation was commenced under the supervision of occupational therapists.
A prophylactic 5-day oral antibiotic regimen was given at both units with Gram-positive cover (500 mg flucloxacillin 4 times a day). Once satisfactory limited mobilisation was obtained, patients were discharged and followed up at a dedicated hand clinic.
Outcome measures
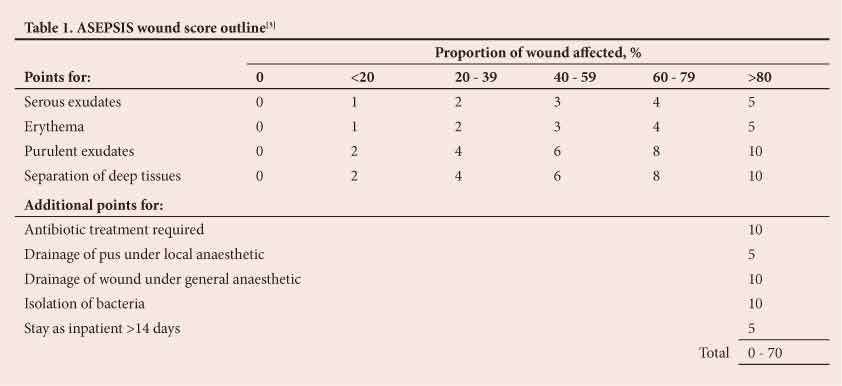
Patients were followed up at the hand clinics at 2, 4, 8 and 12 weeks. For each visit, infection was measured using the ASEPSIS score rating (Table 1) as recommended by the surgical infection study group.[3] The highest score was recorded for each patient and used as a single figure for statistical analysis. Wound swabs were taken and processed for culture and sensitivity if pus was present on clinical examination.
Tendon re-rupture was assessed clinically by hand therapists at each visit. Other complications were recorded during follow-up appointments as part of routine clinical care.
Results
The results are summarised in Table 2. Forty-nine patients with upper extremity panga injuries met the inclusion criteria. Of these, 91.8% (45/49) were male and 8.2% (4/49) female, and the mean age was 28.9 years (range 17 - 69 years). Of the injuries, 46 (93.9%) were caused by alleged assaults and three were accidental, and 69.4% of the patients (34/49) presented within 24 h, only 10.2% (5/49) presenting >48 h after injury. Only half of those who presented early were operated on within 24 h.
Of the patients, 44.9% (22/49) sustained lacerations to the hand, 30.6% (15/49) to the wrist and 24.5% (12/49) to the forearm. When assessed in theatre, 47/49 patients were found to have tendon injuries. These were flexor tendon injuries in 67.3% of the patients (33/49) and extensor tendon injuries in 28.6% (14/49). The mean number of tendon lacerations per patient was 4.1 (range 0 - 8). Peripheral nerve injuries were sustained by 44.9% of the patients (22/49) (13 median, 12 ulnar and five digital), and 18% (11/49) sustained concomitant fractures. The metacarpals were fractured most often (n=4), followed by the ulna (n=3), radius (n=2) and phalanges (n=2).
Infection rates were compared between patients who had early primary repair (within 24 h), those who had delayed primary repair (after 24 h) and those who had delayed repair following initial washout and debridement. An infected wound was regarded as one with an ASEPSIS score >10, as outlined in Table 1; however, the clinical action taken in these 'infected' cases varied, so a further analysis of those who had to return to theatre as a consequence of infection is included in Table 2. All patients with infection who did not return to theatre were successfully treated with oral antibiotics as outpatients. Of the three patients who needed to return to theatre after repair, two required multiple washouts and one an amputation.
Statistical analysis revealed there was no difference in infection rates between early primary repair, delayed primary repair and delayed repair following washout (Fisher's exact test p=0.662).
Four patients had evidence of pus on exploration and swabs were taken. A total of four cultures were positive from three patients; three were Gram-positive (Staphylococcus aureus), all sensitive to flucloxacillin, and one was Gram-negative (Enteroccocus faecalis) and sensitive to gentamicin.
Discussion
Panga injuries are a significant source of morbidity and mortality in many regions of the developing world, and no literature exists on the optimal management of these complicated injuries. Postoperative infections of the upper-limb can result in devastating consequences ranging from amputation to impaired long-term function and prolonged hospital stay.
Young men are the primary victims of panga assaults, as has been shown in previous machete injury studies worldwide.[4] The most common cause of these injuries, generally serious injuries to the upper limbs, is interpersonal violence.[5,6] The severe disability and morbidity associated with such injuries can have a drastic effect on a young person's future, especially in areas where manual labour is the most common form of employment.
The severity of panga injuries is highlighted by the fact that an average of four tendons per patient were repaired and nearly 45% of patients had a peripheral nerve injury. In a study comparing timing of repair and use of prophylactic antibiotics in flexor tendon repairs, <15% of patients had >2 tendons lacerated.[2]
Our results indicate that patients who undergo primary repair are at no greater risk of postoperative wound infection than those who have delayed repair following initial debridement. Delayed repair is considered in lacerations that are >24 h old or are heavily contaminated, because of the increased risk of wound infection and debilitation that can result. The increasing risk of wound infection with advancing wound age has been documented in the literature.[5,6] Stone and Davidson[2] questioned the necessity to repair flexor tendon injuries within a specific time, finding no difference in postoperative infection rates between injuries repaired before or after 12 h. Indeed, Schneider et al.[5] reported no infections in delayed repair of flexor tendons in 31 repairs ranging from 24 h to 21 days after injury. Our results in more contaminated and severe injuries support their findings. Although our two hospitals are tertiary referral centres, where late presentation is extremely common because they cover large areas, 69.4% of patients presented within 24 h and only 10.2% presented after 48 h. Our results and the relatively early presentation of these patients should give surgeons the confidence to repair panga injuries primarily after thorough initial debridement.
The benefits of early repair include reducing the number of theatre visits, decreasing hospital stay, and allowing earlier mobilisation after injury. This approach also reduces the tendon retraction seen in flexor tendon injuries and avoids the difficulties this causes when carrying out delayed repair.
Our overall infection rate of 12.2% was relatively high in comparison with the 6.75% reported in the paper on machete attacks in Nigeria by Omoke and Madubueze.[1] Inclusion criteria differ markedly between the two studies, however, with the Nigerian authors including all machete injuries, even relatively - minor superficial lacerations stitched in the emergency department. Outcome measures also differ, with no definition of infection included in their paper. Our higher infection rates may also be due to the relatively low threshold of infection used in accordance with the ASEPSIS wound score. Although an arbitrary figure of 10 was used, this gave us a relatively objective and sensitive indicator of infection. If we defined infection as a return to theatre for management of acute wound sepsis, the infection rate would be recalculated as 6.1%.
Study limitations
The limitations of our study include the fact that patients were recruited from two different centres, which could introduce bias even though comparative management protocols were carried out. Functional outcomes following surgery could also be looked at in relation to timing of surgical repair.
Conclusion
Our results indicate that panga injuries can be repaired safely at first presentation with no increased risk of infection or re-rupture. With the lack of published articles on these common injuries, there is great scope for further research. The use of prophylactic antibiotics remains controversial, especially in injuries without open fractures.
REFERENCES
1. Omoke NI, Madubueze CC. Machete injuries as seen in a Nigerian teaching hospital. Injury 2010;41(1):120-124. [http://dx.doi.org/10.1016/j.injury.2009.08.023] [ Links ]
2. Stone JF, Davidson JS. The role of antibiotics and timing of repair in flexor tendon injuries of the hand. Ann Plast Surg 1998;40(1):7-13. [http://dx.doi.org/10.1097/00000637-199801000-00002] [ Links ]
3. Wilson AP, Treasure T, Sturridge MF, Grueneburg RN. A scoring method (ASEPSIS) for postoperative wound infections for use in clinical trials of antibiotic prophylaxis. Lancet 1986;327(8476):311-313. [http://dx.doi.org/10.1016/S0140-6736(86)90838-X] [ Links ]
4. Yip KM, Tam TY, Hung LK. Multiple chop wound in Hong Kong. Arch Orthop Trauma Surg 1997;116(5):295-298. [http://dx.doi.org/10.1007/BF00390057] [ Links ]
5. Nylen S, Carlsson B. Time factor, infection frequency and quantative microbiology: Its application to hand injuries. Scand J Plast Reconstr Surg1980;14(2):185-189. [ Links ]
6. Schneider LH, Hunter JM, Norris TR, Nadeau PD. Delayed flexor tendon repair in no man's land. J Hand Surg 1977;2(6):452-455. [ Links ]
 Corresponding author:
Corresponding author:
N Howard
(nick.howard@doctors.org.uk)


{kind=link}
{kind=link}